
Abstract
Background
The purpose of the present study was to examine the relationship between cognitive impairment and the performance of handwritten scripts presented as “letter-writing” to a close relative by patients with dementia Lewy bodies (DLB), as fluctuations of the symptoms phase, and in a matched group of patients with Alzheimer’s disease (AD). The degree of writing disability and personal, spatial, and temporal orientation was compared in these two groups.
Design and methods
Fourteen simple questions, designed in a form that could be utilized by any general practitioner in order to document the level of cognitive functioning of each patient, were presented to 30 AD patients and 26 DLB patients. The initial cognition test was designated PQ1. The patients were examined on tests of letter-writing ability. Directly after the letter-writing, the list of 14 questions presented in PQ1 was presented again in a repeated procedure that was designated PQ2. The difference between these two measures (PQ1 – PQ2) was designated DΔ. This test of letter-writing ability and cognitive performance was administered over 19 days.
Results
Several markedly strong relationships between dysgraphia and several measures of cognitive performance in AD patients and DLB patients were observed, but the deterioration of performance from PQ1 to PQ2 over all test days were markedly significant in AD patients and not significant in DLB patients. It is possible that in graphic expression even by patients diagnosed with moderate to relatively severe AD and DLB there remains some residual capacity for understanding and intention that may be expressed. Furthermore, the deterioration in performance and the differences noted in AD and DLB patients may be due to the different speed at which the process of the protein degradation occurs for functional modification of synapses.
Conclusion
Our method can be used as part of neuropsychological tests to differentiate the diagnosis between AD and DLB.
Introduction
In Western industrial nations, Alzheimer’s disease (AD) represents the most common form of dementia,Citation1,Citation2 at approximately 80%,Citation3 occupying fourth place among the causes of death (after heart disease and circulatory disorders, cancer, and cerebral hemorrhage). Dementia with Lewy bodies (DLB) is the second most common cause of degenerative dementia after AD.
Worldwide there are currently 25 to 35 million individuals with these illnesses, with five to seven million new cases diagnosed each year, or one new case every 7 seconds.Citation4,Citation5 According to the World Health Organization it has been estimated that by the year 2050 the number of people presenting with dementia will be 115.4 million.Citation6
The pathology of dementia is associated with memory loss, loss of orientation, inability to focus attention, and loss of speech. In addition, we notice cognitive fluctuations, defined as spontaneous alterations in cognition, attention, and arousal. Fluctuating confusion, accompanied by disturbances of consciousness, is an important clinical symptom, with a frequency of 80%–90% in DLBCitation7,Citation8 and 20% in Alzheimer’s disease.Citation9 In fact, in these patients, cognitive fluctuations and periods of behavioral confusion, inattention, and alternating episodes of lucidity and capable task performance have been described.Citation10 McKeith identified the “marked amplitude between best and worst performance” as a distinguishing feature of the fluctuations in cognition and consciousness in DLB, contrasting this with “minor day-to-day variations” that can occur in dementia of any cause.Citation11 The term cognitive fluctuation remains elusive despite several attempts to identify, quantify, and assess the phenomenon.Citation12
This fact raises an important question: do the fluctuations occurring in AD patients have a particular quality and specific characteristics different from fluctuations that occur in DLB dementia?
In addition, many authors have observed in patients with AD dementia, a progressive disorganization and degeneration of the various components of handwriting, the diversity and the accuracy of words used, organization,Citation13 punctuation,Citation14 the production of grammatically incorrect sentences, the length of the sentences, the morphology of the letters,Citation15 the amount of written information,Citation16 spelling,Citation17 and graphic and spatial layout of letters and their arrangement in texts.Citation18
We are not aware of research regarding the degeneration of handwriting in DLB patients. The purpose of the present study was to examine the relationship between cognitive impairment and the performance of handwritten scripts presented as “letter-writing” to a close relative by AD patients, as fluctuations of the symptoms phase, and in a matched group of DLB patients.
Also, it is possible that in graphic expression even by patients diagnosed with moderate to relatively severe AD and DLB there remains some residual capacity for understanding and intention that may be expressed. Concurrently, the relationship between measures of functioning, Mini-Mental State Examination (MMSE), and number of years elapsed since first indication of disorder with dysgraphia and assessments of cognitive performance was assessed (or debut).
Materials and methods
Fifty-six patients (from the region of Lazio, Italy) were selected to participate in the study: 30 patients presenting AD and 26 patients presenting DLB. Patients were diagnosed according to the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders AssociationCitation19 and the Diagnostic and Statistical Manual of Mental Disorders, 4th edition reference.
In addition, a group of 30 younger, less impaired AD patients (ADli) was included. Patients were excluded if they presented a history of known or suspected cerebrovascular disease, focal neurological signs or brain imaging evidence for alcohol misuse, head trauma, significant psychiatric history preceding the current diagnosis, or any other major physical illness. All of these diagnoses were confirmed and verified by neurologists in the Department of Neurology at the hospital (Gemelli University Polyclinic – service neuropsychology, Roma and the Alzheimer Evaluation Unit ASLRMF and Alzheimer Evaluation Unit ASLRMD); 26 patients were confirmed by the Department of Neurology and Psychiatry, Sapienza Hospital, Rome, Italy, in the Lazio region. Only subjects with the clinical follow-up and complete diagnostic agreement by the three neurologists were included.
A considerable amount of time (regular meetings every second day for 3 months) was invested in each of the patients in order to promote a relationship of trust and understanding, as well as to reduce stress factorsCitation20 that may affect patients’ mood and attentiveness, or, more seriously, induce behaviors that suggest hallucinations or auditory illusions, paranoid delirium, difficulty in recognizing persons, or loss of cognition of time and place. All the procedures were adopted according to discussions and meetings with nearest relatives and caregivers in order to obtain the consent of the patients as well as those of relatives and caregivers (caregivers could be legal representatives) according to the legal practices.
Alzheimer’s disease
For the sixty patients constituting the AD group and ADli, the diagnosis was based on normal or nonspecific electroencephalography and lateral, occipital brain atrophy on magnetic resonance imaging or computed tomography brain scan, with documented progression after serial observations, and on cognitive test procedures and routine blood assays aimed at excluding the presence of other medical conditions associated with other types of dementia.
Dementia with Lewy bodies
Twenty-six DLB patients were included in the study. Diagnosis was confirmed using the international consensus guidelines for DLB, revised in 2005.Citation21 All patients presented with dementia at the time of their initial evaluation, which usually preceded the onset of motor signs of disorder by 1–2 years. Some patients exhibited cognitive impairment concomitant with mild extrapyramidal signs, which, however, never reached the criteria levels for the diagnosis of idiopathic Parkinson’s disease, and showed no evidence of focal brain lesions on magnetic resonance imaging.
Exclusion criteria were presence of secondary, reversible causes of dementia that were untreated; concomitant neurological or psychiatric illness, substance use and abuse; and history of significant head trauma.
Mini-Mental State Examination
MMSE presents a brief 30-point questionnaire to screen for cognitive impairment and dementia.Citation22 It estimates the severity of disorder and follows the course over time of cognitive changes in an individual, thereby allowing effective monitoring of an individual’s response to treatment.
Unified Parkinson’s Disease Rating Scale
The Unified Parkinson’s Disease Rating Scale is a rating scale used to follow the longitudinal course of Parkinson’s disease.Citation23 It is the most commonly used scale in the clinical study of Parkinson’s disease and of DLB.
Clinician assessment of fluctuation (CAF)
CAF is a short scale consisting of a series of screening questions, regarding fluctuating confusion and impaired consciousness during the month prior to the assessment. The frequency and duration of episodes of fluctuating confusion are both rated on a scale of 0–12 (0 representing no fluctuating confusion, 12 representing severe fluctuating confusion).Citation24
Cognitive performance assessment
Testing material
A writing pad was used for writing text or drawing figures. Preferably the tablet was vergatina type (flimsy typing paper, tissue type, or absorbent in order to avoid false interpretations of the writings). A ballpoint pen was used throughout. The patients were invited to sit in a comfortable position.
Procedure
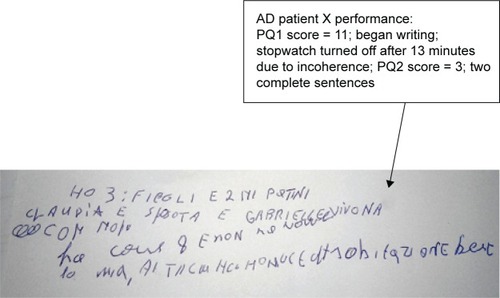
In order to test the cognitive performance of AD patients and DLB patients as well as test their spatial and time orientation and residual capacity, a standard collection of 14 simple questions were presented to the patients (). The authors have designed and presented these questions in a form that could be utilized by any general practitioner in order to document the level of cognitive functioning of each patient. For each correct answer, one point was attributed in proportion to the difficulty of the question.Citation25 The sum of each test session was represented by PQ; the initial session result was designated PQ1. Following this, each patient was then invited to write a letter to a close relative. On consecutive days of testing, patients were invited to write to either the same relative or another one. The letter-writing task was interrupted when it seemed that the text produced by the patient was substantially (pathologically) confused (when the phrase offered no conceptual association with accompanying text although in the presence of otherwise “correct” syntax) and when it had a sudden lack of readability, disjointedness, and incompleteness in meaning, with intrusions, semantic substitutions, alterations in the spatial organization of handwriting, illegible words, incidence of paraphrases, incapacity to form complete sentences, graphemic substitutions (a grapheme is the smallest semantically distinguishing unit in a written language), omissions, and additions. After this, using a chronometer, the number of minutes that had been reached for each single patient was registered and complete sentences were counted (sentences/minutes = XF). The whole procedure involving the letter-writing graphia task was interrupted after 20 minutes (see ).
Table 1 Example scoring list of 14 questions presented to a hypothetical AD patient in PQ1 phase and PQ2 phase. These are routine questions which a doctor can ask to the patient
Figure 1 The performance of AD patient X and DLB patient X during PQ1, followed by the letter-writing test, followed by PQ2.
Abbreviations: AD, Alzheimer’s disease; DLB, dementia Lewy bodies; PQ1, initial cognition test; PQ2, repeated cognition test.
Directly after letter-writing
The list of 14 questions presented in PQ1 was presented again in a repeated procedure that was designated PQ2. The difference between these two measures (PQ1 – PQ2) was designated DΔ. These procedures for testing: 14-item test, graphia test, 14-item test were presented in an identical manner every second day over 10 days (days 1, 3, 5, 7, 9, 11, 13, 15, 17, and 19) at the same hour of day on test days in order to hold constant testing procedures over daily curriculum and any clinical interventions that the patients may be subject to.
Statistical analysis
The results consisting of PQ1 and PQ2 scores, XF, and DΔ were calculated as means and standard deviations of the AD patient group and the DLB patients over consecutive days of testing. Pearson’s correlation coefficient was used to assess the relationship between XF and PQ1 and XF and DΔ for both AD patients and DLB patients for each of the test days. Student’s t-tests were used to test for pairwise differences for each of the parameters.
Results
The clinical characteristics of the participants in the study are presented in .
Table 2 Clinical, demographic, and neuropsychological data of the study groups
AD, ADli, and DLB patients: cognitive performance over PQ1 and PQ2
The cognitive performance of the AD patients and DLB patients deteriorated from PQ1 to PQ2 (), with t-values reaching significance levels over all 10 days of testing.
Table 3 The Student’s t-test values between PQ1 and PQ2 scores (means ± SD) and Pearson product moment correlational analyses between 1) PQ1 and XF, 2) XF and D∆ over 10 days of testing (days 1, 3, 5, 7, 9, 11, 13, 15, 17, and 19)
The cognitive performance of ADli patients deteriorated from PQ1 to PQ2 ().
Table 4 Younger, less impaired AD patient Student’s t-test values between PQ1 and PQ2 scores (means ± SD) and Pearson product moment correlational analyses between 1) PQ1 and XF, 2) XF and DΔ over 10 days of testing (days 1, 3, 5, 7, 9, 11, 13, 15, 17, and 19)
Comparison of AD, ADli with DLB patients: correlation coefficients PQ1 versus XF and XF versus DΔ
The correlation coefficients of both the PQ1 performance and XF relationship and the XF and DΔ relationship were all positive and highly significant in AD patients while they were positive in ADli patients. In DLB patients the correlation coefficient of the PQ1 performance and XF relationship was positive while the correlation analysis of the XF and DΔ relationship was negative ( and ).
Correlation analyses between functional measures
Product moment correlations between the functional estimations of MMSE, debut (years), PQ1, DΔ, and PQ2 were carried out on the data obtained from the 30 AD patients and 26 DLB patients. It was observed that 1) MMSE is correlated significantly with PQ1, XF, and PQ2, 2) MMSE is correlated significantly with DΔ in AD patient while the correlation is negative in DLB patients, and 3) debut (years) does not correlated with PQ1, XF, PQ2, and DΔ in AD patient while the correlations are not significant in DLB patients ().
Table 5 Pearson product moment correlations analyses between MMSE, debut (years), PQ1, XF, PQ2, and DΔ in the 30 AD patients and 26 DLB patients
Comparison AD patients with DLB patients
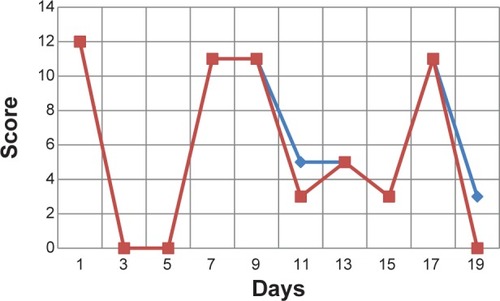
The cognitive impairment that occurs after the write performance in AD patients is clearly shown in . The blue plot shows the levels of cognitive impairment that occurred before the writing performance in AD and DLB patients (over 10 days of testing) day after day. The red plot emphasizes the cognitive level after the writing test ( and ).
Figure 2 Examples of cognitive impairment: AD patient scores for ♦PQ1 (before writing) and ■PQ2 (after writing).
Abbreviations: AD, Alzheimer’s disease; PQ1, initial cognition test; PQ2, repeated cognition test.
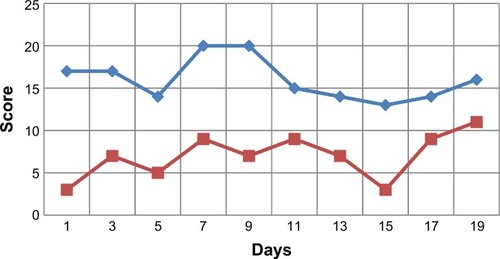
Figure 3 Examples of cognitive impairment: DLB patient scores for ♦PQ1 (before writing) and ■PQ2 (after writing).
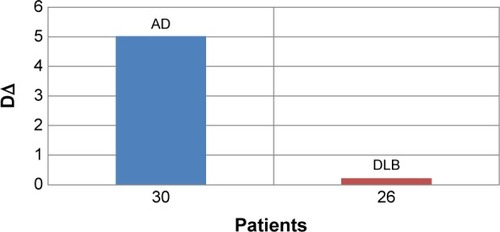
Concurrently, the extent of cognitive performance deterioration; DΔ from the 1st to the 2nd test was found to be markedly advanced in AD patients in comparison with the DLB patients ().
Figure 4 The difference (DΔ) between cognitive performance in PQ1 and PQ2 by AD patients and DLB patients expressed as DΔ means summated over all 10 days of testing.
Abbreviations: AD, Alzheimer’s disease; DLB, dementia Lewy bodies; PQ1, initial cognition test; PQ2, repeated cognition test.
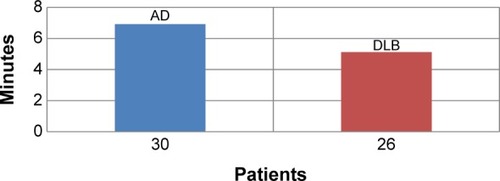
The extent of dysgraphia by the DLB patients was found to be quite advanced in comparison with the AD patients ().
Figure 5 The amount of time spent writing clearly by AD patients and DLB patients expressed as means in the graphia test summated over all 12 days of testing.
Abbreviations: AD, Alzheimer’s disease; DLB, dementia Lewy bodies.
Discussion
This study shows the distinctive features of the cognitive impairment in relation to dysgraphia during the cognitive daily fluctuations in DLB patients and in AD patients.
The cognitive impairment, spontaneous alterations in attention, and incoherent speech, alternating with episodes of lucidity and capable task performance are a recognized feature of dementia, especially in DLB, but they are present also in AD.
We examined the relationships between initial cognitive performance (PQ1), the deterioration in cognitive performance following a letter-writing task (PQ1 – PQ2 = DΔ) and dysgraphia (XF) in a group of AD patients presenting a moderate to relatively severe stage of disorder, and comparisons with a group of DLB patients and with ADli patients. The results may be summarized as follows: 1) the relationships between initial cognitive performance (PQ1) and extent and dysgraphia over both AD and DLB patients and test days were markedly strong; 2) but the deterioration of performance from PQ1 to PQ2 over all test days was markedly significant in AD patients, and it was not significant in DLB patients; 3) the relationships between dysgraphia and cognitive deterioration (DΔ) were also markedly strong in AD patients, and they were not significant in DLB patients; 4) MMSE correlated significantly with PQ1, PQ2, and with XF in both groups of patients; furthermore, number of years elapsed since first diagnosis of disorder does not affect the XF (or expression of dysgraphia), PQ1, PQ2, and DΔ. In particular, the nonassociation between MMSE and DΔ in DLB patients was markedly significant (R2= −0.185).
Dysgraphia occurs during both the earlier as well as the later stages during the clinical course of ADCitation26–Citation28 and is associated with attentional, motor, and memory deficits that develop during disorder progression.Citation29 It has been suggested to be a more sensitive indication of language deficits in AD than anomia.Citation30,Citation31 Some authorsCitation32 have observed that the medial walls of the cerebral hemispheres, notably the cingulate gyri, contain species-specific neuron fields that to date are not well known within the scientific community and yet have been implicated as the underlying cause of such varying conditions as dysgraphia and autism in children and obsessive compulsive disorder and AD in adults.Citation33
In a sample of 52 Japanese patients presenting mild AD and 22 healthy controls, writing ability composed of Kana writing-to-dictation and copying Kanji or dictational Kanji and regional cerebral blood flow using single-photon emission computed tomography were studied.Citation34 Hayashi et al observed that while Kana writing-to-dictation and copying Kanji were preserved in these AD patients, writing to dictated Kanji words was impaired. The impaired writing of dictated Kanji words was associated with dysfunctional cortical activity, predominantly in the left frontal, parietal, and temporal brain regions, consistent with other Japanese dysgraphia studies.Citation35,Citation36
Furthermore, clear differences between AD patients and healthy control individuals have been found for visuomotor task measures, demonstrating large effect size deficits by AD patients, especially with visuomotor task progression through its varying conditions.Citation37,Citation38 They have observed dysgraphia, primarily dysexecutive agraphia, in patients with frontotemporal dementia and parkinsonism linked to chromosome 17. Patients presenting dysexecutive agraphia show not only difficulties in maintaining the effort inherent to writing but appear to lack the ability to organize their thoughts for expression in written text. They seem to be lacking in the complicated functions underlying writing that encompass narrative coherence, selective attention, planning, etc that are disturbed in executive function impairments.
The present observations of dysgraphia associated with deficits in semantic memory that were exacerbated acutely by the writing task appear to fit current notions pertaining to the progressive performance impairments of AD patients within language and cognition domains from a staging perspective.Citation39
The possible relationships between dysgraphia and the motor functioning domain in AD has provided novel insights into the cognitive nature of the disorder,Citation40 through which mild to moderate stage AD patients (n=59) and healthy elderly controls were tested over an extensive assessment of both the central and peripheral components of writing; the former performed less effectively than controls over a broad spectrum of writing measures. Although a predominantly lexical disorder was observed, there were multiple indications of associated disorders located at different stages in the writing/spelling system (eg, phonological route, graphemic buffer, allographic store, graphic motor patterns). The authors concluded that there exists heterogeneous profiles of dysgraphia with primary signs of writing impairment in AD originating from changes at different points in the brain networks that subserve writing and spelling performance.Citation40 In this regard, the possibility of related motor deficits in dysgraphia ought to be considered since there is evidence for altered parietal-motor connections in AD.Citation41 It has been found too that sensory-motor plasticity is impaired in the motor cortex of AD at an early stage of the disease.Citation42
Several have indicated that agraphia is related to severity of AD disorder.Citation17,Citation43,Citation44 Hughes et alCitation26 have demonstrated the relationships between extent of MMSE impairment and patterns of agraphia in AD. MMSE deficits in AD are linked to several comorbidity domains, including cardiovascular, ear, nose and throat, genitourinary, musculoskeletal/integument, and neurologic.
We are not aware of studies that have examined the relationship between cognition and dysgraphia in DLB patients, nor of studies that have compared the cognitive impairment after writing between AD and DLB. Much of the current knowledge regarding the relationship between DLB and AD dementia and cognition is derived from clinical–pathological studies of atypical cases of dementia and specialty clinic samples.Citation45,Citation46 For instance clinic-based studies have shown that cortical Lewy body pathology is associated with more rapid decline in cognition;Citation7,Citation47 however, this has not been noted in all studies.Citation48,Citation49
Cognitive fluctuations that occur in patients cannot be caused by sudden loss or gain of nerve cells;Citation50 recent evidence suggests that variations in the activity of neural networks, and the neural plasticity is mediated by morphological and functional modification of synapses, a process that depends on both synthesis and degradation of proteins,Citation51 events targeting a variety of molecules in pre- and postsynaptic compartments.Citation52
This study, by analyzing relationships between initial cognitive performance (PQ1), the deterioration in cognitive performance following a letter-writing task (PQ1 – PQ2 = DΔ), and dysgraphia in AD and DLB patients, suggests that cognitive fluctuations that occur in patients with AD during the performance of handwritten scripts are not present in patients with DLB. During the observation period, the DLB patients have fluctuating confusion, inattention that is independent from the fatigue of the writing task.
May the differences noted in AD and DLB patients be due to the different speed at which the process of the protein degradation occurs? Is it the recovery of cognition in AD and DLB patients allowed to the influence of protein degradation in relation to temporal dynamics in other regions of the brain? The current study has a limitation: cognitive fluctuation was measured on majority of change in orientation, not other cognitive domains, approximately 20 minutes apart.
Conclusion
Our results can provide new insights into the mechanism of cognitive decline in AD and DLB patients and may be useful to develop a method based on dysgraphia in order to differentiate the diagnosis of both types of dementia. In particular, the writing, in association with the cognitive questionnaire, can be used as part of neuropsychological tests to diagnose the difference between AD and DLB.
Disclosure
The authors report no conflicts of interest in this work.
References
- FratiglioniLLaunerLJAndersenKIncidence of dementia and major subtypes in Europe: a collaborative study of population base cohorts. Neurologic Diseases in the Elderly Research GroupNeurology20005411 Suppl 5S10S1510854355
- LoboALaunerLJFratiglioniLPrevalence of dementia and major subtypes in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in the Elderly Research GroupNeurology20005411 Suppl 5S4S910854354
- TijmsBMMöllerCVrenkenHSingle-subject grey matter graphs in Alzheimer’s diseasePLoS One201383e5892123536835
- FerriCPPrinceMBrayneCAlzheimer’s Disease InternationalGlobal prevalence of dementia: a Delphi consensus studyLancet200536695032112211716360788
- RavagliaGFortiPDe RonchiDPrevalence and severity of dementia among northern Italian centenariansNeurology199953241641810430440
- World Health OrganizationDementia a public health priority [webpage on the Internet]GenevaWorld Health Organization2012 Available from: http://www.who.int/mental_health/publications/dementia_report_2012/en/
- ByrneEJLennoxGLoweJGodwin-AustenRBDiffuse Lewy body disease: clinical features in 15 casesJ Neurol Neurosurg Psychiatry19895267097172545827
- McKeithIGGalaskoDKosakaKConsensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshopNeurology1996475111311248909416
- KolbeinssonHJónssonADelirium and dementia in acute medical admissions of elderly patients in IcelandActa Psychiatr Scand19938721231278447239
- BradshawJSalingMHopwoodMAndersonVBrodtmannAFluctuating cognition in dementia with Lewy bodies and Alzheimer’s disease is qualitatively distinctJ Neurol Neurosurg Psychiatry200475338238714966152
- McKeithIGDementia with Lewy bodiesBr J Psychiatry200018014414711823325
- LeeDRTaylorJPThomasAJAssessment of cognitive fluctuation in dementia: a systematic review of the literatureInt J Geriatr Psychiatry2012271098999822278997
- HornerJHeymanADawsonDRogersHThe relationship of agraphia to the severity of dementia in Alzheimer’s diseaseArch Neurol19884577607633390031
- LaBargeESmithDSDickLStorandtMAgraphia in dementia of the Alzheimer typeArch Neurol19924911115111561444882
- HendersonVWBuckwalterJGSobelEFreedDMDizMMThe agraphia of Alzheimer’s diseaseNeurology19924247777841565231
- CroisileBCarmoiTAdeleinePTrilletMSpelling in Alzheimer’s diseaseBehav Neurol19958135143
- NeilsJRoeltgenDPGreerASpelling and attention in early Alzheimer’s disease: evidence for impairment of the graphemic bufferBrain Lang19954932412627640965
- RoeltgenDPAgraphiaHeilmanKMValensteinEClinical Neuropsychology4thNew York, NYOxford University Press2003126145
- McKhannGDrachmanDFolsteinMKatzmanRPriceDStadlanEMClinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s DiseaseNeurology19843479399446610841
- RicciSFusoAIppolitiFBusinaroRStress-induced cytokines and neuronal dysfunction in Alzheimer’s diseaseJ Alzheimers Dis2012281112422124029
- McKeithIGDicksonDWLoweJConsortium on DLBDiagnosis and management of dementia with Lewy bodies: third report of the DLB ConsortiumNeurology200565121863187216237129
- FolsteinMFFolsteinSEMcHughPR“Mini-mental state”. A practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res19751231891981202204
- Martínez-MartinPGil-NagelAGraciaLMGómezJBMartínez-SarriésJBermejoFUnified Parkinson’s Disease Rating Scale characteristics and structure. The Cooperative Multicentric GroupMov Disord19949176838139608
- WalkerMPAyreGACummingsJLThe Clinician Assessment of Fluctuation and the One Day Fluctuation Assessment Scale. Two methods to assess fluctuating confusion in dementiaBr J Psychiatry200017725225611040887
- OnofriEMercuriMSalesiMRicciardiMRArcherTRicciSCognitive performance deficits and dysgraphia in Alzheimer’s disease patientsJ Neurol Neurophysiol20145223
- HughesJCGrahamNPattersonKHodgesJRDysgraphia in mild dementia of Alzheimer’s typeNeuropsychologia19973545335459106281
- SmallJASandhuNEpisodic and semantic memory influences on picture naming in Alzheimer’s diseaseBrain Lang200810411917223189
- YasudaKNakamuraTBeckmanBBrain processing of proper namesAphasiology2000141110671089
- SilveriMCCordaFDi NardoMCentral and peripheral aspects of writing disorders in Alzheimer’s diseaseJ Clin Exp Neuropsychol200729217918617365253
- CroisileBSkaBBrabantMJComparative study of oral and written picture description in patients with Alzheimer’s diseaseBrain Lang19965311198722896
- YoonJHSuhMKJeongYAgraphia in Korean patients with early onset Alzheimer’s diseaseInt Psychogeriatr20112381317132621615977
- PaucRYoungALittle-known neurons of the medial wall: a literature review of pyramidal cells of the cingulate gyrusJ Chiropr Med20109311512022027033
- AllmanJMHakeemAErwinJMNimchinskyEHofPThe anterior cingulate cortex. The evolution of an interface between emotion and cognitionAnn N Y Acad Sci200193510711711411161
- HayashiANomuraHMochizukiRNeural substrates for writing impairments in Japanese patients with mild Alzheimer’s disease: a SPECT studyNeuropsychologia20114971962196821439989
- SakuraiYMimuraIMannenTAgraphia for kanji resulting from a left posterior middle temporal gyrus lesionBehav Neurol20081939310618641429
- YaguchiHYaguchiMBandoMA case of pure agraphia due to left parietal lobe infarctionNo To Shinkei20065810885892 Japanese17087281
- TippettWJSergioLEBlackSECompromised visually guided motor control in individuals with Alzheimer’s disease: can reliable distinctions be observed?J Clin Neurosci201219565566022459181
- SitekEJNarozanskaEBarczakAAgraphia in patients with frontotemporal dementia and parkinsonism linked to chromosome 17 with P301L MAPT mutation: dysexecutive, aphasic, apraxic or spatial phenomenon?Neurocase2014201698623121543
- ArcherTKostrzewaRMStaging neurological disorders: expressions of cognitive and motor disorderNeurotox Res201018210711119941173
- LambertJGiffardBNoreFde la SayetteVPasquierFEustacheFCentral and peripheral agraphia in Alzheimer’s disease: from the case of Auguste D. to a cognitive neuropsychology approachCortex200743793595117941351
- BonnìSLupoFLo GerfoEAltered parietal-motor connections in Alzheimer’s disease patientsJ Alzheimers Dis201333252553323001709
- TerranovaCCarmenTSantAngeloAImpairment of sensory-motor plasticity in mild Alzheimer’s diseaseBrain Stimul201361626622476006
- PlatelHLambertJEustacheFCharacteristics and evolution of writing impairment in Alzheimer’s diseaseNeuropsychologia19933111114711588107977
- RapcsakSZArthurSABliklenDARubensABLexical agraphia in Alzheimer’s diseaseArch Neurol198946165682910263
- HansenLSalmonDGalaskoDThe Lewy body variant of Alzheimer’s disease: a clinical and pathologic entityNeurology1990401182153271
- HamiltonJMSalmonDPGalaskoDVisuospatial deficits predict rate of cognitive decline in autopsy-verified dementia with Lewy bodiesNeuropsychology200822672973718999346
- GalaskoDRGouldRLAbramsonISSalmonDPMeasuring cognitive change in a cohort of patients with Alzheimer’s diseaseStat Med20001911–121421143210844707
- HanyuHSatoTHiraoKKanetakaHSakuraiHIwamotoTDifferences in clinical course between dementia with Lewy bodies and Alzheimer’s diseaseEur J Neurol200916221221719146642
- WalkerZMcKeithIRoddaJComparison of cognitive decline between dementia with Lewy bodies and Alzheimer’s disease: a cohort studyBMJ Open20122e000380
- PalopJJChinJMuckeLA network dysfunction perspective on neurodegenerative diseasesNature2006443711376877317051202
- BingolBShengMDeconstruction for reconstruction: the role of proteolysis in neural plasticity and diseaseNeuron2011691223221220096
- YiJJEhlersMDEmerging roles for ubiquitin and protein degradation in neuronal functionPharmacol Rev2007591143917329546