
Abstract
Purpose
Individuals with cerebral palsy (CP) are at increased risk for frailty and chronic disease due to factors experienced throughout the lifespan, such as excessive sedentary behaviors and malnutrition. However, little is known about noncommunicable diseases (NCDs) and multimorbidity profiles in young adults with CP. The study objective was to compare NCD and multimorbidity profiles between young adults with and without CP.
Methods
A clinic-based sample of adults (18–30 years) with (n=452) and without (n=448) CP was examined at the University of Michigan Medical Center. The prevalence and predictors of 13 NCDs were evaluated, including existing diagnoses or historical record of musculoskeletal, cardiometabolic, and pulmonary morbidities. The level of motor impairment was determined by the Gross Motor Function Classification System (GMFCS) and stratified by less vs more severe motor impairment (GMFCS I–III vs IV–V). Logistic regression was used to determine the odds of NCD morbidity and multimorbidity in adults with CP compared to adults without CP, and for GMFCS IV–V compared to GMFCS I–III in those with CP, after adjusting for age, sex, body mass index, and smoking.
Results
Adults with CP had a higher prevalence of osteopenia, osteoporosis, hypertension, myocardial infarction, hyperlipidemia, asthma, and multimorbidity compared to adults without CP, and higher odds of musculoskeletal (odds ratio [OR]: 6.97) and cardiometabolic morbidity (OR: 1.98), and multimorbidity (OR: 2.67). Adults with CP with GMFCS levels IV–V had a higher prevalence of osteopenia/osteoporosis, osteoarthritis, hypertension, other cardiovascular conditions, pulmonary embolism, and multimorbidity, and higher odds of musculoskeletal (OR: 3.41), cardiometabolic (OR: 2.05), pulmonary morbidity (OR: 1.42), and multimorbidity (OR: 3.45) compared to GMFCS I–III.
Conclusion
Young adults with CP have a higher prevalence of chronic NCDs and multimorbidity compared to young adults without CP, which is pronounced in those with more severe motor impairment. These findings reiterate the importance of early screening for prevention of NCDs in CP.
Introduction
Cerebral palsy (CP) results from damage to or malformation of the infant brain and is the most common physical disability in childhood.Citation1 Children with CP present with impaired neuromuscular function,Citation2–Citation4 low levels of physical activity,Citation5–Citation7 poor cardiorespiratory fitness,Citation8 underdeveloped musculoskeletal tissue,Citation5,Citation6 and a high degree of fat of total bodyCitation9 and musculoskeletalCitation5,Citation6 depots, which are largely governed by the extent of motor impairment.Citation5,Citation6 Mobility decrements are common in children with CP as they transition into and throughout adulthood.Citation10–Citation12 Consequently, individuals with CP may be at a heightened risk for developing chronic, noncommunicable diseases (NCDs) at younger ages compared to the general population.
There has been a considerable shift in the global burden of disease, with the prevalence of NCDs now outranking injuries and communicable, maternal, neonatal, and nutritional disorders combined.Citation13 The burden of NCDs has been climbing with estimated costs of $7 trillion US dollars by 2030.Citation14 The adult CP population is steadily growing due to increases in survival rateCitation15 and prevalenceCitation16 of CP in recent decades. Indeed, CP represents a significant lifetime disability for individuals, their families, and caregivers. CP is associated with increased prevalence of cardiometabolic mortalityCitation17 and morbidity,Citation18,Citation19 greatly reducing life expectancy,Citation20 all of which may develop or be accelerated by the presence of impairments and/or the aging process.Citation18,Citation19 There is, thus, strong rationale for approaching health care delivery for persons with CP within the context of a life course health development model.Citation21 However, the framework that encompasses clinical care for patients with CP has been largely confined to issues that arise during childhood and adolescence, with little to no focus on understanding life course health development.
A comprehensive understanding of the primary and resulting sequela associated with aging in those with CP is lacking, especially in the early adult years. Better understanding these changes in health through the lifespan will help to guide future, target-specific preventive efforts in rehabilitation research and clinical practice to mitigate the exaggerated chronic conditions observed in patients with CP.Citation19 The primary objective of this study was to examine the NCD profiles and risk factors in young adults with CP compared to young adults without CP. We hypothesized that young adults with CP would have a higher prevalence of NCDs compared to those without CP, and that risk factors would include obesity and greater motor impairments.
Patients and methods
Patient identification
A cohort query tool (Data Direct: https://datadirect.med.umich.edu) was used to identify patients who had clinical appointments at the University of Michigan Medical Center, as previously described.Citation19 Briefly, we annotated the dataset using the Electronic Medical Records Search Engine (EMERSE) software. The EMERSE software is hosted behind the University of Michigan Medical Center firewall in a computing environment certified for storing protected health information. Access to EMERSE is limited to authorized personnel who have patient data access privileges or, among those using it for research, have provided evidence of training in responsible research practices and proof of valid institutional review board (IRB) approvals, including demonstration of a need to review identifiable patient information.Citation22 At each login, users must complete a brief attestation form to document their intent of use. Audit trail logs are kept for each use session. The principal investigators (Peterson and Hurvitz) take full responsibility for de-identifying patient records and maintaining patient data confidentiality. The University of Michigan IRB approved this retrospective study, and patient consent to review their medical record was waived by the IRB because the nature of this study involved no more than minimal risk to the subjects; the waiver did not adversely affect the rights and welfare of the subjects; the research could not practicably (ie, feasibly) be carried out without the waiver.
This internally developed web application provides an interface for searching electronic medical records with a bundle of word iterations and phrases for variables of interest.Citation22 Adults between 18 and 30 years of age, with a confirmed diagnosis of CP or no known neurological disorders (controls), who had an encounter with University of Michigan Medicine between 01/01/2011 and 07/31/2017 (6.5-year period), were considered for this study. Among individuals with CP, the distribution of affected limbs (ie, quadriplegic, hemiplegic, diplegic) was obtained from medical records. The level of motor impairment was classified according to the Gross Motor Function Classification System (GMFCS). GMFCS ranks motor impairment with GMFCS I/II reflecting gross motor independence, GMFCS III reflecting the use of assistive walking devices, and GMFCS IV–V reflecting wheelchair use for most to all mobility. We stratified GMFCS into two categories, GMFCS I–III and GMFCS IV–V, to reflect lesser and greater motor impairment, respectively.
Noncommunicable diseases
Clinical data were included for existing diagnosis or historical record of various NCDs and were grouped into three categories, including 1) musculoskeletal morbidity: osteopenia and osteoporosis, osteoarthritis, and rheumatoid arthritis; 2) cardiometabolic morbidity: stroke, hypertension, other cardiovascular problems (eg, heart valve disorders, peripheral artery disease, aortic aneurysm, heart failure), coronary artery disease, impaired glucose tolerance or type 2 diabetes, myocardial infarction, and hyperlipidemia (total cholesterol >240 mg/dL and/or triglyceride >200 mg/dL); and 3) pulmonary morbidity: asthma, pulmonary embolism, and emphysema. These conditions were chosen because of their potential impact on physical function and in accordance with the guidance from the literature relating to older adults and adults with disabilities.Citation23,Citation24
In addition to using the EMERSE, certain variables required additional data collection. For blood pressure, the most recent measurement was used to determine hypertension status (present vs absent) based on the Eighth Joint National Committee:Citation25 systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg. A clinical history of stroke and/or other cardiovascular problems (eg, heart valve disorders, peripheral artery disease, aortic aneurysm, heart failure) was included if it occurred at 18 years or older. Musculoskeletal, cardiometabolic, and pulmonary morbidities were defined on the basis of presence of at least one of the aforementioned chronic NCDs within each respective category. A morbidity score was created by summing the number of individual NCDs. Multimorbidity was defined as the presence of having at least two of the aforementioned NCDs.
Covariates
Demographic data, including race, age, and sex, were collected using the EMERSE software. Body mass index (BMI) was calculated by dividing body mass by height squared (kg/m2). BMI was separated into underweight (<18.5), normal weight (18.5–24.9), overweight (25.0–29.9), and obese (≥30.0) categories. Smoking status was categorized as never vs current, occasional, or previous smoker.
Statistical analyses
Descriptive characteristics are provided as mean, standard deviation, and percentages. Participant demographics and NCD prevalence were compared between groups (young adults with vs without CP) and between the level of motor impairment for those with CP (GMFCS I–III vs IV–V) using two-sample t-tests and chi-square (χ2) tests for continuous and categorical measures, respectively. Multiple logistic regression was used to determine the odds of NCD morbidity categories (musculoskeletal, cardiometabolic, and pulmonary) and multimorbidity, after adjusting for age, sex, race, BMI, and smoking status. The primary exposure of CP was included as a dichotomous indicator variable in all models. Data were analyzed using SAS software version 9.3 (SAS institute, Cary, NC, USA) with 2-sided 95% confidence intervals to determine significance.
Results
Descriptive characteristics
Descriptive characteristics of the study participants with (n=452) and without (n=448) CP are presented in . There were no group differences in age, sex, or obesity prevalence. However, there were group differences in race, underweight, normal weight, and overweight measures, and adults with CP had a lower prevalence of smoking status compared to adults without CP.
Table 1 Descriptive characteristics and NCD prevalence of young adults with and without CP
Of the young adults with CP, 231 (51%) were classified as GMFCS I–III and 221 (49%) as GMFCS IV–V (). There were no group differences in sex or race distribution. However, there were group differences in age, underweight, overweight, smoking status (GMFCS IV–V lower prevalence), and distribution of affected limbs in young adults with CP. A summary of morbidity score prevalence by CP status and GMFCS categories is depicted in .
Figure 1 Prevalence of morbidity score for adults with CP vs without CP, as well as for adults with CP with GMFCS levels I–III vs IV–V.
Abbreviations: CP, cerebral palsy; GMFCS, Gross Motor Function Classification System.
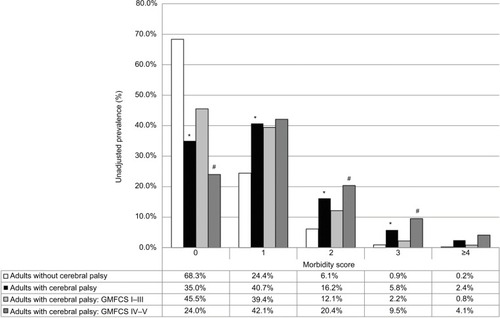
Table 2 Descriptive characteristics of young adults with cerebral palsy based on motor impairment assessed using the GMFCS
Musculoskeletal morbidity
Adults with CP had a higher prevalence of osteopenia/osteoporosis compared to those without CP (). Adults with CP had a higher odds of musculoskeletal morbidity compared to those without CP (). Greater age, being underweight, and smoking status were all significantly associated with musculoskeletal morbidity.
Table 3 Multiple logistic regression models for predictors of musculoskeletal, cardiometabolic, and pulmonary morbidities
Of the adults with CP, those with GMFCS IV–V had a higher prevalence of osteopenia/osteoporosis and osteoarthritis compared to those with GMFCS I–III (). Moreover, a higher prevalence of musculoskeletal morbidity was found for individuals with GMFCS levels IV–V (59.3%) as compared to those with GMFCS levels I–III (31.2%), as well as higher odds of musculoskeletal morbidity (odds ratio [OR]: 3.41; 95% CI: 2.18–5.35). Greater age (OR: 1.10; 95% CI: 1.04–1.16) and underweight status (OR: 1.52; 95% CI: 1.02–1.27) were both associated with musculoskeletal morbidity in individuals with CP.
Cardiometabolic morbidity
Adults with CP had a higher prevalence of hypertension, myocardial infarction, and hyperlipidemia compared to those without CP (). Adults with CP had a higher odds of cardiometabolic morbidity compared to those without CP (), and only obesity was significantly associated with cardiometabolic morbidity.
Of the adults with CP, those with GMFCS IV–V had a higher prevalence of hypertension and other cardiovascular problems compared to those with GMFCS I–III (). Moreover, a higher prevalence of cardiometabolic morbidity was found for individuals with GMFCS levels IV–V (26.2%) compared to GMFCS levels I–III (15.2%), as well as higher odds of cardiometabolic morbidity (OR: 2.05; 95% CI: 1.20–3.50). Only obesity (OR: 1.85; 95% CI: 1.01–3.41) was significantly associated with cardiometabolic morbidity in individuals with CP.
Pulmonary morbidity
Adults with CP had a higher prevalence of asthma compared to those without CP (). There were no group differences in the odds of pulmonary morbidity (), and only smoking status was significantly associated with pulmonary morbidity.
Of the adults with CP, those with GMFCS IV–V had a higher prevalence of pulmonary embolism compared to those with GMFCS I–III (). No difference in prevalence of pulmonary morbidity was found for individuals with GMFCS levels IV–V compared to GMFCS levels I–III; however, individuals with GMFCS levels IV–V had higher odds of pulmonary morbidity (OR: 1.42; 95% CI: 1.02–1.80).
Multimorbidity
Adults with CP had a higher prevalence of multimorbidity compared to those without CP (), as well as a higher odds of multimorbidity compared to those without CP (). Underweight, obesity, and smoking status were all significantly associated with multimorbidity.
Table 4 Multiple logistic regression models for independent predictors of multimorbidity
Of the adults with CP, adults with GMFCS IV–V had a higher prevalence of multimorbidity compared to those with GMFCS I–III (). There was also a higher odds of multimorbidity among those with GMFCS levels IV–V compared to GMFCS levels I–III (OR: 3.45; 95% CI: 2.04–5.83). Only obesity (OR: 1.83; 95% CI: 1.01–1.20) was significantly associated with multimorbidity in individuals with CP.
Discussion
The principal findings of this study are that young adults with CP have a higher prevalence of NCDs relating to musculoskeletal, cardiometabolic, and pulmonary systems compared to the general population of young adults without CP. Age, being underweight or obese, smoking, and the level of motor impairment were each independently associated with higher odds of many NCDs and multimorbidity in young adults with CP.
Over the past few decades, global disease burden has shifted from premature death to years lived with disabilities, and from communicable diseases to NCDs.Citation13 Nearly 40% of global NCD-related deaths occur before the age of 70 years.Citation26 Given the increased survival rateCitation15 and a marginally increasing prevalence of CPCitation16 throughout the past several decades, there is an expanding adult CP population that is at risk for premature NCD-related deaths. In the current study, young adults with CP had a higher prevalence of multiple NCDs and a multimorbidity prevalence of nearly 25%. By middle age (40–60 years), adults with CP have a multimorbidity prevalence of nearly 60%,Citation19 which is 1.5–2.9 times higher than the general population of middle-age adults.Citation27 Collectively, these data highlight a CP-specific NCD burden that is unique from the general population.
Musculoskeletal morbidity
The finding that young adults with CP have a high prevalence of musculoskeletal morbidities is clinically important, but not surprising. Children with CP have an underdeveloped musculoskeletal system,Citation5,Citation6 with deficits presenting as early as 2 years old.Citation28 Mobility deficits are observed as children with CP age into and throughout their adult yearsCitation10–Citation12 leading to a progressive loss of mechanical loading, which is an essential stimulus for musculoskeletal growth and maintenance. Mobility deficits are also associated with musculoskeletal pain,Citation10,Citation12 which is inversely related to physical activity levels in those with CP.Citation29 We found age to be a significant risk factor for musculoskeletal morbidity in the current study, suggesting a worsening of musculoskeletal morbidity prevalence in those with CP even within a young and narrow age range.
Cardiometabolic morbidity
The progressive loss of function in persons with CP may help to explain why the risk for cardiometabolic morbidities is higher in young adults with CP.Citation30,Citation31 The prevalence of hypertension and hyperlipidemia in young adults with CP in the current study was 11.8% and 3%, respectively. Ryan et alCitation32 showed that children and adolescents with CP, aged 6–17 years, had a 10.5% prevalence of hypertension, with age being significantly and positively associated with blood pressure. Moreover, van der Slot et alCitation33 reported a higher prevalence of hypertension of 25.6% in those with CP between the ages of 25 and 45 years, while we have previously reported prevalences up to 50% in 40–60-year-olds for prehypertension and hypertension.Citation19 Ryan et alCitation34 found a prevalence of hyperlipidemia of 27.3% in adults with CP aged 18–65 years, while 9% were taking medication for dyslipidemia and another 9% for hypertension. Although the frequency reporting myocardial infarction was low in the CP cohort (2%) and absent in the adults without CP in the current study, the difference is still clinically meaningful given the young age of study participants. These findings suggest an early cardiovascular risk phenotype among individuals with CP, which provides insight as to why adults with CP have a substantially higher cardiovascular mortality rates compared to the general population.Citation17 Taken together, the window to prevent cardiovascular complications in those with CP occurs prior to reaching adulthood.
Somewhat surprisingly, we did not see a difference in the prevalence of impaired glucose tolerance or type 2 diabetes, which is consistent with another study in adults with CP that found normal fasting glucose levels.Citation34 However, a glucose challenge, such as a glucose tolerance test, may be more indicative of glucose handling, and has not been exclusively studied in those with CP. Elder et alCitation35 reported that adults with spinal cord injury, a comparative reference population often used to better understand pathologies observed in CP,Citation36,Citation37 saw no differences in fasting glucose or insulin levels compared to individuals without CP. However, after administering a glucose load, both glucose and insulin levels were significantly elevated compared to individuals without CP, suggesting impaired glucose handling. Given the hallmark altered musculoskeletalCitation5,Citation6,Citation38 and functional profilesCitation5–Citation7 in CP, both of which are associated with insulin resistance,Citation30,Citation31,Citation35 it is curious as to why glucose dysregulation is not a prevalent complication in those with CP. This phenomenon requires further investigation; and yet, it may be a direct result of poor clinical screening for metabolic diseases in this population.
Pulmonary morbidity
Children with CP have poor cardiorespiratory fitness, which is associated with an increased cardiometabolic disease risk.Citation8 In addition, the low cardiorespiratory capacity in children with CPCitation39 is linked to lower chest mobility during respiration.Citation40 It is of interest whether functional limitations in CP lead to pulmonary dysfunction and morbidity, or if pulmonary dysfunction and morbidity are drivers of the functional loss with age and subsequent increased risk for developing NCDs. Future research is needed to better understand the causal pathways leading to pulmonary dysfunction and morbidity in the context of disability severity.
The finding that modifiable risk factors, such as weight status and smoking status, are associated with NCDs and multimorbidity prevalence is consistent with our previous study in middle-age adults with CP.Citation19 While there are known associations between NCDs and being underweight,Citation41 being obese,Citation42 and using tobacco,Citation14 there are weight management and smoking cessation programs that may help to mitigate the high prevalence of NCDs observed in the adult CP population. Not surprisingly, motor impairment was also significantly associated with NCDs and multimorbidity in the current study. In general, adults with CP have lower levels of physical activity. However, the degree of physical activity restriction is inversely related to increasing levels of motor impairment.Citation43 Poor diet or malnutrition, tobacco use, and physical inactivity are the three most common modifiable risk factors associated with NCD-related premature death.Citation14 These three modifiable risk factors are associated with NCDs and multimorbidity in the entire cohort of young adults with and without CP. Interestingly, young adults with CP had a fewer number of risk factors associated with musculoskeletal morbidity, pulmonary morbidity, and multimorbidity, but similar strength of associations, compared with the combined sample of young adults with and without CP. This may suggest that those with CP have a unique set of risk factors for developing or accelerating NCDs compared with the general population. Future initiatives are needed to develop programs with goals specific to assist persons with CP and caregivers for maintaining a healthy body composition, abstinence from tobacco use, and improving sleep, nutrition, and physical activity levels.Citation44
Strength and limitations
The study has several strengths. To date, this is the largest study in young adults with CP, which also includes a control group within the same age range. The recent initiatives in CP-specific surveillance programs have helped to identify a disease burden that is accelerated in the CP population by middle age.Citation19 This has prompted the investigation of evaluating the NCD profiles in a younger cohort of adults with CP to help identify the window of disease clustering. Another strength of the current study is that all data were pulled from the same site (hospital system at the University of Michigan) and within a relatively narrow time period. This is important to consider because different global regions and time periods are associated with heterogeneous development of communicable diseases and NCDs.Citation13
Several limitations must also be discussed. First, due to the design, we were unable to determine a cause and effect among exposures and outcomes. Second, we were limited to identifying NCDs using medical records that yielded a dichotomous coding for NCDs rather than a graded scale. Therefore, the severity of conditions was not accessible, which could have provided further insight into the NCD profiles of young adults with CP (eg, bone mineral density or T-scores for osteopenia and osteoporosis). Another limitation is the accuracy of the medical charts. If the NCD was not diagnosed on their medical chart, the participant was considered to not have that NCD. However, screening for NCDs in young adults with CP is not a common clinical practice in the United States. Therefore, our estimates may actually be underrepresenting the true extent of the NCD risk in young adults with CP.
Conclusion
Young adults with CP have a high prevalence of NCDs and multimorbidity, particularly for the musculoskeletal and cardiometabolic systems. Modifiable risk factors, such as underweight, obesity, and smoking status, were associated with NCDs and multimorbidity. This is an important finding because adults with CP are not expected to have such a disease burden at a young age, and clinical screening has been inadequate. Our findings highlight the importance of clinical screening for NCD clustering in persons with CP as early as adolescence or young adulthood, and may prompt early behavioral interventions for NCD prevention in this population.
Author contributions
EA Hurvitz and MD Peterson had full access to all of the data in the study and take full responsibility for the integrity of the data and the accuracy of the data analyses. DG Whitney, EA Hurvitz, JM Ryan, and MD Peterson contributed to the concept and design. EA Hurvitz, ZP French, EC Ellenberg, and MD Peterson contributed to acquisition of data. All authors contributed to drafting of the manuscript. MD Peterson contributed to statistical analysis, and study supervision. All authors contributed to the interpretation of data. EA Hurvitz, MJ Devlin, MS Caird, ZP French, EC Ellenberg, and MD Peterson contributed to administrative, technical, or material support. All authors contributed to critical revision of the manuscript for important intellectual content. All authors provided final approval of the manuscript version to be published, and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
We thank Rachael V Torres, University of Delaware, for critically reviewing the later versions of this manuscript. Mark D Peterson is funded by the National Institutes of Health (NIH) (1KO1 HD074706) and the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) (90IF0102-01).
Disclosure
The authors report no conflicts of interest in this work.
References
- ChristensenDVan Naarden BraunKDoernbergNSPrevalence of cerebral palsy, co-occurring autism spectrum disorders, and motor functioning - Autism and Developmental Disabilities Monitoring Network, USA, 2008Dev Med Child Neurol2014561596524117446
- StackhouseSKBinder-MacleodSALeeSCVoluntary muscle activation, contractile properties, and fatigability in children with and without cerebral palsyMuscle Nerve200531559460115779003
- MoreauNGFalvoMJDamianoDLRapid force generation is impaired in cerebral palsy and is related to decreased muscle size and functional mobilityGait Posture201235115415821930383
- RoseJMcGillKCNeuromuscular activation and motor-unit firing characteristics in cerebral palsyDev Med Child Neurol200547532933615892375
- WhitneyDGSinghHMillerFCortical bone deficit and fat infiltration of bone marrow and skeletal muscle in ambulatory children with mild spastic cerebral palsyBone201794909727732905
- JohnsonDLMillerFSubramanianPModleskyCMAdipose tissue infiltration of skeletal muscle in children with cerebral palsyJ Pediatr2009154571572019111321
- RyanJMFordeCHusseyJMGormleyJComparison of patterns of physical activity and sedentary behavior between children with cerebral palsy and children with typical developmentPhys Ther201595121609161626023216
- RyanJMHenseyOMcLoughlinBLyonsAGormleyJAssociations of sedentary behaviour, physical activity, blood pressure and anthropometric measures with cardiorespiratory fitness in children with cerebral palsyPLoS One2015104e012326725835955
- OftedalSDaviesPSBoydRNBody composition, diet, and physical activity: a longitudinal cohort study in preschoolers with cerebral palsyAm J Clin Nutr2017105236937828077375
- MorganPMcGinleyJGait function and decline in adults with cerebral palsy: a systematic reviewDisabil Rehabil20143611923594053
- DaySMWuYWStraussDJShavelleRMReynoldsRJChange in ambulatory ability of adolescents and young adults with cerebral palsyDev Med Child Neurol200749964765317718819
- BottosMFeliciangeliASciutoLGerickeCVianelloAFunctional status of adults with cerebral palsy and implications for treatment of childrenDev Med Child Neurol200143851652811508917
- MurrayCJVosTLozanoRDisability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010Lancet201238098592197222323245608
- WHOGlobal Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020Geneva, SwitzerlandWorld Health Organization2013
- BrooksJCStraussDJShavelleRMTranLMRosenbloomLWuYWRecent trends in cerebral palsy survival. Part I: period and cohort effectsDev Med Child Neurol201456111059106424966011
- PanethNHongTKorzeniewskiSThe descriptive epidemiology of cerebral palsyClin Perinatol200633225126716765723
- StraussDCableWShavelleRCauses of excess mortality in cerebral palsyDev Med Child Neurol199941958058510503915
- PetersonMDRyanJMHurvitzEAMahmoudiEChronic conditions in adults with cerebral palsyJAMA2015314212303230526624831
- CremerNHurvitzEAPetersonMDMultimorbidity in middle-aged adults with cerebral palsyAm J Med20171306e9744.e1527542609
- KruseMMichelsenSIFlachsEMBronnum-HansenHMadsenMUldallPLifetime costs of cerebral palsyDev Med Child Neurol200951862262819416329
- PalisanoRJDi RezzeBStewartDLife course health development of individuals with neurodevelopmental conditionsDev Med Child Neurol201759547047628229458
- HanauerDAMeiQLawJKhannaRZhengKSupporting information retrieval from electronic health records: a report of University of Michigan’s nine-year experience in developing and using the Electronic Medical Record Search Engine (EMERSE)J Biomed Inform20155529030025979153
- QuinonesARMarkwardtSBotoseneanuAMultimorbidity combinations and disability in older adultsJ Gerontol A Biol Sci Med Sci201671682383026968451
- SaliveMEMultimorbidity in older adultsEpidemiol Rev201335758323372025
- JamesPAOparilSCarterBL2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8)JAMA2014311550752024352797
- WHOGlobal Status Report on Noncommunicable Diseases 2014Geneva, SwitzerlandWorld Health Organization2014
- RoccaWABoydCMGrossardtBRPrevalence of multimorbidity in a geographically defined American population: patterns by age, sex, and race/ethnicityMayo Clin Proc201489101336134925220409
- HerskindARitterband-RosenbaumAWillerslev-OlsenMMuscle growth is reduced in 15-month-old children with cerebral palsyDev Med Child Neurol201658548549126510820
- VogtleLKMaloneLAAzueroAOutcomes of an exercise program for pain and fatigue management in adults with cerebral palsyDisabil Rehabil2014361081882523924251
- LukeADugasLRDurazo-ArvizuRACaoGCooperRSAssessing physical activity and its relationship to cardiovascular risk factors: NHANES 2003–2006BMC Public Health20111138721612597
- CamhiSMSissonSBJohnsonWDKatzmarzykPTTudor-LockeCAccelerometer-determined moderate intensity lifestyle activity and cardiometabolic healthPrev Med201152535836021300082
- RyanJMHenseyOMcLoughlinBLyonsAGormleyJReduced moderate-to-vigorous physical activity and increased sedentary behavior are associated with elevated blood pressure values in children with cerebral palsyPhys Ther20149481144115324700137
- van der SlotWMRoebroeckMENieuwenhuijsenCMoveFit and Lifespan Research GroupCardiovascular disease risk in adults with spastic bilateral cerebral palsyJ Rehabil Med201345986687223828200
- RyanJMCrowleyVEHenseyOMcGaheyAGormleyJWaist circumference provides an indication of numerous cardiometabolic risk factors in adults with cerebral palsyArch Phys Med Rehabil20149581540154624742941
- ElderCPAppleDFBickelCSMeyerRADudleyGAIntramuscular fat and glucose tolerance after spinal cord injury--a cross-sectional studySpinal Cord2004421271171615303112
- BaumanWAThe potential metabolic consequences of cerebral palsy: inferences from the general population and persons with spinal cord injuryDev Med Child Neurol200951Suppl 4647819740212
- PetersonMDGordonPMHurvitzEABurantCFSecondary muscle pathology and metabolic dysregulation in adults with cerebral palsyAm J Physiol Endocrinol Metab20123039E1085E109322912367
- PetersonMDGordonPMHurvitzEAChronic disease risk among adults with cerebral palsy: the role of premature sarcopoenia, obesity and sedentary behaviourObes Rev201314217118223094988
- GorterHHoltyLRameckersEEElversHJOostendorpRAChanges in endurance and walking ability through functional physical training in children with cerebral palsy. Pediatr Phys TherSpring20092113137
- ErsozMSelcukBGunduzRKurtaranAAkyuzMDecreased chest mobility in children with spastic cerebral palsyTurk J Pediatr200648434435017290570
- WangZJZhouYJGalperBZGaoFYehRWMauriLAssociation of body mass index with mortality and cardiovascular events for patients with coronary artery disease: a systematic review and meta-analysisHeart2015101201631163826025084
- KearnsKDeeAFitzgeraldAPDohertyEPerryIJChronic disease burden associated with overweight and obesity in Ireland: the effects of a small BMI reduction at population levelBMC Public Health20141414324512151
- RyanJMCrowleyVEHenseyOBroderickJMMcGaheyAGormleyJHabitual physical activity and cardiometabolic risk factors in adults with cerebral palsyRes Dev Disabil20143591995200224864052
- VerschurenOMcPheePRosenbaumPGorterJWThe formula for health and well-being in individuals with cerebral palsy: physical activity, sleep, and nutritionDev Med Child Neurol201658998999027518536