
Abstract
Background
Data from the Nordic health care registers have been of great value in perinatal epidemiological research. It has been assumed that findings from the Nordic population (Denmark, Finland, Iceland, Norway, and Sweden) are applicable to other populations as well, including the population of the US.
Objective
To describe and compare maternal and infant characteristics between the Nordic and the American populations as recorded in the official statistics.
Materials and methods
This population-based study included data on all females who gave birth and their infants in the Nordic countries and the US. The data were obtained from the US National Center for Health Statistics and the official statistics data for the Nordic countries. The data from all six countries included births from 2006 to 2010.
Results
The mean maternal age at delivery was lower in the US than in the Nordic countries (27.5 vs 30.3 years). Cesarean sections (32.2% vs 17.9%), low birth weight (8.2% vs 4.8%), and preterm birth (12.3% vs 5.9%) were more common in the US than in the Nordic countries. Smoking during early pregnancy was slightly less common in the US compared with Nordic countries (9.8% vs 11.2%). Restricting the data from the US to females with a university degree, characteristics such as age at delivery, birth weight, and preterm deliveries were more in alignment with the Nordic data.
Conclusion
There are differences in some key maternal and neonatal characteristics between the Nordic countries and the US. However, some characteristics are related to socioeconomic status, suggesting that the Nordic data seem to be applicable to the part of the population in the US with a higher socioeconomic status.
Background
The Nordic countries (Denmark, Finland, Iceland, Norway, and Sweden) have been collecting health data of high quality and complete coverage in national registers for decades.Citation1–Citation7 All the Nordic countries have public health care systems and it is mandatory for the health care professionals to report to the national registers, including data on births, cancer, in- and outpatient care visits, causes of death, and prescribed drugs.Citation6,Citation7
All residents of the Nordic countries are assigned a unique personal identification number at birth or immigration.Citation6–Citation9 The personal identification number allows for accurate linkage of information from the different registers. The possibility of linking data has made the Nordic health care registers valuable in epidemiological research.Citation6,Citation7
It has been assumed that findings in the Nordic population are applicable to other populations as well.Citation10,Citation11 However, due to genetic and socioeconomic differences between the Nordic and other populations, such as the population of the US, the generalizability of the data may be questioned. The aim of this population-based study was to describe and compare the characteristics of females and their infants in the Nordic countries and the US.
To the best of our knowledge, this is the first study that compares both similarities and differences in characteristics between the Nordic countries and the US among pregnant females and infants.
Materials and methods
Data source and study population
The study included data on all females who gave birth, and their infants, between 2006 and 2010 in the Nordic countries and the US. The American data were obtained from the official statistics held at the National Center for Health Statistics at the Centers for Diseases Control and Prevention.Citation12 The Centers for Diseases Control and Prevention data files included data from the birth data files, the birth cohort – infant death data files, and the fetal death data files. The US data files are considered to have a high degree of completeness and 99% of all births are recorded in the birth data files. The Nordic data were obtained from the official statistics in each countryCitation13–Citation22 and from a previous Nordic collaborative study based on information in the national health care registers.Citation11 Some data from Finland were provided directly by the National Institute for Health and Welfare in Finland.Citation23
Each Nordic country has a medical birth register that records detailed information on all females, deliveries, and their infants. The American data were based on birth certificates and included data on infants born after gestational week 17. In this study, a lower limit of 22 weeks gestational age was used for inclusion. The study was mainly based on official statistics from the Nordic countries and the US and included data at an aggregated level, which is publicly available on the Internet. For research containing no personal data there is, according to Swedish law, no requirement for ethics review. Data was also obtained from the previous Nordic collaborative study,Citation11 and that study was approved by the Regional Ethical Review Board at Karolinska Institutet in Stockholm, Sweden; the National Board of Health, Denmark; the Danish Data Protection Agency; the National Institute for Health and Welfare of Finland; Statistics Finland; the Data Protection Authority and the National Bioethics Committee in Iceland; and the Norwegian Data Inspectorate.
Maternal and infant characteristics
Characteristics related to the pregnancy (maternal age, parity, maternal marital status, maternal country of birth, race, and smoking in early pregnancy), the delivery (cesarean section, number of infants, and gestational length), and the infants (birth weight, sex, congenital anomalies, stillbirth, and neonatal death) were compared between the Nordic countries and the US. Cesarean section was defined as a delivery performed by cesarean section independent of whether it was a planned or an emergency section. Parity was given based on the number of previous pregnancies leading to a delivery independent of whether the newborn was dead or alive at the time of birth. For the first pregnancy, the parity was zero. Number of infants were the number of infants born at a delivery and were grouped as single (one infant) or multiple (two or more infants). Maternal country of birth was only reported for the Nordic countries and the mothers were categorized as born in a Nordic country or not. Information on race was not available in the Nordic countries and was therefore only reported for the US as Whites, Blacks, American Indian/American native, or Asian/Pacific Islander. Low birth weight was defined as weight <2,500 g and high birth weight as >4,500 g. The sex of the infant was the sex reported on the birth certificate and was grouped as female or male. Preterm birth was defined as birth <37 gestational weeks and very preterm delivery as birth <32 gestational weeks. Post-term birth was defined as birth after ≥42 weeks of gestation. The congenital anomalies reported in the study were anencephaly, meningomyelocele/spina bifida, omphalocele/gastroschisis, and Down syndrome. Stillbirth was defined as the birth of an infant who showed no evidence of life after 22 weeks of gestation. Neonatal death was defined as the death of a live-born infant within the first 27 days after birth and was grouped as early neonatal death (0–6 days) and late neonatal death (7–27 days). Smoking in early pregnancy was defined as those who reported smoking during the first trimester. The marital status of the mother grouped as “married” included both legally married and cohabiting in Sweden, while in the US it only included the parents who were legally married. For Finland, Iceland, and Norway, information on legally married, cohabiting, and unmarried mothers was available in separate categories. No information on marital status was available from Denmark. The marital status was compared in two ways. First, “married” was compared, excluding Sweden, since Sweden did not have separate categories for married and cohabiting. Second, married and cohabiting as a combined variable in the Nordic countries was compared with married in the US. All data management and analysis were carried out using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Statistical analysis
Descriptive estimates were calculated in the form of central tendency (mean values) and distributions. Estimates were presented together with 95% confidence intervals. For the Nordic data, the mean age for the aggregated years 2006–2010 was obtained by calculating the weighted mean age, using the number of deliveries per year to create the weight.
In additional analyses, characteristics related to the pregnancy, delivery, and infants were also estimated, restricting the data from the US to females who had graduated from university as a proxy for higher socioeconomic status (SES).
Results
In total, 22,593,635 births were included in the study, 21,099,903 from the US and 1,493,732 from the Nordic countries ().
Table 1 Point estimates and 95% CIs of maternal and infant characteristics for births between 2006 and 2010 in the US and the Nordic countries (Denmark, Finland, Iceland, Norway, and Sweden)
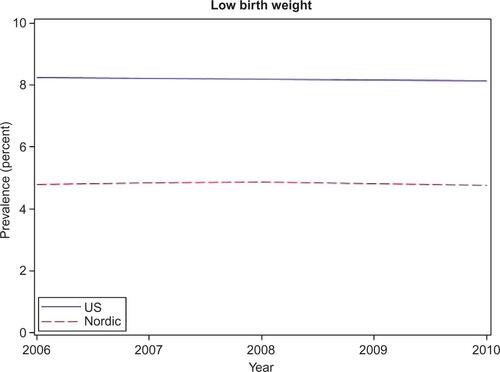
The mean maternal age at delivery was lower in the US compared to the Nordic countries, both for all deliveries (27.5 vs 30.3 years) and the first delivery (24.8 vs 28.3 years). The mean age for both the first delivery and all deliveries was stable in both the regions during the study period ( and ). Cesarean sections were almost twice as common in the US as in the Nordic countries (32.2% vs 17.9%), and the occurrence did not change during the study period (). In the US, 19.5% of mothers had a parity ≥3. In the Nordic countries, the corresponding proportion was 6.5%. A higher proportion of females were married in the US compared to the Nordic countries (59.9% vs 51.8%). When comparing the Nordic combined variable of married and cohabiting to married in the USA, the proportion in the US was lower than in Nordic countries (59.9% vs 90.2%). Low birth weight (8.2% vs 4.8%) and preterm delivery (12.3% vs. 5.9%) were more frequent in the US, while high birth weight (1.0% vs 3.3%) and post-term delivery (5.6% vs 7.4%) were less common in the US. The proportion of infants with low birth weight did not change over time in any of the compared populations ().
The prevalence of congenital anomalies differed between the populations. For anencephaly, the prevalence was higher in the US (12 vs 1 per 1,00,000 live-birth singletons), and for Down syndrome the prevalence was lower in the US compared to the Nordic countries (49 vs 103 per 1,00,000 live-birth singletons). Smoking in early pregnancy was less common in the US than in the Nordic countries (9.8% vs. 11.2%). Smoking varied widely among the Nordic countries: from 6.9% in Sweden to 18.0% in Norway (). The prevalence of smoking in early pregnancy decreased in both the Nordic countries and the US during the study period ().
Figure 1 Prevalence of females who gave birth and reported smoking during early pregnancy in the US and the Nordic countries between 2006 and 2010.
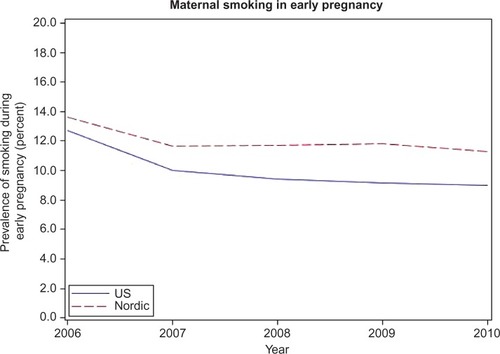
Table 2 Point estimates and 95% CIs of maternal and infant characteristics for births between 2006 and 2010 by Nordic countries (Denmark, Finland, Iceland, Norway, and Sweden)
Restricting the data from the US to only include females with a university degree revealed that their characteristics were more similar to those of females in the Nordic countries, eg, maternal age at all deliveries (31.2 years), maternal age at the time of the first delivery (29.5 years), parity ≥3 (14.3%), birth weight <2,500 g (7.0%), and preterm delivery <37 weeks of gestation (10.6%). The proportion of married pregnant females with a university degree in the US was similar to that of Nordic females who were married or cohabiting (88.5% vs 90.2%).
Discussion
In this comparison between the Nordic countries and the US, which included over 20 million pregnancies, we found that the mean maternal age was higher in the Nordic countries both for the first delivery and for all deliveries. The prevalence of cesarean section was almost twice as high in the US. Having at least three children, being married, low birth weight, preterm delivery, and anencephaly were more common in the US, whereas in the Nordic countries, it was more common that infants had a high birth weight, were born post-term, or had Down’s syndrome. Smoking in early pregnancy was more common in the Nordic countries.
The observed differences in the characteristics of pregnant populations of the US and the Nordic countries likely contribute to differences seen in pregnancy outcomes. In the US, ~40% of the deliveries in 2003 were covered by Medicaid, a social health care program for families and individuals with low income and resources.Citation24 This indicates that a high proportion of the mothers in the US had a low SES, which likely affected many of the variables assessed in this study. When restricting the US data to females with a university degree, as a proxy for higher SES, the characteristics were more similar to those of Nordic females. However, there were still differences between the groups, which are likely due to factors other than SES, such as genetic differences, or differences on a structural level in the society affecting all citizens independent of SES (eg, treatment recommendations, procedures, or organizations of the health care systems). Nevertheless, this indicates that the Nordic population mirrors those in the US with a higher SES better than the overall US population. It is also worth mentioning that, in Sweden, in 2010, ~42% of all females in the age 25–64 years had a university degree.Citation25
The prevalence of cesarean section increases with age.Citation26 However, the results in this study found that cesarean section was less common in the Nordic countries compared to the US, despite a higher mean age at delivery. This contradiction may reflect different obstetric practices and health care system organizations. Cesarean section may affect morbidity and mortality later on in life for infants as well as mothers. For example, infants delivered by cesarean section have both short- and long-term increased risk of developing type 1 diabetes, asthma, and allergies.Citation27,Citation28 Cesarean sections have been associated with different complications for the mother, eg, an increased risk of preeclampsia in subsequent pregnancies,Citation29 but may also have beneficial effects, such as lower risk of adverse birth outcomes in breech presentations and decreased risk of pelvic organ prolapse symptoms.Citation30,Citation31 Though the World Health Organization in 1985 set the optimal rates for cesarean section to be 10%–15%, the rates have continued to increase globally, including in the Nordic countries.Citation32,Citation33
Low maternal SES has been associated with an increased risk of both giving birth to infants with low birth weight (<2,500 g) and preterm deliveries (<37 weeks).Citation34 A higher proportion of females with low SES in the US may explain the higher proportion of low birth weight and preterm deliveries in the US. As for cesarean delivery, both low and high birth weight may explain a higher occurrence of conditions seen later on in life. Low birth weight has been associated with systolic hypertension, asthma, and type 2 diabetes.Citation35–Citation37 High birth weight, which was more frequent in the Nordic countries, has also been associated with an increased risk of poor health such as type 1 and 2 diabetes, and obesity.Citation35,Citation38,Citation39
The higher proportion of mothers with a parity ≥3 in the US may be a result of younger age at first delivery, allowing time for more pregnancies to occur during a female’s reproductive lifetime. It is also possible that the higher parity reflects religious and cultural differences between the compared regions.
There was a small difference in the prevalence of congenital anomalies between the compared regions. However, due to the rarity of congenital anomalies, the small number of observed cases limit the possibility to determine any real difference between the Nordic countries and the US. For example, during the 5 years studied, there were only nine cases of anencephaly in the Nordic countries. The observed differences could be due to differences in clinical practice such as routine ultrasounds during pregnancy and attitudes toward termination. The higher maternal age at delivery in the Nordic countries may contribute to the higher prevalence of Down syndrome seen in the Nordic countries.
It should be noted that, for the US, previous studies found the prevalence data concerning the anomalies that were assessed in this comparison to be underestimated.Citation40,Citation41 Data from SwedenCitation42–Citation46 and FinlandCitation47,Citation48 also indicate that anomalies could be underreported in the medical birth registers, as some anomalies may be diagnosed after discharge from the postnatal care units and for that reason may not get included in the birth registers.
According to previous studies, smoking during pregnancy is more common among mothers with a low SES and younger mothers.Citation49,Citation50 With this in mind, and the assumed higher proportion of mothers with low SES in the US, it would be expected that smoking is more common in the US than in the Nordic countries. The higher prevalence in the Nordic countries was mainly due to the high prevalence in Finland (14.9%) and Norway (18.0%) (). In Norway, smoking was only recorded for females who gave their consent to register this information.Citation13–Citation17 Accordingly, the actual proportion of smokers during early pregnancy may be even higher in Norway.
Strengths
This study has covered all births in the Nordic countries and the US that occurred between 2006 and 2010, and the completeness of data in all countries is high.Citation12,Citation51 The large number of pregnancies obtained from using the registers facilitated comparison of the groups with a good degree of accuracy. The use of register data reduces the level of recall bias and sampling uncertainty. The study also included information concerning several covariates, which are important when considering differences in pregnancy outcomes.
Limitations
Some of the assessed variables were not available in all the Nordic countries. For example, maternal marital status was missing for Denmark; maternal country of birth was missing for Finland and Norway. Smoking during pregnancy was not captured in Iceland and in Norway only the mothers who gave their consent were registered as smokers. However, as the missing data were for a whole population, this cannot cause bias. Discrepancies between the different countries regarding the exact time period during pregnancy for which the characteristics were recorded may be a limitation to the comparisons.
Conclusion
There are some differences in maternal and neonatal characteristics between the Nordic countries and the US and it is important to be aware of these differences when generalizing findings based on data from the Nordic countries to the general US population. It is notable that the Nordic maternal and neonatal characteristics were more similar to those of the females in the US with a university degree, indicating that SES should be taken into consideration when generalizing findings from the Nordic countries.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
We would like to thank Sarah Burkill for her help with the language copyediting.
Supplementary materials
Figure S1 Mean age at delivery for females who gave birth in the US and in the Nordic countries between 2006 and 2010.
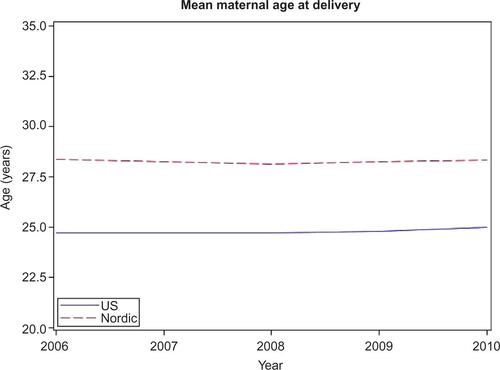
Figure S2 Mean age at first delivery for females who gave birth in the US and the Nordic countries between 2006 and 2010.
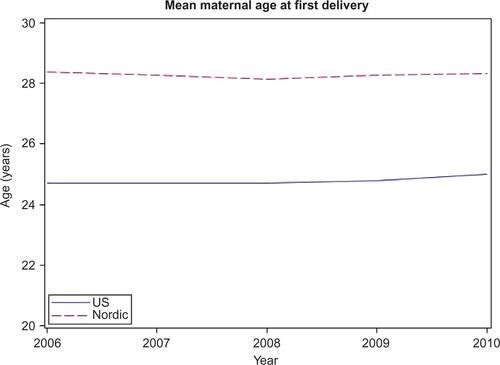
Figure S3 Prevalence of cesarean section of females who gave birth in the US and the Nordic countries between 2006 and 2010.
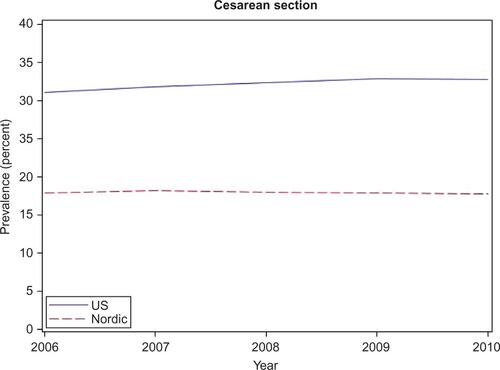
Figure S4 Prevalence of low birth weight among infants born in the US and the Nordic countries between 2006 and 2010.
Disclosure
The authors report no conflicts of interest in this work.
References
- GisslerMTeperiJHemminkiEMerilainenJData quality after restructuring a national medical registryScand J Soc Med199523175807784857
- TeperiJMulti method approach to the assessment of data quality in the Finnish Medical Birth RegistryJ Epidemiol Community Health19934732422478350040
- KnudsenLBOlsenJThe Danish Medical Birth RegistryDan Med Bull19984533203239675544
- MelveKKLieRTSkjaervenRRegistration of Down syndrome in the Medical Birth Registry of Norway: validity and time trendsActa Obstet Gynecol Scand200887882483018607831
- CnattingiusSEricsonAGunnarskogJKallenBA quality study of a medical birth registryScand J Soc Med19901821431482367825
- KielerHNordic databases to evaluate medications in pregnancyTherapie2014691656924698190
- RosenMNational Health Data Registers: a Nordic heritage to public healthScand J Public Health2002302818512028856
- FuruKWettermarkBAndersenMMartikainenJEAlmarsdottirABSorensenHTThe Nordic countries as a cohort for pharmacoepidemiological researchBasic Clin Pharmacol Toxicol20101062869419961477
- Langhoff-RoosJKrebsLKlungsoyrKThe Nordic medical birth registers – a potential goldmine for clinical researchActa Obstet Gynecol Scand201493213213724237585
- LudvigssonJFStromPLundholmCMaternal vaccination against H1N1 influenza and offspring mortality: population based cohort study and sibling designBMJ2015351h558526572546
- KielerHArtamaMEngelandASelective serotonin reuptake inhibitors during pregnancy and risk of persistent pulmonary hypertension in the newborn: population based cohort study from the five Nordic countriesBMJ2012344d801222240235
- Center for diseases prevention (CDC)Vital statistics2015 Available from: http://www.cdc.gov/nchs/data_access/VitalStatsOnline.htmAccessed September 29, 2015
- Norwegian Institute of Public HealthÅrstabeller for Medisinsk Fødselsregister 2005–20062008 Available from: http://www.fhi.no/dokumenter/b268921580.pdfAccessed October 12, 2015
- Norwegian Institute of Public HealthÅrstabeller for Medisinsk Fødselsregister 20072009 Available from: http://www.fhi.no/dokumenter/676bc56530.pdfAccessed October 12, 2015
- Norwegian Institute of Public HealthÅrstabeller for Medisinsk Fødselsregister 20082010 Available from: http://www.fhi.no/dokumenter/b05ede8c59.pdfAccessed October 12, 2015
- Norwegian Institute of Public HealthÅrstabeller for Medisinsk Fødselsregister 20092011 Available from: http://www.fhi.no/dokumenter/9a55cc5467.pdfAccessed October 12, 2015
- Norwegian Institute of Public HealthÅrstabeller for Medisinsk Fødselsregister 20102012 Available from: http://www.fhi.no/dokumenter/d3421cc3c3.pdfAccessed October 12, 2015
- THLPerinatal Statistics in the Nordic countries 2012National Institute for Health and Welfare - Finland2014 Available from: https://www.julkari.fi/bitstream/handle/10024/125322/Tr31_14.pdf?sequence=3Accessed October 14, 2015
- THLPerinatal Statistics: Parturients, Deliveries and Newborns 20132014 Available from: https://www.julkari.fi/bitstream/handle/10024/116818/Tr23_14.pdf?sequence=3Accessed October 14, 2015
- Hagstofa Islands. Births and Deaths Available from: http://www.statice.is/Statistics/Population/Births-and-deathsAccessed October 16, 2015
- Statistics Denmark (DST)Population and elections – births2015 Available from: http://www.statbank.dk/statbank5a/default.asp?w=2560Accessed October 19, 2015
- SocialstyrelsenPregnancies, Deliveries and Newborn Infants – The Swedish Medical Birth Register 1973–20132014 Available from: https://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/19627/2014-12-19.pdfAccessed October 29, 2015
- THLNational Institute for Health and Welfare2015 Available from: https://www.thl.fi/sv/web/thlfi-enAccessed October 27, 2015
- GarciaGMaternal and Child Health (MCH) Update: States Increase Eligibility for Childrens’s Health in 20072008 Available from: http://www.nga.org/files/live/sites/NGA/files/pdf/0811MCHUPDATE.PDFAccessed October 20, 2015
- Statistics Sweden, SCBUtbildningsnivå 1990–2014 efter kön, 25–64 år; 2014 Available from: http://www.scb.se/sv_/Hitta-statistik/Statistikefter-amne/Utbildning-och-forskning/Befolkningens-utbildning/Befolkningens-utbildning/#c_undefinedAccessed January 25, 2016
- LukeBBrownMBElevated risks of pregnancy complications and adverse outcomes with increasing maternal ageHum Reprod20072251264127217289684
- ThavagnanamSFlemingJBromleyAShieldsMDCardwellCRA meta-analysis of the association between caesarean section and child-hood asthmaClin Exp Allergy200838462963318352976
- BagerPWohlfahrtJWestergaardTCaesarean delivery and risk of atopy and allergic disease: meta-analysesClin Exp Allergy200838463464218266879
- ChoGJKimLYMinKJPrior cesarean section is associated with increased preeclampsia risk in a subsequent pregnancyBMC Pregnancy Childbirth2015152425879208
- TrutnovskyGKamisan AtanIMartinADietzHPDelivery mode and pelvic organ prolapse: a retrospective observational studyBJOG Epub2015105
- VillarJCarroliGZavaletaNMaternal and neonatal individual risks and benefits associated with caesarean delivery: multicentre prospective studyBMJ20073357628102517977819
- BetranAPTorloniMRZhangJWhat is the optimal rate of caesarean section at population level? A systematic review of ecologic studiesReprod Health2015125726093498
- WHOAppropriate technology for birthLancet1985284524364372863457
- BlumenshinePEgerterSBarclayCJCubbinCBravemanPASocioeconomic disparities in adverse birth outcomes: a systematic reviewAm J Prev Med201039326327220709259
- HarderTRodekampESchellongKDudenhausenJWPlagemannABirth weight and subsequent risk of type 2 diabetes: a meta-analysisAm J Epidemiol2007165884985717215379
- MuMWangSFShengJBirth weight and subsequent blood pressure: a meta-analysisArch Cardiovasc Dis201210529911322424328
- MuMYeSBaiMJBirth weight and subsequent risk of asthma: a systematic review and meta-analysisHeart Lung Circ201423651151924582482
- HarderTRoepkeKDillerNStechlingYDudenhausenJWPlagemannABirth weight, early weight gain, and subsequent risk of type 1 diabetes: systematic review and meta-analysisAm J Epidemiol2009169121428143619363100
- JohnssonIWHaglundBAhlssonFGustafssonJA high birth weight is associated with increased risk of type 2 diabetes and obesityPediatr Obes2015102778324916852
- ParkerSEMaiCTCanfieldMAUpdated National Birth Prevalence estimates for selected birth defects in the United States, 2004–2006Birth Defects Res A Clin Mol Teratol201088121008101620878909
- WatkinsMLEdmondsLMcClearnAMullinsLMulinareJKhouryMThe surveillance of birth defects: the usefulness of the revised US standard birth certificateAm J Public Health19968657317348629729
- SocialstyrelsenBirth Defects 20062007 Available from: http://www.socialstyrelsen.se/lists/artikelkatalog/attachments/9323/2007-42-14_20074214.pdfAccessed October 14, 2015
- SocialstyrelsenBirth Defects 20072008 Available from: http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/8722/2008-125-22_200812522_rev.pdfAccessed October 14, 2015
- SocialstyrelsenBirth Defects 20082009 Available from: https://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/17807/2009-11-6.pdfAccessed October 14, 2015
- SocialstyrelsenBirth Defects 20092010 Available from: https://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/18175/2010-11-16.pdfAccessed October 14, 2015
- SocialstyrelsenBirth Defects 20102011 Available from: https://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/18481/2011-11-10.pdfAccessed October 14, 2015
- THLCongenital Anomalies 1993–20082011 Available from: http://www.stakes.fi/tilastot/tilastotiedotteet/2011/Tr07_11.pdfAccessed November 16, 2015
- THLCongenital Anomalies 1993–20112014 Available from: http://www.julkari.fi/bitstream/handle/10024/114911/Tr06_14.pdf?sequence=4Accessed October 14, 2015
- EkbladMGisslerMKorkeilaJLehtonenLTrends and risk groups for smoking during pregnancy in Finland and other Nordic countriesEur J Public Health201424454455124025664
- RaisanenSKramerMRGisslerMSaariJHakulinen-ViitanenTHeinonenSSmoking during pregnancy was up to 70% more common in the most deprived municipalities – a multilevel analysis of all singleton births during 2005–2010 in FinlandPrev Med20146761124983887
- GisslerMRegistration of births and induced abortions in the Nordic countries – Finnish yearbook of population researchXLV2010171178 Available from: http://ojs.tsv.fi/index.php/fyp/article/viewFile/45059/11337Accessed March 24, 2016