
Abstract
Purpose
The purpose of this study was to explore the effects of an innovative momentum-based dumbbell-training intervention on cognitive function in older adults with mild cognitive impairment (MCI).
Subjects and methods
A total of 45 community-dwelling older adults with MCI were randomly assigned to either a dumbbell-training group (DTG; n=22) or a control group (CG; n=23). Participants in the DTG participated in exercise sessions three times weekly for 12 weeks. The primary outcome measures were cognitive function, including the Alzheimer’s Disease Assessment Scale (ADAS) – Cognitive subscale, Trail Making Test part B, Digit Span Test (DST) – forward, and DST – backward, with secondary outcome measures being Timed Up and Go, functional reach, and the Activities-Specific Balance Confidence Scale.
Results
In an intent-to-treat analysis, participants in the DTG had significantly improved ADAS – Cognitive subscale scores compared to those in the CG (5.02 points, P=0.012). There was a significant within-group change (improvement) in Trail Making Test part B (33.32 seconds, P<0.001) and DST – backward (0.41 points, P=0.025) scores. No change was observed for the DST – forward measure. Participants in the DTG also improved their functional mobility compared to those in the CG (Timed Up and Go, 0.81 seconds; P=0.043).
Conclusion
There is preliminary evidence showing the potential benefit of momentum-based dumbbell training for improving cognitive function in older adults with MCI.
Introduction
With the escalation of the aging population worldwide, dementia has become a major public health concern. In 2010, the number of older adults worldwide living with dementia was estimated to be 35.6 million; the number is expected to double by 2030 and more than triple by 2050.Citation1 In the People’s Republic of China (PRC), 6–7 million people live with dementia, with an incidence rate between 5% and 7% for people 65 years of age and older.Citation2
Alzheimer’s disease (AD) is the most common form of dementia, accounting for 60%–70% of cases. If the disease onset could be delayed by 12 months, there would be 9.2 million fewer cases of AD.Citation3 Therefore, early diagnosis and treatment are becoming critically important in order to reduce the prevalence of dementia in the elderly. Mild cognitive impairment (MCI) is a transitional state between healthy aging and dementia.Citation4 Elderly individuals with MCI are at higher risk for developing AD, with estimates ranging from 10% to 15% annually, while this rate among normal elderly individuals is only 1%–2%.Citation4
Given that no effective pharmacological treatment exists for individuals with MCI to alter or slow the progression of cognitive decline,Citation5–Citation7 there has been growing interest in adopting lifestyle-change approaches, such as exercise, to prevent and/or reduce risk of developing dementia. Observational studies have shown that people who have MCI but are physically active tend to have slower cognitive decline and slower progression to dementia in later life.Citation8–Citation12 Randomized controlled studies have demonstrated that exercise or physical activity (eg, aerobic exercise, resistance training, multimodal exercises) may well provide cognitive benefits, including improved global cognitive function, executive function, memory, attention,Citation13–Citation15 and brain healthCitation16,Citation17 to older adults with cognitive disorders. Therefore, exercise has many health benefits that positively impact cognitive function and reduce vascular risks for developing dementia.Citation18
In this proof-of-concept study, we explored whether a momentum-based dumbbell-training intervention would improve cognitive function in older adults with MCI. Momentum-based dumbbell training is a self-initiated spinning exercise that uses dumbbells to generate momentum while performing exercise movements with varying configurations aimed at concurrently challenging physical and cognitive abilities. Our approach was based on preliminary findings showing that the use of momentum-based bodybuilding equipment (eg, dumbbells and barbells) was safe and feasible, and improved mobility, balance, strength, posture stability, and quality of life.Citation19,Citation20 Building on this preliminary work,Citation20 the main purpose of our study was to explore the effects of momentum-based dumbbell training on cognitive function in older adults with MCI. A secondary purpose was to examine its effects on physical performance. It was hypothesized that spinning dumbbell training would lead to improvement in cognitive function and physical performance among older adults with MCI.
Subjects and methods
Study design
We conducted a pilot randomized controlled trial with two experimental groups: a dumbbell-training group (DTG) and a control group (CG), with participants in the DTG taking part in an exercise session three times per week for 12 weeks. The study protocol was approved by the ethics committee of the Shanghai University of Sport, and written informed consent was obtained from all study participants.
Participants
Participants were recruited from three communities in Shanghai, PRC. Study eligibility criteria were: 1) ≥65 years of age; 2) memory complaint with typical general cognitive function (Mini-Mental Status Evaluation [MMSE]Citation21 ≥24,Citation22 Montreal Cognitive Assessment [MoCA]Citation23 <26;Citation24 3) the ability to perform daily living activities (Activities of Daily Living scale <26);Citation25 and 4) not clinically demented.Citation4 Individuals were excluded if they: 1) had any musculoskeletal or joint problems, major neurological, cardiac, or cerebrovascular diseases, or other medical diseases associated with cognition and physical performance; 2) were unable to make a 12-week commitment during the study period; or 3) were participating in any regular physical activities or exercise programs.
Recruitment, randomization, masking, and baseline measurement
Participants were recruited primarily through initial contacts with community leaders and presentations at community centers, where study protocols (assessment, group assignment, and training) were described in detail. Those who qualified for study eligibility were assigned randomly to either the DTG or CG. Group-allocation sequence was generated through a computer-generated list and was delivered by a research-team staff member. Assessors who conducted outcome assessments were blind to group allocation. Baseline assessment, which included demographics, anthropometrics, cognitive function, and physical performance, was completed in a research laboratory at the Shanghai University of Sport. Intervention began within 1 week after the baseline assessment was completed.
Intervention
Intervention group
The protocol used in this study was based on a pilot study in which we showed that momentum-based dumbbell training was safe and suitable for healthy middle-aged and older adults, and improved their mobility, balance, well-being, and sleep quality.Citation20 Participants in the DTG participated three times per week over 12 weeks in a 60-minute momentum-based dumbbell-training class. All classes were conducted at local senior centers.
The momentum-based dumbbell is a handheld device with two built-in eccentric pendulums (~9 cm in length) at each end. Each dumbbell is 32 cm in length, 22 cm in diameter, and weighs 1.92 kg. Both the size and weight of the dumbbell were fixed for all participants.Citation26
The dumbbell training involved instructor-led handheld dumbbell-spinning exercises performed on the front part or lateral side of the body (). Specifically, the spinning motion was done in different directions (eg, clockwise and counterclockwise, forward and backward) and body sides (front, ; left/right, ). Each individual spinning exercise lasted 1–2, minutes with repetitions set at 4–5 minutes. The initial exercise sessions focused on acclimatizing participants to the movement forms, and followed an easy–difficult progression of short duration (1 minute) with multiple rest breaks. Exercises progressed to longer intervals (1.5–2 minutes), with a 1-minute break between each exercise set. The level of exercise difficulty was tailored to the capabilities of participants. Once most of the participants had mastered the movement, a different movement with a new position or spinning direction and longer exercise duration was adopted to increase the challenge.
Figure 1 Pictorial representation of dumbbell spinning.
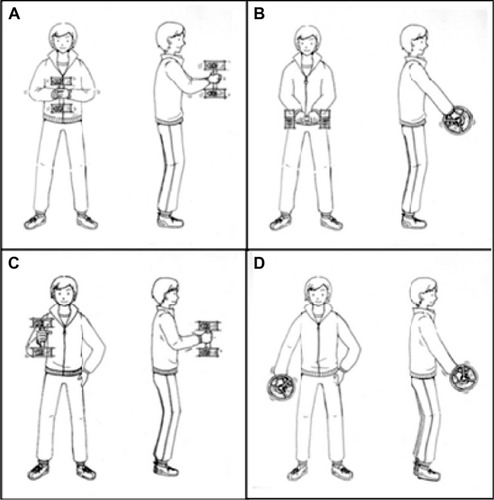
Each training session began with 5 minutes of warm-up involving light stretching of the major upper-and lower-extremity muscles, followed by 50 minutes of dumbbell-spinning exercises and a 5-minute cooldown period. Intervention sessions were delivered by two physical education students who were trained by a master instructor involved in the design and training protocol of the intervention.
Control group
The study used a passive control condition in which participants were instructed to maintain a regular lifestyle routine without starting any new exercise activities.
Measures
Primary outcomes
The study had three primary outcome measures, each of which is described in the following paragraphs.
The Chinese versionCitation27 of the Alzheimer’s Disease Assessment Scale – Cognitive subscale (ADAS-Cog)Citation28 was used to assess global cognitive function. The ADAS-Cog consists of 12 cognitive tests evaluating memory, language, praxis, and attention. ADAS-Cog scores ranged from 0 to 75, with higher scores indicating greater severity of CI. In this study, 12-week test–retest reliability was 0.60, with 91.9% sensitivity and 89.5% specificity.Citation29
The Trail Making Test part B (TMT-B; Chinese version) was used to assess executive function.Citation29,Citation30 The TMT-B is a time-based test (in seconds) that requires participants to track letters and numbers alternately (eg, 1, A, 2, B, 3, C). The 12-week test–retest reliability was 0.83, with 87% sensitivity and 90% specificity.Citation29
The Digit Span Test – forward (DST-F; Chinese version) and DST – backward (DST-B; Chinese version) were used to assess immediate memory and attention.Citation29 During each test, participants were asked to recall the numbers in forward order (DST-F) or in backward order (DST-B), which were presented at the rate of one every second. The 12-week test–retest reliability for the two tests was 0.80 and 0.73, respectively, with 46% sensitivity (77% specificity) and 77% sensitivity (78% specificity),Citation29 respectively.
Secondary outcomes
There were three secondary outcome measures used. The Timed Up and Go (TUG) test was used to assess functional mobility. Participants were asked to stand up from a chair, walk 3 m, turn around, and return to the chair.Citation31 The 12-week test–retest reliability for this test was 0.76, with 87% sensitivity and 100% specificity.Citation32
The functional reach test was used to assess forward stability. Participants were asked to reach forward as far as possible while maintaining their balance without moving their feet.Citation33 The 12-week test–retest reliability for this test was 0.72, with 62% sensitivity and 92% specificity.Citation32
The Activities-Specific Balance Confidence scale assesses participants’ perceived confidence in performing balance-related activities.Citation34 Participants were required to rate their confidence in performing each activity without falling on a 1–5 scale, with 1 indicating “not at all confident” and 5 indicating “completely confident”. The 12-week test–retest reliability for this test was 0.83, with 65% sensitivity and 77% specificity.Citation35
Statistical analysis
Data were analyzed using intent to treat. Baseline characteristics of the study participants were analyzed using analysis of variance for continuous variables and a χ2 test for categorical variables. Repeated-measure analysis of variance (group × time) was performed to assess the effects of intervention on cognitive function and physical performance. Important covariates, such as age, sex, education, and health status, were included in the initial analyses. Because results were not altered, the final results were based on unadjusted model testing. An α-level of 0.05 was considered statistically significant. Data analyses were performed using SPSS software (version 20.0; IBM Corporation, Armonk, NY, USA).
Sample size
We calculated that a sample size of 40 participants would provide 80% power (at a two-tailed α-level of 0.05) for detecting differences between groups for an effect size of 0.4 in the ADAS-Cog.Citation36 Assuming a 10% attrition rate, the study recruited a total of 44 participants (22 per group).
Results
Sample characteristics
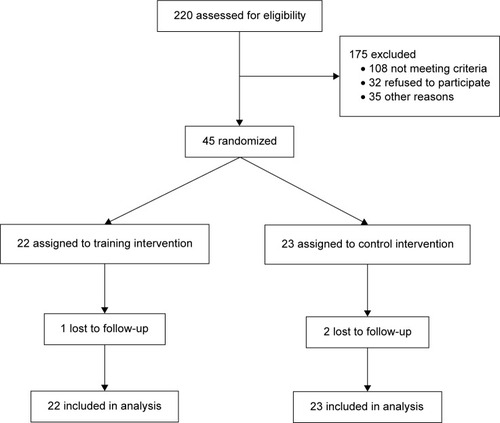
A total of 220 individuals were screened. Of these, 175 were excluded for such reasons as not meeting eligibility criteria, being unwilling to participate, or being unavailable due to time conflicts. A final pool of 45 qualified individuals were randomized, with 22 assigned to DTG and 23 assigned to CG (). Demographic, anthropometric, cognitive, medication, and comorbidity characteristics of the participants at baseline are shown in . There were no significant differences between the two groups with regard to baseline descriptors (P>0.05).
Table 1 Baseline characteristics of trial participants
Figure 2 Flowchart of participants from screening to completion of the study.
Compliance and adverse events
One participant in the DTG dropped out due to family-related issues and two dropped out in the CG for reasons related to health and traveling; 42 participants completed the 12-week intervention. The average attendance for the DTG was 31 sessions (of 36 total, range 24–36 sessions). There were no adverse events observed during the course of intervention.
Change in primary outcomes
At the end of the 12-week intervention, participants in the DTG showed significant improvement in the ADAS-Cog (F=6.95, P=0.012) compared to those in the CG (). Participants in the DTG exhibited a significant pre- to postintervention improvement in TMT-B (t=3.42, P=0.003) and DST-B (t=−2.41, P=0.025) scores. However, there was a significant within-group pretest–posttest change in TMT-B scores (t=3.14, P=0.005) observed in the CG.
Table 2 Effect of intervention on cognitive function (n=45)
Change in secondary outcomes
Compared to those in the CG, participants in the DTG showed significant improvement in the TUG test (F=4.34, P=0.043). There was no between-group difference in other outcomes ().
Table 3 Effects of intervention on physical function (n=45)
Discussion
In this study, we explored the potential health benefit of a novel, momentum-based dumbbell-training intervention on cognitive function in older adults with MCI. The results indicated that compared to a control condition, a 12-week dumbbell-training intervention significantly improved cognition, as indicated by the positive change in the ADAS-Cog score. Though no between-group difference was observed, there was a significant within-group change (improvement) in TMT-B and DST-B measures, indicating a positive trend in these domain-specific cognitive measures. Compared to those in the CG, the DTG participants showed a concomitant improvement in the mobility measure of the TUG test. The intervention was shown to have satisfactory compliance, as indicated by the low attrition rate (<5%), good attendance rate (mean 31 sessions), and no adverse events. These observations collectively suggest the feasibility of implementing the novel intervention in a community setting and the safety in performing momentum-based dumbbell-spinning exercises with older adults with MCI.
Results from this pilot study support growing evidence that shows physical activity or exercise benefits cognitive function in older adults with MCI.Citation13–Citation17,Citation37 The finding on the improved ADAS-Cog scores is consistent with previous exercise-based interventions involving home-based aerobicCitation13 and multimodal exercises.Citation14 To the best of our knowledge, this is the first time that a momentum-based dumbbell-training approach has been used to target change in cognition function. Although the study was exploratory in nature, the findings suggest that dumbbell training is potentially beneficial and may be considered an exercise modality for preventing decline in cognitive function or delaying the onset of dementia in older adults with MCI.
In addition to demonstrating improvement in cognitive measures, the study also showed improved functional mobility, as measured by the TUG test. This finding may be attributed to the fact that dumbbell training is considered a strength-based exercise modality, which may have an impact on lower-limb strength, control of center of mass, and coordination. This may in turn help promote functional activities (ie, sit-to-stand, walking, turning, and stand-to-sit) that are relevant to older adults’ activities of living. To ensure the relevance of the training to promoting healthy aging, future studies should consider assessing change in cognitive function in relation to change in physical performance-based outcomes.
Although the mechanism by which the intervention resulted in the positive change in cognitive function is unclear (apart from the need to engage physically in resistance-based dumbbell-spinning exercises), the variation in position changes and movement configurations during the dumbbell-training sessions engages participants in several features pertaining to cognition, such as spatiotemporal orientation, selective attention, and executive control. Integrating motor and cognitive challenges into the multitasking exercise routine may have driven the change in cognitive function among the dumbbell-training participants. Future studies should further examine the potential value of this modality by integrating measures of cognition, sensory, and biomechanical characteristics (eg, kinematics and kinetics) to gain insight into how the momentum-based exercise is able to elicit exercise-induced change in cognitive function.
A major strength of the study is the novelty of using a dumbbell-spinning exercise intervention to evaluate change in cognitive function. However, the study has at least two notable limitations. First, the study used a passive control group. It is thus possible that the positive findings observed in the exercise group may have been due in part to extensive contact time with or attention received from the intervention staff, and/or the Hawthorne effect. Future studies should establish a better choice of a control condition to ensure comparable contact time or attention control. Second, although participants were selected based on some established cognitive measures, they were relative healthy and physically mobile, which could explain the relatively small effect observed.
In conclusion, results from this preliminary study demonstrated that a 12-week, momentum-based dumbbell-training intervention improved cognitive function, especially global cognitive function, in older adults with MCI. Given the promising results, future studies should evaluate the efficacy of this novel exercise modality in improving specific dimensions of cognitive function, and (using a longer follow-up time) examine the sustainability of its training effects.
Acknowledgments
The authors would like to express their gratitude to all the volunteers who participated in this study, and to Ms Xiaodan Li and Mr Pei Ma for teaching and instructing the intervention classes. This study was supported by the National Natural Science Foundation of China (11372194), the Science and Technology Commission of Shanghai (14DZ1103500), and the Education Commission of Shanghai (15cxy46).
Disclosure
The authors report no conflicts of interest in this work.
References
- World Health OrganizationDementia: A Public Health PriorityGenevaWHO2012
- SongYWangJOverview of Chinese research on senile dementia in mainland ChinaAgeing Res Rev20109Suppl 1S6S1220813206
- BrookmeyerRJohnsonEZiegler-GrahamKArrighiHMForecasting the global burden of Alzheimer’s diseaseAlzheimers Dement20073318619119595937
- PetersenRCSmithGEWaringSCIvnikRJTangalosEGKokmenEMild cognitive impairment: clinical characterization and outcomeArch Neurol199956330330810190820
- PetersenRCThomasRGGrundmanMVitamin E and donepezil for the treatment of mild cognitive impairmentN Engl J Med2005352232379238815829527
- FeldmanHHFerrisSWinbladBEffect of rivastigmine on delay to diagnosis of Alzheimer’s disease from mild cognitive impairment: the InDDEx studyLancet Neurol20076650151217509485
- ThalLJFerrisSHKirbyLA randomized, double-blind, study of rofecoxib in patients with mild cognitive impairmentNeuropsychopharmacology20053061204121515742005
- DoiTMakizakoHShimadaHObjectively measured physical activity, brain atrophy, and white matter lesions in older adults with mild cognitive impairmentExp Gerontol2014621625528600
- MakizakoHLiu-AmbroseTShimadaHModerate-intensity physical activity, hippocampal volume, and memory in older adults with mild cognitive impairmentJ Gerontol A Biol Sci Med Sci201470448048625147086
- TanigawaTTakechiHAraiHYamadaMNishiguchiSAoyamaTEffect of physical activity on memory function in older adults with mild Alzheimer’s disease and mild cognitive impairmentGeriatr Gerontol Int201414475876224646035
- JedrziewskiMKEwbankDCWangHTrojanowskiJQExercise and cognition: results from the National Long Term Care SurveyAlzheimers Dement20106644845521044775
- GrandeGVanacoreNMaggioreLPhysical activity reduces the risk of dementia in mild cognitive impairment subjects: a cohort studyJ Alzheimers Dis201439483383924296815
- LautenschlagerNTCoxKLFlickerLEffect of physical activity on cognitive function in older adults at risk for Alzheimer disease: a randomized trialJAMA200830091027103718768414
- SuzukiTShimadaHMakizakoHA randomized controlled trial of multicomponent exercise in older adults with mild cognitive impairmentPloS One201384e6148323585901
- SuzukiTShimadaHMakizakoHEffects of multicomponent exercise on cognitive function in older adults with amnestic mild cognitive impairment: a randomized controlled trialBMC Neurol20121212823113898
- CassilhasRCLeeKSFernandesJSpatial memory is improved by aerobic and resistance exercise through divergent molecular mechanismsNeuroscience201220230931722155655
- ten BrinkeLFBolandzadehNNagamatsuLSAerobic exercise increases hippocampal volume in older women with probable mild cognitive impairment: a 6-month randomised controlled trialBr J Sports Med201549424825424711660
- KhanKMThompsonAMBlairSNSport and exercise as contributors to the health of nationsLancet20123809836596422770457
- SunMYEffect of inertial barbell training on transversus abdominis muscle activityChina Sport Sci Technol2013491140145
- LüJLiuYEffect of momentum-based dumbbell training program on physical performance in middle-aged and elderly adults: a feasibility studyPoster presented at: 17th National Conference on Sports Biomechanics Academic ExchangeSeptember 29, 2014Dalian, People’s Republic of China
- FolsteinMFFolsteinSEMcHughPR“Mini-mental state”: a practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res19751231891981202204
- ZhangMYKatzmanRSalmonDThe prevalence of dementia and Alzheimer’s disease in Shanghai, China: impact of age, gender, and educationAnn Neurol19902744284372353798
- NasreddineZSPhillipsNABédirianVThe Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairmentJ Am Geriatr Soc200553469569915817019
- LuJLiDLiFMontreal Cognitive Assessment in detecting cognitive impairment in Chinese elderly individuals: a population-based studyJ Geriatr Psychiatry Neurol201124418419022228824
- HillLRKlauberMRSalmonDPFunctional status, education, and the diagnosis of dementia in the Shanghai surveyNeurology19934311381458423878
- LiuYLuJQinventorsShanghai University of Sport, assigneeDumbbell having adjustable inertial resistance load characteristicUnited States Patent US8251878B22012828
- WangHShuLSiTTianCHZhangHYValidity and reliability of Chinese version of Alzheimer’s Disease Assessment ScaleChin J Clin Psychol2000828992 Chinese
- RosenWGMohsRCDavisKLA new rating scale for Alzheimer’s diseaseAm J Psychiatry198414111135613646496779
- GuoQHongZNeuropsychological AssessmentShanghaiShanghai Science and Technology Press2013
- StraussEShermanEMSpreenOA Compendium of Neuropsychological Tests: Administration, Norms, and Commentary3rd edNew YorkOxford University Press2006
- MathiasSNayakUIsaacsBBalance in elderly patients: the” get-up and go” testArch Phys Med Rehabil19866763873893487300
- ThomasJILaneJVA pilot study to explore the predictive validity of 4 measures of falls risk in frail elderly patientsArch Phys Med Rehabil20058681636164016084819
- DuncanPWWeinerDKChandlerJStudenskiSFunctional reach: a new clinical measure of balanceJ Gerontol1990456M192M1972229941
- PowellLEMyersAMThe Activities-Specific Balance Confidence (ABC) scaleJ Gerontol A Biol Sci Med Sci199550A1M28M347814786
- CattaneoDRegolaAMeottiMValidity of six balance disorders scales in persons with multiple sclerosisDisabil Rehabil2006281278979516754576
- OrrellMYatesLABurnsAIndividual Cognitive Stimulation Therapy for dementia (iCST): study protocol for a randomized controlled trialTrials20121317222998983
- PortoFHCoutinhoAMPintoALEffects of aerobic training on cognition and brain glucose metabolism in subjects with mild cognitive impairmentJ Alzheimers Dis201546374776025835427