
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background and aims
Esophageal squamous cell carcinoma (ESCC) is the dominant histological type of esophageal cancer worldwide (90%). We aimed to provide an update of the global temporal trends in the incidence of ESCC.
Methods
Incidence data for ESCC were collected from 30 well-established cancer registries from 20 countries in Europe, Northern America, Australia, or Asia for 1970–2015. Time trends in annual age-standardized incidence rates of ESCC were assessed using joinpoint analysis and log-linear regression. Age–period–cohort analysis was used to estimate the influence of age, calendar-period, and birth-cohort on the observed time trends in incidence.
Results
The age-standardized incidence rates of ESCC varied more than eightfold in men and sevenfold in women across populations. In 2012, the highest rate of ESCC in men was observed in Nagasaki, Japan (9.7/100,000 person-years) and in women in Scotland (2.7/100,000 person-years). In men, the incidence decreased globally during the study period, as well as during the last few years. In women, the incidence increased in Japan (three regions), the Netherlands, New Zealand, Norway, and Switzerland, whereas it stabilized or decreased in other populations. Among ethnic groups in the United States, black men and women had more pronounced decreases in incidence than other groups. Generally, birth-cohort effects were stronger determinants of incidence trends than calendar-period effects.
Conclusion
In men, the global ESCC incidence has decreased over time. In women, the incidence trends vary across populations, and the rates have increased in some countries. Changes in the prevalence of tobacco smoking and alcohol consumption may have contributed to these time trends.
Introduction
Esophageal cancer is the sixth leading cause of cancer-related death globally, accounting for 440,000 deaths in 2013.Citation1 Esophageal squamous cell carcinoma (ESCC) represents 90% of all cases of esophageal cancer worldwide.Citation2,Citation3 The main risk factors for ESCC are tobacco smoking and overconsumption of alcohol, particularly in combination.Citation3 In 2012, the estimated age-standardized incidence rate was <5/100,000 person-years in both sexes in most Western countries, whereas it was >13/100,000 person-years in men and >4/100,000 person-years in women in Eastern and Southeast Asian countries.Citation2 In an analysis of a few Asian countries up to the year 2007, the ESCC incidence was decreasing in Hong Kong, Israel, and Singapore, and stable in Japan.Citation4 Studies of Western populations have found linear declines in the incidence of ESCC in Australia, Sweden, and the United States in 1984–2008,Citation5 and decreasing or stable incidence trends in European men, but increasing trends in women from Austria, Denmark, Estonia, Slovakia, and Switzerland, in 1980–2002.Citation6 However, recent global time trends have not been assessed. With the collection of the most updated incidence data from well-established cancer registries across the world, this study aimed to assess the recent global time trends in the incidence of ESCC.
Methods
Design
Data were retrieved from 30 population-based cancer registries in 20 countries during January 1, 1970 to December 31, 2015 (varying across registries). All included registries have been evaluated for high completeness and quality of the data recorded.Citation7 Cancer registries with incomplete histological information for esophageal cancer were excluded. The requested variables were the number of newly diagnosed ESCCs, calendar year of diagnosis, age at diagnosis (in 5-year groups), sex, and size of the background population at risk. The registries represented the following populations (in alphabetical order): Australia (Australian Capital Territory, New South Wales, South Australia, Tasmania, and Western Australia), China (Hong Kong), Croatia (nationwide), Finland (nationwide), France (Calvados), Iceland (nationwide), Ireland (nationwide), Italy (Veneto), Japan (Hiroshima, Miyagi, and Nagasaki), Kuwait (nationwide), Netherlands (nationwide), New Zealand (nationwide), Norway (nationwide), Slovenia (nationwide), Spain (Asturias, Granada, and Tarragona), Sweden (nationwide), Switzerland (almost nationwide), Thailand (Chiang Mai), United Kingdom (England, Scotland, and Wales), and United States (the Surveillance, Epidemiology and End Results [SEER] program). To assess the incidence time trends in the United States, including ethnicity-specific data, two combinations of the SEER registries were used: the SEER 9 registries (including the states Atlanta, Connecticut, Detroit, Hawaii, Iowa, New Mexico, San Francisco-Oakland, Seattle-Puget Sound, and Utah), with the longest registration period, and the SEER 18 registries (including all states in the SEER 9 registries plus the Alaska Native Tumor Registry, Greater California, Greater Georgia, Kentucky, Los Angeles, Louisiana, New Jersey, Rural Georgia, and San Jose-Monterey), with the widest geographic coverage.Citation8,Citation9 Data from the SEER registries were extracted from the SEER*Stat software version 8.3.3. Data from all other registries were collected by directly contacting the specific registries (contact persons are listed in Acknowledgments). Cancer registries that did not reply despite several attempts were mostly from developing countries. Data collected before 1970 were excluded to minimize differences in diagnosis coding practices between registries and, thus, make the results comparable across registries. In most registries, the diagnosis code C15 in the International Classification of Diseases, version 10 (ICD-10) defined the esophageal tumor site, and the histology codes 8050-8078 and 8083-8084 in the International Classification of Disease for Oncology, version 3 (ICD-O-3) represented squamous cell carcinoma. Detailed information about the registries included as well as coding of ESCC is presented in Table S1. Ethical approval and informed consent from participants were exempted because no personal records were accessed, and the study was based only on publicly available data of population sizes and aggregated data of cancer cases.
Statistical analysis
All analyses were stratified for sex. Data from regional registries within a country were merged to provide a wider geographic coverage and better statistical precision. Cross-sectional analysis comparing several registries was conducted for 2012, which was the most recent year of data availability in the majority of registries. The country-specific age-standardized annual incidence rates were calculated using the direct method, based on the World Standard Population 2000 as the reference, and the corresponding 95% CIs were estimated using the gamma distribution. Joinpoint analysis was conducted to identify change points in incidence trends, and to estimate the annual percentage change in each time segment before and after joinpoints. The annual percentage change was estimated on a log-linear scale under the assumption that the rate changed by a constant percentage every year on a log-scale within a specific time-period. The average annual percentage change – a weighted average of annual percentage changes from joinpoint models with weights equal to the length of each segment – was computed as a summary measure of the trend over the study period. A maximum of three predefined change points were allowed. Subgroup analyses by ethnicity (white, black, Asian/Pacific Islander, and American Indian/Alaska Native) were conducted on the basis of the SEER registries in the United States.
Age–period–cohort regression was used to evaluate the effects of age, calendar-period, and birth-cohort on the incidence rates of ESCC, using a web-tool developed by the National Cancer Institute in the United States.Citation10 Period effects result from factors that affect all age groups equally at a particular calendar time (eg, introduction of new diagnostic methods in a certain calendar period), whereas cohort effects occur when the effect of an exposure is different across age groups (birth cohorts) in a certain period and are more likely to be associated with risk factors (eg, increased smoking prevalence in younger generations).The age–period–cohort modeling was applied with 5-year age groups (varying across registries), 5-year calendar-periods (varying across countries), and consequently spanned into partially overlapping 9-year birth-cohorts. The age–period–cohort regression was based on a log-linear model for the incidence rates with additive effects from age, calendar-period, and birth-cohort as shown in the formula:
where ρpa defines the expected incidence rate, and αa, βp, and γc represent the effects of age, calendar-period, and birth-cohort, respectively. The generic effects can be separated into linear and nonlinear components. The web tool used fits the age–period–cohort model, and estimates the sum of linear components of birth-cohort and calendar-period effects (net drift), which is equivalent to the overall annual percentage change in age-standardized rates. The age-group–specific annual percentage change (local drift) was generated from the log-linear regression analysis. The relative rate in any given calendar-period (or birth-cohort) versus a reference calendar-period (or birth-cohort) was estimated with adjustment for age and nonlinear birth-cohort effects (or calendar-period effects).
The statistical software used was mainly SAS version 9.4 (SAS Institute, Cary, NC, USA), together with the Joinpoint Program (version 4.4.0.0, National Cancer Institute, United States) and the age–period–cohort web tool. All statistical tests were two-sided.
Results
Participants
The study included 180,395 patients diagnosed with ESCC from 30 registries in 20 countries in 1970–2015. Of these, 109,630 (60.8%) were men and 70,765 (39.2%) were women. The median age at diagnosis was 67.5 years (interquartile range 62.5–77.5 years).
Incidence in 2012
In men, the highest incidence rates in the year 2012 were observed in Nagasaki, Japan (9.7/100,000 person-years), Calvados, France (8.2/100,000 person-years), and Hong Kong, China (4.9/100,000 person-years), whereas the lowest rates were found in Finland and South Australia in Australia (both 1.2/100,000 person-years).
In women, the incidence rates in 2012 were generally lower than in men, with the highest rates in Scotland (2.7/100,000 person-years), Ireland (2.6/100,000 person-years), and Tasmania, Australia (2.0/100,000 person-years), and the lowest rates in Croatia, Spain (three regions) and Thailand (Chiang Mai; all 0.4/100,000 person-years).
The male-to-female ratio in 2012 was highest in Nagasaki, Japan (8.9:1) and Calvados, France (8.1:1), and lowest in Ireland (1.0:1) and South Australia, Australia (1.1:1).
Incidence trends in 1970–2015
In men, the incidence of ESCC decreased from 2000 onwards in most countries, except in Japan (three regions); however, the year when the decrease began varied across countries (). In 1990–2014, the incidence rate was gradually decreasing and relatively low (<4.0/100,000 person-years) in North-Western European countries (Finland, Ireland, Norway, the Netherlands, Sweden, Switzerland, and the United Kingdom [three regions]), Oceanian countries (Australia [five regions] and New Zealand), and the United States (SEER 9; ). A sharp decrease was observed in Calvados, France (from 28.6/100,000 person-years in 1979 to 6.4/100,000 person-years in 2013) and Hong Kong, China (from 10.1/100,000 person-years in 1994 to 5.0/100,000 person-years in 2013; ). In contrast, the incidence increased by 1.0% (95% CI 0.5%–1.6%) annually in Japan (three regions) in 1986–2005, followed by a slight decrease in 2006–2010 ( and , and ).
Figure 1 Global annual age-standardized incidence rates of esophageal squamous cell carcinoma in men (A) and women (B).
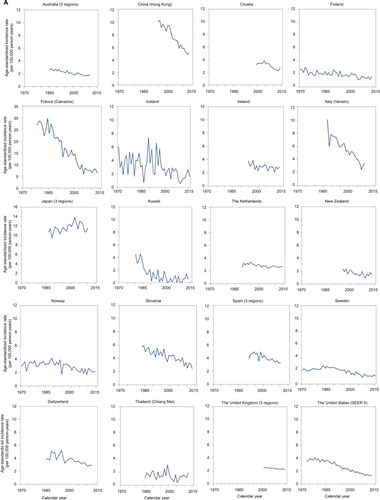
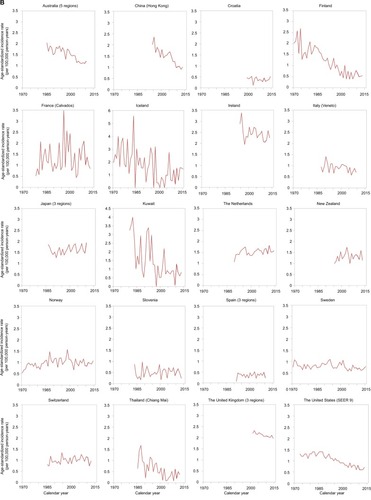
Figure 2 Average annual percentage change and 95% CI in the incidence of esophageal squamous cell carcinoma in men (A) and women (B).
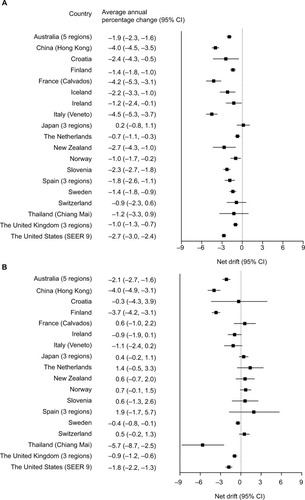
Table 1 Results from joinpoint analyses for selected registers
In women, the incidence trends increased, stabilized, or decreased, based on the country (). Increasing incidence trends were observed in Japan (three regions), the Netherlands, New Zealand, Norway, and Switzerland throughout the study period ( and ). In the Netherlands and Spain (three regions), an annual increase of >1.0% was identified during the study period. Joinpoints were found in the incidence trends both in the Netherlands and Norway in the 1990s; after the joinpoint, the incidence slightly increased in the Netherlands (annual percentage change 0.2%, 95% CI −0.3% to 0.8%), and was stable in Norway (annual percentage change −0.6%, 95% CI −1.4% to 0.3%; ). In contrast to most other countries, Hong Kong, China, and Finland showed strongly decreasing incidence rates (average annual percentage change −4.0%, 95% CI −4.9% to −3.1% and −3.7%, 95% CI −4.2% to −3.1%, respectively; ). The incidence rates were low (<1.5/100,000 person-years) in South European countries (Croatia, France [Calvados], Italy [Veneto], Slovenia, and Spain [three regions]) and were stable or slightly increasing over time, whereas the relatively high-incidence countries Ireland and the United Kingdom (three regions; >2.0/100,000 person-years) had slightly decreasing incidence rates over time ().
The male-to-female ratio ranged from 1.0:1 to 4.0:1 by country, and was stable over time in North-Western European countries, Oceanian countries, and the United States (Figure S1). In Asian (China [Hong Kong], Japan [three regions], and Thailand [Chiang Mai]) and South European countries (Croatia, France [three regions], Italy [Veneto], Slovenia, and Spain [three regions]), the male-to-female ratio ranged from 5.0:1 to 30.0:1, but decreased over time (Figure S1).
Age–period–cohort analysis
In men, interactions between calendar-period and birth-cohort effects seem to have contributed to the decrease in incidence of ESCC (Table S2). The increase in incidence trends in Japanese men showed a calendar-period effect (P=0.021), but no birth-cohort effect (P=0.059; Table S2). The analysis of age-specific percentage change indicated calendar-period effects in French men older than 50 years and Chinese men older than 40 years (). Substantial birth-cohort effects were found in New Zealand (P=0.045) and Spain (three regions; P=0.004; Table S2).
Figure 3 Age-specific annual percentage change (local drifts) in the incidence of esophageal squamous cell carcinoma stratified by sex.
Abbreviation: SEER, The Surveillance, Epidemiology and End Results.

In women, the incidence trends of ESCC seem to have been influenced by both calendar-period and birth-cohort effects in most countries, including Australia (five regions), Croatia, Finland, Slovenia, Sweden, the United Kingdom (three regions), and the United States (SEER 9; Table S2). However, the increasing incidence in Norwegian women was due to a calendar-period effect (P=0.046), especially in women aged 45–70 years (Table S2, ). A birth-cohort effect was indicated behind the increasing incidence in the Netherlands (P<0.001), Switzerland (P=0.014), and Japan (three regions; P<0.001; Table S2). An increased annual percentage change was found in women older than 60 years in the Netherlands and Switzerland, and in women aged 45–64 years in Japan (three regions; ). The birth-cohort-specific relative risk was >1 in Japan (three regions) and Norway in recent cohorts compared with the reference cohort, but <1 in the Netherlands and Switzerland (Figure S2).
Ethnicity
The incidence of ESCC in the United States (SEER 9 and 18) was higher in black men and women than in white, Asian, Pacific Islander, American Indian, or Alaska Native groups ().
Figure 4 Age-standardized incidence rates of esophageal squamous cell carcinoma in the United States by ethnicity in men (A) and women (B).
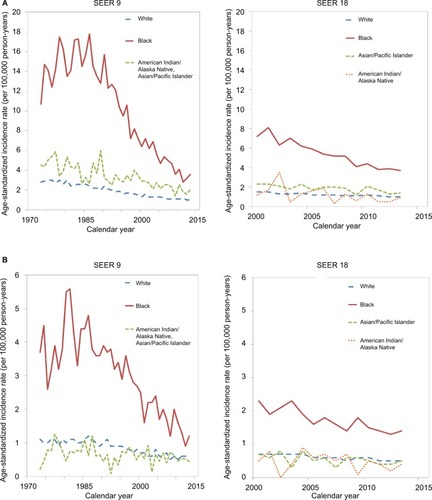
In men, the incidence in blacks increased from the year 1973 and peaked in 1986 (17.8/100,000 person-years), followed by a steady decrease to 3.6/100,000 person-years in 2013. In white, Pacific, or Alaskan men, low incidence rates (<3.0/100,000 person-years) in the 1970s were followed by a further slight decrease throughout the study period ().
In women, black women had an incidence rate of 1.4/100,000 person-years and white and Pacific or Alaskan women had an incidence of 0.5/100,000 person-years in 2013 (). A relatively high incidence was found in black women in 1977–1992, peaking in the year 1981 at 5.6/100,000 person-years, and declining from 1993 onwards. In white and Pacific or Alaskan women, the incidence was low and continued to slightly decrease during the study period ().
Discussion
This global assessment of the recent incidence trends of ESCC showed a generally decreasing incidence in men during the last decade, although it is still high in some populations, including Japan (three regions), France (Calvados), and China (Hong Kong). The incidence is generally lower in women than in men, but some countries have increased incidence in women – that is, Japan (three regions), the Netherlands, New Zealand, Norway, and Switzerland. The incidence has decreased more rapidly in blacks than in other ethnicities in the United States.
A decreasing incidence of ESCC globally in men has been reported previously,Citation6,Citation11–Citation19 and the present study indicated a continuous decrease during recent years. A study using incidence data from 12 countries in 1988–2007 predicted a continuing decrease in the incidence of ESCC in men worldwide, except in Japan, and increasing trends in women in Japan, the Netherlands, Slovakia, and Spain.Citation20 That prediction is supported by the updated results of the present study. Increased incidence trends in men have been reported in England, the Netherlands, Scotland, and the Nordic countries during the 1980s–1990s;Citation6,Citation15,Citation16,Citation21 however, the present study shows that the incidence decreased after the 2000s in these countries. In women, previous studies have reported stable or slightly increasing incidence rates in France, Italy, Norway, Slovenia, and Switzerland before the 2000s,Citation6,Citation11,Citation12,Citation16,Citation19 and these trends continued in 2005–2015 in the present study. A slightly increasing incidence has been reported in Swedish and Scottish women in 1980–1997;Citation15 however, after this period, the incidence has continued to decrease.
The increasing incidence of ESCC in women in some countries deserves attention. Increased use of endoscopy and improved registration systems might have resulted in an artificially increased incidence due to earlier tumor detection, but it is unlikely that these factors differ between the sexes. Tumor misclassification should be limited and misclassification of ESCC with adenocarcinoma should be uncommon; the proportion of esophageal tumors with unspecified histology was <20% in almost all registries. Calendar-period effects were found in women in Norway, whereas birth-cohort effects were found in women in Japan, the Netherlands, and Switzerland and could have contributed to the increase. The age–period–cohort analysis indicated that the increasing incidence in women from Japan and Norway could continue during the coming decades, whereas the incidence in Dutch and Swiss women could decline. Additionally, changes in the prevalence of risk factor exposure may influence the increasing incidence rates in women in some countries. An increased prevalence of smoking has been reported in Swiss women (from 20.6% in 1980 to 26.1% in 1998), which could explain the increasing incidence until 2012, but this trend might change due to the sharp drop in tobacco smoking after 1998.Citation22 Dutch women have had a slight increase in smoking prevalence (from 23.4% to 25.9% in 1980–1990), and a moderate decrease after 1990, which corresponds to the increasing incidence of ESCC reported in the present study and a predicted future decreasing trend.Citation22 However, the increased incidence in Japanese women does not correspond with the stable prevalence of tobacco smoking (11.0–12.0% in 1980–2005).Citation22 On the other hand, the prevalence of alcohol consumption among Japanese women increased from 6.3% to 9.4% in 1989–1998,Citation23 which could contribute to the increase, particularly because the use of spirits, which is a stronger risk factor for ESCC than other alcoholic beverages, composed almost half of the total alcohol consumption in Japan.Citation24 In Norwegian women, the tobacco smoking prevalence was stable at 27.0% in 1980–1991 and decreased to 15.9% in 2010,Citation22 and the alcohol consumption has remained stable,Citation25 indicating a role for other factors in explaining the increasing incidence of ESCC.
The generally decreasing incidence trends of ESCC in men from around the 1990s onwards could be explained by the globally declining smoking prevalence in men since 1980.Citation22,Citation26 Additionally, the trends in alcohol consumption have been decreasing or stable from 1980s onwards.Citation27,Citation28 The increasing incidence of ESCC in Japan over time before 2005 is in contrast to the decreasing smoking prevalence,Citation22,Citation23 but can be explained by the increasing prevalence of alcohol consumption.Citation28
The higher incidence of ESCC in black men than in other ethnicities in the United States could be explained by the higher smoking prevalence compared with other ethnicities.Citation29 The decreasing incidence in all ethnicities assessed is in accordance with the declining smoking prevalence in the United States.Citation22 However, in black women, the smoking prevalence is similar to that of white women and the alcohol consumption is lower.Citation30 The distinct incidence time trends among women of different ethnic groups might be explained by other factors (eg, diet).Citation31,Citation32
To the best of our knowledge, this is the most comprehensive and updated study examining the global incidence trends of ESCC. Strengths include the direct data collection from cancer registries of high quality and completeness.Citation7 Moreover, the age–period–cohort analysis enabled assessment of calendar-period-specific and birth-cohort-specific effects. The lack of nationwide registries in some included countries is among the limitations of this study. Therefore, merging of data from regional registries within the same country was applied. The fact that the registries covered entire countries or large regions meant that we could not separate rural and urban areas. Another limitation was that data on histological tumor type was not accessible from China, except for Hong Kong. The lack of individual data from cancer registries on risk factors (eg, regarding tobacco smoking and alcohol consumption) prohibited direct analyses of potential reasons for the observed change in incidence trends of ESCC, which however were indirectly analyzed and indicated by the age– period–cohort model in the study.
Monitoring the incidence trends of ESCC is of importance for future research and may have public health implications. Tobacco control activities have contributed to the decreasing incidence trends of ESCC in several countries (eg, in Hong Kong, the United States, and several European countries).Citation4,Citation14,Citation33 However, more efforts toward alcohol control are proposed, not least in Eastern countries, including Japan.Citation28 Despite the decreasing incidence of ESCC in most countries, the incidence remains high in many populations, and the increasing incidence in women in some countries is worrisome.Citation3
Conclusion
The global incidence of ESCC is decreasing in men, but increasing in women in Japan (three regions), the Netherlands, New Zealand, Norway, and Switzerland. An emphasis on continuous monitoring of the changing epidemiology of ESCC and prioritization of primary prevention of risk factors, including tobacco and alcohol control, is recommended in several populations, not least in women.
Acknowledgments
This work was supported by the Swedish Research Council (521-2014-2536) and the Swedish Cancer Society (CAN 2015/460). The study sponsors had no role in the study design; collection, analysis, and interpretation of data; the writing of the report; or the decision to submit the manuscript for publication. All of the authors appreciate the assistance in data retrieval from the following persons or registries (presented in alphabetical order):
Dr. Amani Elbasmi (Kuwait Cancer Registry); Mr. Andrew Deas (Scottish Cancer Registry); Ms. Anita Feller (National Institute for Cancer Epidemiology and Registration, Switzerland); Mr. Brian Stokes (Tasmanian Cancer Registry (Australia); Mr. Chris Lewis (New Zealand Cancer Registry); Cancer Institute New South Wales (Australia); Mr. Edrun Andrea Schnell (Cancer Registry of Norway); Ms. Elizabeth Chalker and Ms. Leah Newman (Australian Capital Territory Cancer Registry, Australia); Finnish Cancer Registry; Prof. Imjai Chitapanarux (Chiang Mai Cancer Registry, Thailand); Dr. Jaume Galceran (Tarragona Cancer Registry, Spain); Ms. Jennifer Lai (Public Health England, United Kingdom); Mr. J. Ramón Quirós (Asturias Cancer Registry, Spain); Dr. Katina D’Onise (South Australian Cancer Registry, Australia); Dr. Kotaro Ozasa (Tumor and Tissue Registry Office Hiroshima, Japan); Prof. Laufey Tryggvadottir (Icelandic Cancer Registry, Iceland); Dr. Manuel Zorzi (Veneto Tumor Registry, Italy); Dr. María José Sánchez Pérez (Granada Cancer Registry, Spain); Dr. Mario Šekerija (Croatian National Cancer Registry); Public Health Wales, United Kingdom; Dr. Roger K.C. Ngan (Hong Kong Cancer Registry, China); Mr. Sander Hogewoning (Netherlands Cancer Registry); Dr. Sandra Deady (National Cancer Registry, Ireland); Dr. Seiki Kanemura (Miyagi Prefectural Cancer Registry, Japan); Surveillance, Epidemiology, and End Results Program, United States; Swedish Cancer Registry; Dr. Timothy Threlfall (Western Australian Cancer Registry, Australia); Dr. Véronique Bouvier (Registre des Tumeurs Digestives du Calvados, France); Prof. Vesna Zadnik (Cancer Registry of Republic of Slovenia); and Dr. Yuko Akazawa (Nagasaki Prefectural Cancer Registry, Japan).
The study has used data from the Cancer Registry of Norway. The interpretation and reporting of these data are the sole responsibility of the authors, and no endorsement by the Cancer Registry of Norway is intended nor should be inferred.
Disclosure
All authors report no conflicts of interest in this work.
References
- Global Burden of Disease Cancer CollaborationFitzmauriceCDickerDPainAThe Global Burden of Cancer 2013JAMA Oncol20151450552726181261
- ArnoldMSoerjomataramIFerlayJFormanDGlobal incidence of oesophageal cancer by histological subtype in 2012Gut201564338138725320104
- LagergrenJSmythECunninghamDLagergrenPOesophageal cancerLancet2017390101102383239628648400
- XieSHLagergrenJTime trends in the incidence of oesophageal cancer in Asia: variations across populations and histological typesCancer Epidemiol201644717627504606
- ThriftAPWhitemanDCThe incidence of esophageal adenocarcinoma continues to rise: analysis of period and birth cohort effects on recent trendsAnn Oncol201223123155316222847812
- CastroCBosettiCMalvezziMPatterns and trends in esophageal cancer mortality and incidence in Europe (1980–2011) and predictions to 2015Ann Oncol201425128329024356640
- WHOCancer Incidence in Five Continents Volumes I to X, Indices of Data Quality2017 Available from: http://ci5.iarc.fr/CI5I-X/Pages/Quality_sel.aspxAccessed July 7, 2017
- SEER*Stat Database: Incidence – SEER 9 Regs Research Data, Nov 2015 Sub (1973–2013)2016 Available from: https://seer.cancer.gov/data-software/documentation/seerstat/nov2015/Accessed May 28, 2018
- SEER*Stat Database: Incidence – SEER 18 Regs Research Data + Hurricane Katrina Impacted Louisiana Cases, Nov 2015 Sub (2000–2013)2016 Available from: https://seer.cancer.gov/data-software/documentation/seerstat/nov2015/Accessed May 28, 2018
- RosenbergPSCheckDPAndersonWFA web tool for age-period-cohort analysis of cancer incidence and mortality ratesCancer Epidemiol Biomarkers Prev201423112296230225146089
- DesoubeauxNLe PrieurALaunoyGRecent time trends in cancer of the oesophagus and gastric cardia in the region of Calvados in France, 1978–1995: a population based studyEur J Cancer Prev19998647948610643936
- LaunoyGFaivreJPienkowskiPMilanCGignouxMPottierDChanging pattern of oesophageal cancer incidence in FranceInt J Epidemiol19942322462518082949
- YeeYKCheungTKChanAOYuenMFWongBCDecreasing trend of esophageal adenocarcinoma in Hong KongCancer Epidemiol Biomarkers Prev200716122637264018086768
- GiriSPathakRAryalMRKarmacharyaPBhattVRMartinMGIncidence trend of esophageal squamous cell carcinoma: an analysis of Surveillance Epidemiology, and End Results (SEER) databaseCancer Causes Control201526115916125376829
- BosettiCLeviFFerlayJTrends in oesophageal cancer incidence and mortality in EuropeInt J Cancer200812251118112917990321
- VizcainoAPMorenoVLambertRParkinDMTime trends incidence of both major histologic types of esophageal carcinomas in selected countries, 1973–1995Int J Cancer200299686086812115489
- FellerAFehrMBordoniATrends in incidence of oesophageal and gastric cancer according to morphology and anatomical location, in Switzerland 1982–2011Swiss Med Wkly2015145w1424526661828
- XieSHMattssonFLagergrenJIncidence trends in oesophageal cancer by histological type: an updated analysis in SwedenCancer Epidemiol20174711411728258029
- HansenSWiigJNGierckskyKETretliSEsophageal and gastric carcinoma in Norway 1958–1992: incidence time trend variability according to morphological subtypes and organ subsitesInt J Cancer19977133403449139864
- ArnoldMLaversanneMBrownLMDevesaSSBrayFPredicting the future burden of esophageal cancer by histological subtype: International Trends in Incidence up to 2030Am J Gastroenterol201711281247125528585555
- SteevensJBotterweckAADirxMJvan den BrandtPASchoutenLJTrends in incidence of oesophageal and stomach cancer subtypes in EuropeEur J Gastroenterol Hepatol201022666967819474750
- Tobacco Visualization Seattle, WA: IHME, University of Washington2017 Available from: https://vizhub.healthdata.org/tobacco/Accessed July 7, 2017
- Cancer Statistics in Japan-2016 Trends in Consumption of Tobacco, Alcohol and Food2016 Available from: http://ganjoho.jp/en/professional/statistics/brochure/2016_en.htmlAccessed July 7, 2017
- OzeIMatsuoKWakaiKResearch Group for the Development and Evaluation of Cancer Prevention Strategies in JapanAlcohol drinking and esophageal cancer risk: an evaluation based on a systematic review of epidemiologic evidence among the Japanese populationJpn J Clin Oncol201141567769221430021
- WHOGlobal Health Observatory (GHO) data: Global status report on alcohol and health2014Norway Available from: http://www.who.int/substance_abuse/publications/global_alcohol_report/profiles/nor.pdfAccessed July 7, 2017
- EnzingerPCMayerRJEsophageal cancerN Engl J Med2003349232241225214657432
- La VecchiaCBosettiCBertuccioPCastroCPelucchiCNegriETrends in alcohol consumption in Europe and their impact on major alcohol-related cancersEur J Cancer Prev201423431932224045697
- WHOGlobal Health Observatory data repository: recorded alcohol per capita consumption, 1980–1999 by country2017 Available from: http://apps.who.int/gho/data/node.main.A1024?lang=en&showonly=GISAHAccessed July 7, 2017
- TrinidadDRPérez-StableEJWhiteMMEmerySLMesserKA nationwide analysis of US racial/ethnic disparities in smoking behaviors, smoking cessation, and cessation-related factorsAm J Public Health2011101469970621330593
- JamalAHomaDMO’ConnorECurrent cigarette smoking among adults – United States, 2005–2014MMWR Morb Mortal Wkly Rep201564441233124026562061
- QuXBenQJiangYConsumption of red and processed meat and risk for esophageal squamous cell carcinoma based on a meta-analysisAnn Epidemiol20132312762770.e76124176821
- XieSHRabbaniSPetrickJLCookMBLagergrenJRacial and ethnic disparities in the incidence of esophageal cancer in the United States, 1992–2013Am J Epidemiol2017186121341135128641390
- LevyDTHuangATCurrieLMClancyLThe benefits from complying with the framework convention on tobacco control: a SimSmoke analysis of 15 European nationsHealth Policy Plan20142981031104224262281