
Abstract
Background and purpose
Autonomic dysfunction is common after stroke, which is correlated with unfavorable outcome. Phase-rectified signal averaging is a newly developed technique for assessing cardiac autonomic function, by detecting sympathetic and vagal nerve activity separately through calculating acceleration capacity (AC) and deceleration capacity (DC) of heart rate. In this study, we used this technique for the first time to investigate the cardiac autonomic function of patients with acute hemispheric ischemic stroke.
Methods
A 24-hour Holter monitoring was performed in 63 patients with first-ever acute ischemic stroke in hemisphere and sinus rhythm, as well as in 50 controls with high risk of stroke. DC, AC, heart rate variability parameters, standard deviation of all normal-to-normal intervals (SDNN), and square root of the mean of the sum of the squares of differences between adjacent normal-to-normal intervals (RMSSD) were calculated. The National Institutes of Health Stroke Scale (NIHSS) was used to assess the severity of stroke. We analyzed the changes of DC, AC, SDNN, and RMSSD and also studied the correlations between these parameters and NIHSS scores.
Results
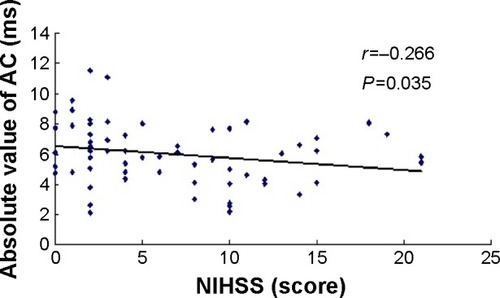
The R–R (R wave to R wave on electrocardiogram) intervals, DC, AC, and SDNN in the cerebral infarction group were lower than those in controls (P=0.003, P=0.002, P=0.006, and P=0.043), but the difference of RMSSD and the D-value and ratio between absolute value of AC (|AC|) and DC were not statistically significant compared with those in controls. The DC of the infarction group was significantly correlated with |AC|, SDNN, and RMSSD (r=0.857, r=0.619, and r=0.358; P=0.000, P=0.000, and P=0.004). Correlation analysis also showed that DC, |AC|, and SDNN were negatively correlated with NIHSS scores (r=−0.279, r=−0.266, and r=−0.319; P=0.027, P=0.035, and P=0.011).
Conclusion
Both DC and AC of heart rate decreased in patients with hemispheric infarction, reflecting a decrease in both vagal and sympathetic modulation. Both DC and AC were correlated with the severity of stroke.
Introduction
Stroke has become the leading cause of death in the People’s Republic of ChinaCitation1 and the second most common cause of death worldwide.Citation2 Cardiac autonomic dysfunction is common after stroke, which is correlated with unfavorable outcome.Citation3,Citation4 As an electrophysiological method, heart rate variability (HRV) has been used to assess the autonomic function for decades. Studies have shown that HRV is related to the severity of strokeCitation5 and has some mortality predictive values.Citation6 However, it cannot accurately distinguish the sympathetic and vagal nerve activity. Phase-rectified signal averaging (PRSA) is a newly developed technique for detecting cardiac autonomic function, which can quantitatively detect the function of vagal and sympathetic nerves by calculating the deceleration capacity (DC) and acceleration capacity (AC) of the heart, respectively. Its advantages have been shown in the field of cardiology.Citation7 However, this method has not yet been used in the study of autonomic dysfunction after stroke. In this study, the changes in DC and AC of heart rate and other related parameters were studied in patients with acute cerebral infarction for the purpose of investigating their values in assessing the autonomic function of patients with stroke.
Materials and methods
Subjects
A total of 63 patients (38 men and 25 women; mean age, 71±12 years) with first-ever acute cerebral infarction and sinus rhythm were recruited within 72 hours after stroke. A magnetic resonance imaging (MRI) or computed tomography (CT) scan confirmed the infarction located in the cerebral hemispheres, with 35 in the left hemisphere and 28 in the right. Patients with manifestations of other nervous system lesions and patients with any other diseases or medication known to affect the autonomic nervous system were excluded. Patients with tumor, infection, previous heart, or pulmonary disease were also excluded.
A total of 50 controls (24 men and 26 women; mean age, 68±11 years) were recruited from subjects with high risk of stroke but without history of stroke. Patients who had two or more of the following major risk factors, or one major risk factor, and two or more secondary risk factors were defined as patients with high risk of stroke. Major risk factors include 1) hypertension, 2) hyperlipidemia, 3) diabetes mellitus, 4) age >50 years, and 5) metabolic syndrome; secondary risk factors include 1) atrial fibrillation or heart disease, 2) smoking, 3) family history of stroke or heart attack, 4) obesity, 5) regular alcohol consumption, 6) lack of physical exercise, 7) dietary excess oil, 8) sleep apnea, 9) male, 10) often gums bleeding, teeth loose, or loss, 11) ischemic ophthalmopathy, and 12) sudden deafness. MRI was used in the control group to exclude acute infarction. The other exclusion criteria were the same as for the stroke group.
We obtained oral informed consent from both patients and controls or their clients. This study was approved by the ethics committee of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital. Sex, age, and combined basic diseases and conditions were not statistically different between the two groups ().
Table 1 Comparison between infarction patients and controls
Clinical materials
MRI was used to obtain the side and location information of the infarction. If MRI was contraindicated or unable to be obtained, repeat CT scans were used in order to identify the exact location of infarction. The National Institutes of Health Stroke Scale (NIHSS) was used to record the severity of neurologic deficit. An experienced neurologist was in charge of this work.
Detection of autonomic parameters
All patients underwent a 24-hour Holter monitoring within 1 week after admission. The recordings were analyzed by a DMS Holter system (DMS300-3; Diagnostic Monitoring Software, Stateline, NV, USA). The interferences were excluded, and the events of arrhythmia were tagged artificially when playing back the recordings. The signal processing technique of PRSA was used to process sequences of R–R intervals obtained from the Holter recordings.Citation8 This technique provides separate characterizations of deceleration- and acceleration-related modulations, quantified by DC and AC. It is believed that DC reflects vagal activity and AC reflects sympathetic activity of the heart. The computer calculated DC and AC automatically. Meantime, standard deviation of all normal-to-normal intervals (SDNN) and square root of the mean of the sum of the squares of differences between adjacent normal-to-normal intervals (RMSSD) were also calculated through the 24-hour Holter recordings, which were widely used parameters of HRV and were considered to reflect overall variability and parasympathetic modulation of the heart, respectively. As the values of AC were negative, we used the absolute value of AC (|AC|) in the analyses. We also calculated the D-value between |AC| and DC (|AC|−DC) and the ratio of |AC| and DC (|AC|/DC) to reflect the balance of sympathetic and parasympathetic modulation. The electrophysiological analysts remained blinded to the clinical data during the study period.
Statistical analysis
Mean values (± standard deviation [SD]) were calculated for continuous variables. Distributions of continuous variables were determined by the Shapiro–Wilk test. Group differences were assessed by Student’s t-test or Mann–Whitney U-test. Comparisons of categorical variables were made using chi-square test or Fisher’s exact test. Correlations between different autonomic parameters were calculated using Pearson’s correlation test, and correlations between autonomic parameters and NIHSS scores were calculated using Spearman rank correlation test. Data analysis was performed using SPSS Version 17.0 (SPSS Inc., Chicago, IL, USA). A value of P<0.05 was considered statistically significant.
Results
Comparison of autonomic parameters between infarction patients and controls
Compared with controls, the R–R intervals, DC, AC, and SDNN of the infarction group were lower. But the difference of RMSSD, the D-value between |AC| and DC (|AC|−DC), and the ratio of |AC| and DC (|AC|/DC) were not statistically significant compared with controls ().
Comparison between left and right hemispheric infarction
Some autonomic parameters of patients with the right hemispheric infarction were slightly lower than that of the left, but the differences were not statistically significant ().
Table 2 Comparison between left and right hemispheric infarction
Correlation analysis
In the infarction group, DC correlated significantly with |AC|, SDNN, and RMSSD. In 63 patients with stroke, NIHSS scores ranged from 0 to 21 (6.52±5.68). There is a negative correlation between NIHSS and DC, |AC|, and SDNN. No significant correlation was identified between NIHSS scores and RMSSD, the D-value between |AC| and DC, and the ratio of |AC| and DC (; –).
Table 3 Correlation analysis between parameters of infarction group
Figure 1 Correlation between DC and absolute value of AC.
Abbreviations: AC, acceleration capacity; DC, deceleration capacity.
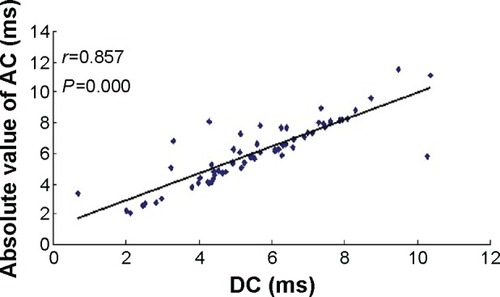
Figure 2 Correlation between NIHSS scores and DC.
Abbreviations: DC, deceleration capacity; NIHSS, National Institutes of Health Stroke Scale.
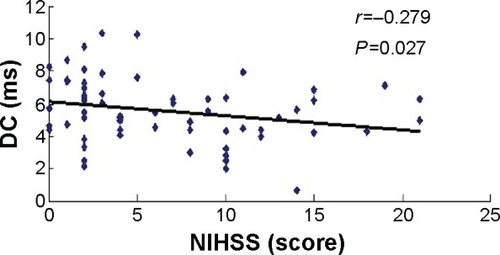
Figure 3 Correlation between NIHSS scores and absolute value of AC.
Discussion
Patients with stroke often complicate with cardiac autonomic dysfunction, which can lead to a variety of cardiac arrhythmias, T wave change, myocardial infarction, and even sudden death.Citation9 Cardiac involvement is an important cause of death after stroke.Citation10 Sympathetic hyperactivity and decrease in parasympathetic activity caused by stroke may be the reason of arrhythmia and sudden death. Studies found that cardiac autonomic dysfunction was related to the location and severity of strokeCitation4,Citation5 and may be related to the unfavorable outcome of stroke.Citation6,Citation11,Citation12
HRV has been used to detect the cardiac autonomic modulation for decades. However, it cannot distinguish the sympathetic and vagus nerve activity. In addition, there is no HRV parameter directly reflecting sympathetic modulation.Citation13 Plasma catecholamine concentrations are usually used to measure the function of sympathetic nerve. However, plasma catecholamine concentrations are affected by many factors, such as the release, distribution, metabolism, and excretion of amines,Citation14 and they are also affected by circadian rhythm.Citation15 PRSA is a new technique for detecting autonomic function. It can detect the AC and DC of the heart directly through analyzing the overall trend of 24-hour heart rate, and thus it can quantitatively detect the sympathetic activity and vagus activity, respectively, at the same time.Citation7,Citation8 This technique has been used mainly in the field of cardiovascular medicine, but not yet in the analysis of autonomic dysfunction after stroke.
In our study, we found that DC and AC as well as SDNN were all lower than controls, reflecting both sympathetic and vagal modulation loss in patients with hemispheric infarction. DC and AC were correlated with each other strongly, and the D-value and the ratio of absolute value of AC and DC had no significant difference compared with controls, reflecting that there was no major change in sympathovagal balance in patients with stroke. The loss of parasympathetic modulation is consistent with HRV studies.Citation3,Citation16 However, the decrease in AC reflects a decrease in sympathetic activity, which is inconsistent with studies concluding that the sympathetic activity of stroke increased through the detection of catecholamine concentrations.Citation16,Citation17 In the clinic, increased blood pressure, heart rate, and other characteristics of enhanced sympathetic activity are common in patients with cerebral infarction. In our study, we also found that R–R intervals of patients with infarction were shorter than those in controls, which might be a reflection of sympathetic hyperactivity. Our findings demonstrate a phenomenon that both the vagal and sympathetic modulation decrease after stroke, but the combined effects of the two result in predominant sympathetic activity. This phenomenon could be explained by the fact that the effect of heart rate increasing by decreased vagal activity was larger than the effect of heart rate decreasing by decreased sympathetic activity. The sympathetic activity is relatively predominant rather than absolutely predominant.
The study results were not conclusive of whether the lateralization and location of infarction were associated with autonomic derangement. Most studies found that if the infarctions are located in the right hemisphere especially with insula involvement, the cardiac autonomic dysfunction was more pronounced.Citation4,Citation18,Citation19 In this study, autonomic parameters of patients with left and right cerebral infarction were compared. Although the autonomic parameters of patients with right hemispheric infarction were slightly lower than those of the left hemisphere, the differences were not statistically significant. Due to limited sample size, patients with the insula involvement were not analyzed separately. A further study of a larger number of cases is needed to search for the effect of lateralization and location of infarction on the autonomic nervous system.
In this study, the NIHSS score was used to assess the severity of stroke. Correlation analysis showed that DC, absolute value of AC, and SDNN were negatively correlated with NIHSS scores, which indicates a higher risk of autonomic complications in patients with more severe stroke.Citation5 Although significant correlations between autonomic parameters and NIHSS scores were found, the r values were rather low. We assume that autonomic function is affected by many factors such as age, sex, and combined diseases, which do not influence the NIHSS scores directly. The infarction location and lateralization also have different effects on autonomic modulation and NIHSS scores.
Declining autonomic modulation predicts poor outcomes in many diseases, such as myocardial infarction,Citation20 chronic heart failure,Citation21 and ischemic stroke.Citation6 Studies also showed that vagus nerve had protective effects.Citation22,Citation23 The decline of vagal modulation may decrease this protective effect. DC, which is a direct reflection of vagal modulation, has shown its value in predicting mortality after myocardial infarction.Citation7 Our study has also shown a decline in DC in patients with hemispheric infarction. Further studies for the value of DC in prognosis prediction in patients with stroke are deserved.
Conclusion
Both DC and AC decrease in patients with acute hemispheric infarction, reflecting the loss of both parasympathetic and sympathetic modulation after stroke. The clinical manifestations of hyperactivity of sympathetic nerve after stroke are possibly a reflection of the relative increase of sympathetic activity caused by more decline of vagal activity. Both DC and AC were correlated negatively with the severity of stroke. For the protective effect of vagal nerve, a decline of vagal modulation might have some predictive values for unfavorable outcomes after stroke. Further studies for the predictive value of DC and AC for the prognosis of stroke are deserved.
Acknowledgments
The authors sincerely thank the participants of this study for their cooperation. This study was supported by grants from the Science and Technology Foundation of Shanghai (14401970303).
Disclosure
The authors report no conflicts of interest in this work.
References
- LiuLWangDWongKSWangYStroke and stroke care in China: huge burden, significant workload, and a national priorityStroke201142123651365422052510
- LozanoRNaghaviMForemanKGlobal and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010Lancet201238098592095212823245604
- KorpelainenJTSotaniemiKAHuikuriHVMyllyäVVAbnormal heart rate variability as a manifestation of autonomic dysfunction in hemispheric brain infarctionStroke19962711205920638898816
- TokgozogluSLBaturMKTop uogluMASaribasOKesSOtoAEffects of stroke localization on cardiac autonomic balance and sudden deathStroke19993071307131110390300
- HilzMJMoellerSAkhundovaAHigh NIHSS values predict impairment of cardiovascular autonomic controlStroke20114261528153321493903
- MäkikallioAMMäkikallioTHKorpelainenJTSotaniemiKAHuikuriHVMyllyäVVHeart rate dynamics predict poststroke mortalityNeurology200462101822182615159485
- BauerASchmidtGKantelhardtJWDeceleration capacity of heart rate as a predictor of mortality after myocardial infarction: cohort studyLancet200636795231674168116714188
- BauerAKantelhardtJWBundeAMalikMSchneiderRSchmidtGPhase-rectified signal averaging detects quasiperiodicities in non-stationary dataPhysica A2006364423434
- AyHKoroshetzWJBennerTNeuroanatomic correlates of stroke-related myocardial injuryNeurology20066691325132916525122
- ProsserJMacGregorLLeesKRVISTA InvestigatorsPredictors of early cardiac morbidity and mortality after ischemic strokeStroke20073882295230217569877
- ColivicchiFBassiASantiniMCaltagironeCPrognostic implications of right-sided insular damage, cardiac autonomic derangement, and arrhythmias after acute ischemic strokeStroke20053681710171516020766
- BassiAColivicchiFSantiniMCaltagironeCCardiac autonomic dysfunction and functional outcome after ischaemic strokeEur J Neurol200714891792217662015
- CygankiewiczIZarebaWHeart rate variabilityHandb Clin Neurol201311737939324095141
- EslerMJenningsGLambertGMeredithIHorneMEisenhoferGOverflow of catecholamine neurotransmitters to the circulation: source, fate, and functionsPhysiol Rev19907049639851977182
- SchöflCBeckerCPrankKvon zur MühlenABrabantGTwenty-four-hour rhythms of plasma catecholamines and their relation to cardiovascular parameters in healthy young menEur J Endocrinol199713766756839437236
- AkılETamamYAkılMAIdentifying autonomic nervous system dysfunction in acute cerebrovascular attack by assessments of heart rate variability and catecholamine levelsJ Neurosci Rural Pract20156214515025883469
- MyersMGNorrisJWHachniskiVCSoleMJPlasma norepinephrine in strokeStroke19811222002047233464
- ColivicchiFBassiASantiniMCaltagironeCCardiac autonomic derangement and arrhythmias in right-sided stroke with insular involvementStroke20043592094209815272134
- StrittmatterMMeyerSFischerCGeorgTSchmitzBLocation-dependent patterns in cardio-autonomic dysfunction in ischaemic strokeEur Neurol2003501303812824710
- La RovereMTBiggerJTJrMarcusFIMortaraASchwartzPJBaroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (autonomic tone and reflexes after myocardial infarction) investigatorsLancet199835191014784849482439
- NolanJBatinPDAndrewsRProspective study of heart rate variability and mortality in chronic heart failure: results of the United Kingdom heart failure evaluation and assessment of risk trial (UK-heart)Circulation19989815151015169769304
- AyINapadowVAyHElectrical stimulation of the vagus nerve dermatome in the external ear is protective in rat cerebral ischemiaBrain Stimul20158171225312600
- NgGAVagal modulation of cardiac ventricular arrhythmiaExp Physiol201499229529924014808