
Abstract
Purpose
Updated estimates of incidence and prevalence of dementia are crucial to ensure adequate public health policy. However, most of the epidemiological studies in the population in Spain were conducted before 2010. This study assessed the validity of dementia diagnoses recorded in electronic health records contained in a large primary-care database to determine if they could be used for research purposes. Then, to update the epidemiology of dementia in Catalonia (Spain), we estimated crude and standardized prevalence and incidence rates of dementia in Catalonia in 2016.
Methods
The System for the Development of Research in Primary Care (SIDIAP) database contains anonymized information for >80% of the Catalan population. Validity of dementia codes in SIDIAP was assessed in patients at least 40 years old by asking general practitioners for additional evidence to support the diagnosis. Crude and standardized incidence and prevalence (95% CI) in people aged ≥65 years were estimated assuming a Poisson distribution.
Results
The positive predictive value of dementia diagnoses recorded in SIDIAP was estimated as 91.0% (95% CI 87.5%–94.5%). Age-and sex-standardized incidence and prevalence of dementia were 8.6/1,000 person-years (95% CI 8.0–9.3) and 5.1% (95% CI 4.5%–5.7%), respectively.
Conclusion
SIDIAP contains valid dementia records. We observed incidence and prevalence estimations similar to recent face-to-face studies conducted in Spain and higher than studies using electronic health data from other European populations.
Introduction
Dementia affects about 47 million people worldwide and is related to dependence, poor quality of life, institutionalization, and mortality.Citation1 Age is the main risk factor for dementia, and the world population is aging; therefore, the number of people affected by dementia is expected to increase to 131 million in 2050, resulting in huge social and economic costs.Citation1 Population-based epidemiological estimates of its prevalence and incidence is crucial to plan and budget health services and evaluate its economic burden. Therefore, robust and up-to-date estimates are needed to support the creation of useful public policies on dementia.Citation2 However, updated estimates of prevalence and incidence in the European population are scarce,Citation1 eg, in Spain, most of the studies collected data in the 1990s or 2000s, and to our knowledge, only four used data collected during the past 10 years.Citation3–Citation6 High economic costs of door-to-door surveys or questionnaire-based studies may contribute to the difficulty of updating estimates of prevalence and incidence of dementia.
Electronic health records emerged as a new opportunity to study the epidemiology of dementia: prevalence and incidence-rate estimates can be updated at low cost using data routinely collected in health care settings. Indeed, the use of electronic medical databases to assess the epidemiology of dementia has been increasing at the European levelCitation7 and in many developed countries, such as CanadaCitation8 and the Netherlands.Citation9 However, the accuracy of dementia records in routinely collected health care data sets is always a concern, and cohorts should ideally conduct their own setting-specific validation.Citation10 This concern is especially apparent for electronic health records collected in primary care, because accuracy of dementia diagnoses recorded by general practitioners has been considered low.Citation8,Citation11 Nevertheless, a recent systematic review reported high positive predictive values (PPVs) (0.83 or higher) when identifying dementia cases in primary-care data, indicating that dementia codes in those primary-care databases were sufficiently accurate to be used for research purposes.Citation10
We thus used data from a large primary-care database to describe the epidemiology of dementia in Catalonia, southern Europe. First, we assessed the validity of dementia diagnoses recorded in the database to determine if they could be used for research purposes. Then, we estimated crude and standardized prevalence and incidence rates of dementia in Catalonia in 2016, in order to update the epidemiological estimates.
Methods
This population-based study was approved by the Clinical Research Ethics Committee, Primary Care Research Institute – IDIAP Jordi Gol. Data were obtained from the System for the Development of Research in Primary Care (SIDIAP) database, which contains routine records of consultations from ~275 general-care practices belonging to the National Health Service of Catalonia (Institut Català de la Salut). SIDIAP contains anonymized longitudinal medical records containing data on demographics, symptoms, diagnoses, and prescriptions for about 6 million people (>80% of the Catalan population, 15% of the Spanish population).Citation12,Citation13 We defined dementia diagnoses using the following codes from the International Classification of Diseases, Tenth revision (ICD10): dementia in Alzheimer’s disease (F00), vascular dementia (F01), dementia in other diseases classified elsewhere (F02.8), unspecified dementia (F03), Alzheimer’s disease (G30), Lewy body disease (G31.8), or frontotemporal dementia (G31.0). SIDIAP is linked with the pharmacy-invoicing database provided by the National Health Service of Catalonia and medications are recorded using the Anatomical Therapeutic Chemical (ATC) codes. We considered as treated those patients who had a prescription or billing for anticholinesterases (N06DA) or memantine (N06D × 01). We used outcomes recorded in SIDIAP to describe dementia assessment in the Catalan primary-care system, because clinical practice might influence the identification of dementia cases, and this would affect estimates of prevalence and incidence rates.Citation10,Citation14 In particular, we identified the number of persons who were institutionalized, attended by the home-care program, had a record of cognitive assessment, or had a record of functional ability and independence assessment. Cognitive assessment was defined as at least one Mini-Mental Status ExaminationCitation15 or Pfeiffer testCitation16 (Spanish versions) score ≤23 or ≥3, respectively, considered to suggest cognitive impairment. Assessment of functional ability and independence was defined as at least one recorded score on the Barthel Index,Citation17 Lawton Scale,Citation18 Katz Index,Citation19 or Blessed Dementia Rating Scale.Citation20 Low functional ability or dependence was considered when the score was <90 on the Barthel Index, <3 in men and <5 in women on the Lawton Scale, ≥2 on the Katz Index, or ≥4 on the Blessed Dementia Rating Scale.
Validation of dementia diagnoses
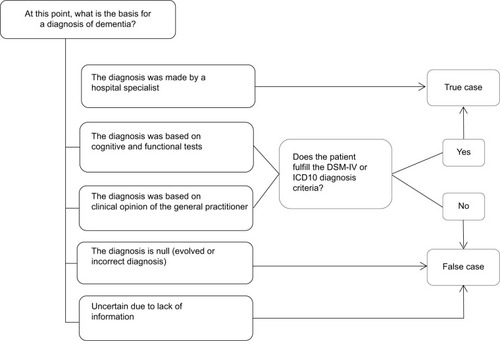
To assess accuracy of dementia diagnoses recorded in SIDIAP, we emailed a short survey to general practitioners asking about the current status of the diagnosis (), a method used previously in validations of dementia diagnosis.Citation21 We invited general practitioners of the Agency of Clinical Research Management in Primary Care (AGICAP), associated with the IDIAP Jordi Gol to participate in the validation study. AGICAP general practitioners received training and had experience in recruitment of patients in clinical trials and in review of diagnoses recorded in the electronic medical history. We emailed an online survey to general practitioners who agreed to participate, asking for further evidence to confirm the diagnosis of all their patients aged at least 40 years who had a dementia code recorded in SIDIAP (ICD10). The survey remained available online for 1 month for general practitioners to evaluate dementia diagnoses. In order to enhance the response rate, we offered a small monetary incentive and sent one follow-up email to nonresponding general practitioners to remind them to complete the questionnaire. The online survey examined whether or not the diagnosis was made by a specialist, whether or not the diagnosis fulfilled the Diagnostic and Statistical Manual of Mental Disorders (DSM) IV or ICD10 diagnosis criteria, which symptoms were observed, subtype and severity of dementia, and if the diagnosis was considered to be incorrect, evolved, or uncertain due to incomplete information (). When applicable, additional information about the score achieved in cognitive and functional tests was requested (). We defined patients as true cases if they were diagnosed by a specialist (eg, neurologist or psychiatrist), by cognitive or functional tests, or by clinical opinion of the general practitioner and DSM-IV or ICD10 diagnostic criteria were fulfilled (). Patients were defined as false cases when the diagnosis was considered by the general practitioner not to fulfill DSM-IV or ICD10 diagnostic criteria, was based on inconsistent evidence, had evolved, or was incorrect ().
Figure 1 Definition of true and false cases of dementia.
Incidence and prevalence
The study population included patients aged at least 65 years who were registered in SIDIAP. We defined a case as any patient having an ICD10 diagnosis of dementia or an ATC code of pharmacological treatment related to dementia recorded in SIDIAP. In Catalonia, the prescription of antidementia drugs is requested by the general practitioner, but until 2014 required approval from the advisory board, a group of experts who evaluated all patients with dementia recommended for pharmacological treatment. Since 2014, approval has been determined by a geriatrician, psychiatrist, or neurologist. Since all treated patients had been evaluated previously by specialists, we considered them true cases. To estimate the incidence rate, persons who were alive in 2016 according to SIDIAP records were included. Incident cases were defined as dementia patients diagnosed or treated during 2016. Patients diagnosed with dementia or treated with antidementia drugs before January 1, 2016 were excluded. To estimate dementia prevalence, persons who had SIDIAP records and were alive as of December 31, 2016 were included. Patients who moved away or died before that date were excluded. Prevalent cases were defined as patients diagnosed or treated as of December 31, 2016.
Statistical analyses
We estimated PPV and 95% CI of dementia diagnosis using data from the survey of general practitioners. PPV is an indicator of the probability that a person with a record of dementia diagnosis in SIDIAP truly had the disease. A higher PPV indicated better accuracy of the dementia records in SIDIAP. PPV was defined as the number of confirmed diagnoses of dementia (numerator) against all the diagnoses of dementia evaluated by general practitioners using the questionnaire (denominator). Results were stratified by sex and age-group. We also performed sensitivity analyses to explore the robustness of our results. By extrapolating figures to the worst-case scenario, we replicated the analyses considering both evaluated and unevaluated diagnoses of dementia. PPV was replicated, including in the numerator all diagnoses of dementia confirmed by the general practitioners or with evidence of treatment with antidementia drugs, and in the denominator all recorded diagnoses of dementia included in the validation study (evaluated or not by general practitioners).
To describe the study population and primary-care settings, we used percentages for categorical variables and means (SD) or medians (IQR) for continuous variables. We estimated overall crude prevalence and incidence rates, and 95% CI was calculated assuming a Poisson distribution. We stratified the prevalence and incidence estimates by sex and age-group. We used the direct method to estimate age-and sex-standardized prevalence and incidence of dementia. The 2013 revision of the European standard population served as the basis for adjustment (EU27/European Free Trade Association standard population:Citation22 weights of 0.28, 0.26, 0.21, 0.13, 0.08, and 0.05 for age-groups 65–69, 70–74, 75–79, 80–84, 85–89, and ≥90 years, and 0.5 for both men and women). We used the official 2015 population estimate of 11,045,521 citizens in Spain aged ≥65 years (http://www.ine.es).
Finally, we calculated age-standardized rates for women and men and sex-standardized rates for age-groups separately. We used the likelihood-ratio test to examine the age–sex interaction. All analyses were performed using R software version 3.5.2.Citation23
Results
Validation of dementia diagnoses
Surveys were sent to 42 general practitioners, of which 29 participated in the validation study (response rate 69%). These 29 general practitioners had records of 374 patients with a dementia diagnosis, of which 256 diagnoses were evaluated during the 1-month validation period. Among the 118 unevaluated dementia diagnoses, 58 of the patients were treated with antidementia drugs and 60 were untreated. General practitioners evaluated 256 dementia diagnoses and considered 233 true cases: 209 patients diagnosed by a specialist and 24 patients who fulfilled the DSM-IV or ICD10 diagnostic criteria. We identified 23 false cases: 21 considered evolved, incorrect, or uncertain diagnoses and two not fulfilling DSM-IV or ICD10 diagnostic criteria. Therefore, the PPV of dementia codes registered in SIDIAP was 91.0% (95% CI 87.5%–94.5%). Results stratified by age and sex provided similar results: PPV was estimated as 89.8% (95% CI 85.2%–94.4%) for women (n=166), 93.3% (95% CI 88.1%–98.5%) for men (n=90), 90.3% (95% CI 85.6%–95.0%) for persons aged <80 years (n=154), and 92.1% (95% CI 86.9%–97.3%) for persons at least 80 years old (n=102).
General practitioners evaluated 128 diagnoses of patients who had both a diagnosis and pharmacological treatment for dementia recorded in SIDIAP, and 99% of these were confirmed as true cases. We replicated the PPV estimates, adding the unevaluated cases as true cases if the diagnosed patient had been treated with antidementia drugs or as false cases if they had not been treated. In this worst-case scenario, the PPV estimate included 291 true cases in the numerator (233 dementia diagnoses evaluated and confirmed by general practitioners, and 58 unevaluated dementia diagnoses in patients being treated for the disease) and 374 dementia diagnoses in the denominator (256 evaluated by general practitioners and 118 unevaluated). The resulting PPV was 77.8% (95% CI 73.6%–82.0%).
Incidence and prevalence
For 2016, we obtained data for 1,035,046 persons, mainly women (56.2%), from urban areas (80.9%) and 75.7 (7.9) years old on average. We obtained 1,008,755 person-years and detected 9,596 incident cases, of which 8,553 had been diagnosed and 1,043 undiagnosed but treated with antidementia drugs. provides further details of the population studied to estimate incidence rates. The crude incidence of dementia was estimated at 9.5/1,000 person-years (95% CI 9.3–9.7), sex-standardized incidence at 9.3/1,000 person-years (95% CI 9.0–9.6), age-standardized incidence at 8.8/1,000 person-years (95% CI 8.4–9.2), and age-and sex-standardized incidence at 8.6/1,000 person-years (95% CI 8.0–9.3). The incidence rate was higher among women than men, and increased with age: it was about 25 times higher in people older than 90 years than in people aged 65–69 years (). We found a significant age–sex interaction (P<0.001), and age-related increase in incidence was more pronounced in women than in men (, ).
Figure 2 Incidence rate (A) and prevalence (B) of dementia.
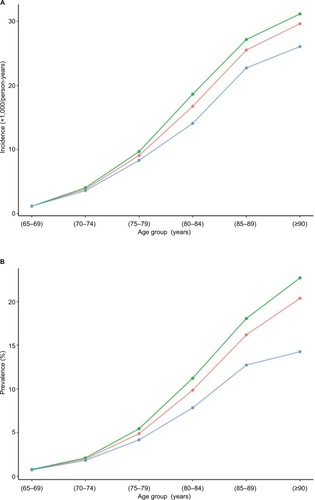
Table 1 Crude and standardized incidence rates of dementia (per 1,000 person-years) in people aged ≥65 years in Catalonia (Spain) in 2016, stratified by sex and age
To estimate dementia prevalence, we obtained data on 1,048,956 persons recorded in SIDIAP on December 31, 2016. Participants were mainly women (57.2%) and predominantly from urban areas (80.9%). Mean (SD) age was 75.9 (7.9) years. shows the medical conditions of the study population used to estimate dementia prevalence. We found 63,117 prevalent cases, of which 55,951 had been diagnosed and 7,166 undiagnosed but treated with antidementia drugs. The median duration of dementia in prevalent cases was 3.77 (IQR 1.67–6.50) years. describes the dementia assessment in the Catalan primary settings. We estimated crude prevalence as 6.0% (95% CI 6.0%–6.1%), sex-standardized prevalence 5.8% (95% CI 5.7%–5.9%), age-standardized prevalence 5.3% (95% CI 5.0%–5.6%), and both sex-and age-standardized prevalence 5.1% (95% CI 4.5%–5.7%). Dementia prevalence was higher in women than men and increased with age (). The age-related increase in prevalence was significantly higher in women than in men, with a P-value <0.001 for the age–sex interaction (, ).
Table 2 Description of the characteristics of the primary care settings in Catalonia (Spain) in relation to dementia assessment
Table 3 Crude and adjusted prevalence of dementia in people aged ≥65 years in Catalonia (Spain) in 2016, stratified by sex and age
Discussion
This large-scale nationwide study of >1 million cases provides a comprehensive update of the epidemiology of dementia in southern Europe. Our findings highlighted that records of dementia diagnoses routinely collected in primary care and registered in SIDIAP are accurate enough to be used for research purposes. Moreover, we provided a detailed update about crude and standardized prevalence and incidence rates, which may help to improve policies related to dementia not only in primary-care settings but also in secondary care.
Validation of dementia diagnoses
We found a 91% PPV of diagnoses of dementia recorded in SIDIAP. Sensitivity analyses showed that in the worst scenario, the PPV would be 77.8%. Our PPV estimate was slightly higher than values observed in previous studies that assessed the quality of routinely collected data on dementia in primary-care services for research purposes.Citation10,Citation24,Citation25 When routinely collected electronic health records are applied to research, avoiding false-positive diagnoses could be more important than avoiding false negatives. In longitudinal studies, for example, false positives can dilute observed effects and reduce statistical power.Citation26 Our results highlighted that false positives on dementia cases are scarce in SIDIAP and that patients having a record in SIDIAP of a diagnosis of dementia are very likely to have the disease. Therefore, the SIDIAP database is valid for epidemiological research on dementia.
Incidence and prevalence
We estimated an age-and sex-standardized incidence of 8.6/1,000 person-years (95% CI 8.0–9.3), similar to the adjusted incidence estimated by the NEDICES study on the Spanish population aged ≥65 years.Citation27 Other studies conducted in Spain have reported disparate estimates of dementia incidence.Citation28,Citation29 However, differences in study populations and methodologies limit comparability with our findings. When comparing incidence of dementia according to age-group, our estimations were similar to those reported by Bermejo-Pareja et alCitation27 and Lobo et alCitation28 in all age-groups except the oldest old (aged at least 85 years), in which our values were lower than the face-to-face studies cited. This disparity might be partially due to some level of underrecording in SIDIAP, mainly concentrated in the oldest-old patients, in line with previous studies.Citation30 Some general practitioners may consider memory difficulties part of the normal aging process, rather than a disability that requires specialist care and support,Citation31 while others might be reluctant to use dementia codes in this age-group because they consider the diagnosis and treatment of dementia useless.Citation8,Citation31
We estimated the age-and sex-standardized prevalence of dementia as 5.1% (95% CI 4.5%–5.7%), which overlapped with the standardized estimations reported by the the most recent face-to-face studies in the Spanish population at least 65 years old.Citation4,Citation5 Previous face-to-face studies – mostly conducted before 2010 – reported crude prevalence estimates, ranging from 5.5% to 14.9% in Spanish people aged ≥65 years.Citation32–Citation35 At the European level, age-and sex-standardized prevalence of dementia was estimated at 6.4% by a collaborative study of population-based cohorts conducted in the 1990s,Citation36 7.3% by a meta-analysis that integrated studies conducted from 1980 until 2004,Citation37 and 7.1% based on a meta-analysis on data obtained mainly during the 1990s and 2000s.Citation38 More recent national estimates have been 6.5% in the UK,Citation39 3.65% in Portugal,Citation40 or 5.0% in Greece.Citation41 Our prevalence estimation fell in the lower range of published results from the 1990s and early 2000s in face-to-face studies in Spain and in the European population, and were in line with the most recent estimations. The prevalence of dementia has been reported to be decreasing in high-income countries,Citation42 the USA,Citation43 the UK,Citation39 and Spain.Citation44 However, comparisons between studies are difficult to make, because of methodological differences. Therefore, it is plausible that our 2016 estimates reflect a reduction in dementia cases since the 1990s or 2000s, but we cannot reject other explanations. Population characteristics could be a factor. For example, most of the population in Catalonia is bilingual in Catalan and Spanish. Bilingualism may contribute to cognitive reserve and protect against the onset of dementia,Citation45 and could have affected our estimates. SIDIAP does not provide data on languages spoken by patients.
Electronic health records
In a comparison with other studies based on electronic health records, our findings provided new insights about the epidemiology of dementia. Our results were similar to those reported by a study that used diagnoses and drug-prescription data from primary-care and pharmacy electronic databases to estimate unadjusted prevalence as 5.91% (95% CI 5.85%–5.95%) in persons at least 65 years old living in Madrid in 2011.Citation6 However, our estimates were higher than previous studies in other European populations. A Danish study estimated the prevalence of dementia at 3.8% using electronic health records from secondary-care settings.Citation46 Another study, by Perera et al, compiled data from six electronic health-record systems, including both primary and secondary care from different European countries, to estimate prevalence and incidence rates of dementia.Citation7 They reported lower incidence and prevalence estimates in all age-groups than the ones we observed. Such differences remained for estimates restricted to data from primary-care settings, which contained fewer dementia cases than SIDIAP. These differences might be partially explained by methodological issues, demographic aspects, and characteristics of primary-care settings. Our methodology applied a mixed definition of dementia that included not only diagnosis but also prescription or billing of antidementia drugs. This broader definition might capture more dementia cases than that used by Perera et al, who identified cases using only diagnostic codes or free text.Citation7 Demographic aspects might also contribute to explaining differences between primary-care databases from different countries. Life expectancy in Spain is the longest in the EU (83.3 years),Citation47 and the sex gap in life expectancy favors women to a higher extent than in other countries, such as Denmark, the Netherlands, or the UK.Citation47 Since dementia prevalence is higher in women and increases with age, demographic characteristics of the population might facilitate a higher number of dementia cases in Spain than in other European countries. Primary-care characteristics might also contribute to explaining disparities between studies on dementia epidemiology based on electronic health records from primary care. Catalan primary-care settings from which SIDIAP obtained data might be highly sensitive in diagnosing dementia cases. On one hand, cognitive tests are administered widely to identify dementia cases in the Catalan primary-care system: in SIDIAP, >22% of patients with no dementia code in their electronic health history had taken a cognitive test. Patients with memory complaints reported by themselves, their relatives, or general practitioners are asked to take a cognitive test. Patients included in specific programs for home care or institutionalized due to chronic complex disease may also be asked to complete a cognitive test, even if they have no memory or cognitive complaints. The huge number of cognitive tests administered in Catalan primary care might facilitate the identification of new dementia cases.Citation14 On the other hand, we found that most patients with a dementia code in SIDIAP had been diagnosed by a specialist or prescribed antidementia drugs by specialists. These findings suggest a good coordination between primary and secondary settings provided by the Catalan Health Institute, strengthened by such initiatives as the Computerized Support System for the Diagnosis of Dementia in Primary Care (SISDDAP [Catalan acronym]), an asynchronous telemedicine program involving both primary-and specialized-care professionals that establishes protocols for the screening and diagnosis of dementia.Citation48 Appropriate communication and coordination between primary and secondary care might facilitate the identification of new dementia cases and the recording of diagnoses in the electronic health record. Our findings are in line with previous literature reporting that settings with active dementia-diagnosis centers are likely to see a higher proportion of community cases in health care databases.Citation7 Our findings also suggested that the high level of underdiagnosis of dementia reported in several primary-care systemsCitation31,Citation49 might not be true for other primary-care settings. General practitioner concern and training, as well as programs and policies designed to better diagnose dementia cases, might help to reduce underdiagnosis in primary care. Therefore, databases containing routinely collected data from primary care might be a powerful tool to study dementia epidemiology if data have been recorded in a setting with active management of dementia cases and validated as sufficiently accurate for research purposes.
Limitations and strengths
We acknowledge several limitations. First, the PPV could have been overestimated, because the validation study was constrained to general practitioners from the AGICAP network, who are regularly involved in clinical trials and thus could be more prone to register diagnoses accurately in electronic medical records. Second, as not all dementia diagnoses were evaluated by general practitioners, we cannot discard a potential bias that might have resulted in an overestimation of the PPV. Therefore, we replicated the PPV estimate considering the worst-case scenario, in which data from both evaluated and unevaluated dementia diagnoses were used. This worst-case scenario PPV estimate would indicate the minimum value of the PPV, ie, if bias had occurred and the PPV value had been overestimated, the PPV would not be lower than the worst-case scenario estimate. Third, the validation study did not provide sensitivity estimates of dementia diagnoses recorded in SIDIAP: it was cost-prohibitive to search for cases in persons with no recorded dementia diagnosis in SIDIAP. However, sensitivity has been reported to be less crucial than PPV in evaluating the accuracy of routinely collected health data, because the effects of false negatives would be diluted among the large control population.Citation10 Moreover, our prevalence estimates were quite similar to those reported by clinical studies in Spain during the last decade, and a decreasing trend in prevalence figures has been observed in high-income countries.Citation42 All this suggests that the recording of dementia diagnoses in SIDIAP is satisfactory. Fourth, we did not use free text to improve identification of persons with dementia. However, we used a mixed definition of dementia cases that included diagnosis and prescription or billing codes involving not only data from the general practitioner but also from the pharmacy-invoicing database. Using two different data sources minimized the possible effect of underrecording of dementia diagnoses in SIDIAP. Finally, a lower education level has been associated with a greater risk of dementia.Citation50 We could not stratify the results according to literacy, since this information is unavailable in SIDIAP.
Our study has several strengths. First, it included about 10,000 incident cases in 1 year and 63,000 prevalent cases, while most epidemiological studies on dementia conducted in Western Europe had smaller samples.Citation1 Second, our study did not depend on participants’ response rate, and thus was not affected by selection bias due to lack of response, which can be common among people with dementia due to reluctance of relatives to participate or difficulties in completing the questionnaires.Citation1 Finally, this was a nationwide study that included >1 million people in Catalonia, a 32,000 km2 region of southern Europe. Therefore, this study provides better representation of the Spanish population than previous studies conducted in a single cityCitation5,Citation34,Citation44,Citation51 or a limited area. The nationwide approach may facilitate the design and implementation of new dementia policies in national health systems.
Conclusion
Dementia diagnoses recorded in the SIDIAP database are valid to be used for research purposes. Age-and sex-standardized prevalence and incidence rates of dementia in 2016 were higher for women and the oldest-old population. Our figures were in line with the most recent studies conducted in Spain and higher than those provided by other primary-care databases from other European countries. These findings may be helpful to plan dementia policies not only in primary-care settings but also in secondary care and in the overall public health system.
Acknowledgments
We thank the Registre del Conjunt Mínim de Bases de Dades (CMBD), Divisió de Registres de Demanda i d’Activitat, Àrea de Serveis i Qualitat, Servei Català de la Salut for providing data on hospital discharges. We also thank Eduardo Hermosilla for data-management support and Elaine Lilly for revision of the English text. This work was supported by the Real world Outcomes across the Alzheimer’s Disease spectrum for better care: Multi-modal data Access Platform (ROADMAP) from the Innovative Medicines Initiative (grant agreement 116020). This project was also supported by clinical research grants from Carlos III Health Institute, within the Net for Research in Preventive Activities and Health Enhancement (RedIAPP RD16/0007/0004) framework, and from the Agency for Management of University and Research Grants (2017 SGR 1146).
Supplementary material
Figure S1 Summary of questionnaire for the validation of dementia diagnosis.
Abbreviations: CIE-10, Código Internacional de Enfermedades (Spanish version of the ICD); DSM, Diagnostic and Statistical Manual of Mental Disorders.
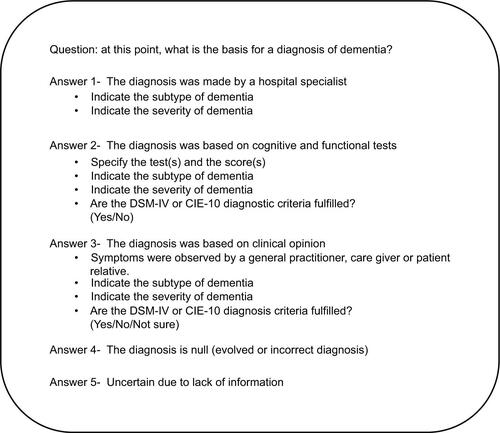
Table S1 Characteristics of study population to estimate incidence rate of dementia
Table S2 Crude incidence rates of dementia (per 1,000 person-years) in people aged ≥65 years in Catalonia (Spain) in 2016, stratified by sex and age
Table S3 Characteristics of study population to estimate dementia prevalence that includes persons aged ≥65 years registered in SIDIAP on December 31, 2016
Table S4 Crude prevalence of dementia in people aged ≥65 years in Catalonia (Spain) in 2016, stratified by sex and age
Disclosure
The authors report no conflicts of interest in this work.
References
- Martin PrinceAWimoAGuerchetMWorld Alzheimer report 2015 the global impact of dementia an analysis of prevalence, incidence, cost and trends2015 Available from: https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdfAccessed June 14, 2017
- WuYTFratiglioniLMatthewsFEDementia in Western Europe: epidemiological evidence and implications for policy makingLancet Neurol201615111612426300044
- Virués-OrtegaJde Pedro-CuestaJVegaSPrevalence and European comparison of dementia in a ≥75-year-old composite population in SpainActa Neurol Scand2011123531632420636450
- Rodríguez-SánchezEMora-SimónSPatino-AlonsoMCPrevalence of cognitive impairment in individuals aged over 65 in an urban area: DERIVA studyBMC Neurol201111114722093337
- Tola-ArribasMAYuguerosMIGareaMJPrevalence of dementia and subtypes in Valladolid, northwestern Spain: the DEMINVALL studyPLoS One2013810e7768824147055
- de Hoyos-AlonsoMCBonisJTapias-MerinoECastellMVOteroAEstimación de la prevalencia de demencia a partir del análisis de bases de datos sobre uso de fármacos. La situación en La Comunidad de Madrid (España)Neurología20163111825444413
- PereraGPedersenLAnselDDementia prevalence and incidence in a Federation of European electronic health record databases—the European medical informatics framework resourceAlzheimers Dement201814213013928734783
- DrummondNBirtwhistleRWilliamsonTKhanSGariesSMolnarFPrevalence and management of dementia in primary care practices with electronic medical records: a report from the Canadian primary care sentinel surveillance networkCMAJ Open201642E177E184
- van BusselEFRichardEArtsDLDementia incidence trend over 1992-2014 in the Netherlands: analysis of primary care dataPLoS Med2017143e100223528267788
- WilkinsonTLyASchnierCIdentifying dementia cases with routinely collected health data: a systematic reviewAlzheimers Dement20181481038105129621480
- Zunzunegui PastorMVSerT delRodríguez LasoAGarcía YébenesMJDomingoJOtero PuimeADemencia no detectada y utilización de los servicios sanitarios: implicaciones para la atención primaria TT-Non-detected dementia and use of the health services: implications for primary careAten Primaria200331958158612783748
- BolíbarBFina AvilésFMorrosR[SIDIAP database: electronic clinical records in primary care as a source of information for epidemiologic research]Med Clin (Barc)201213814617621 Spanish22444996
- García-GilMMHermosillaEPrieto-AlhambraDConstruction and validation of a scoring system for the selection of high-quality data in a Spanish population primary care database (SIDIAP)Inform Prim Care201119313514522688222
- EichlerTThyrianJRHertelJRates of formal diagnosis of dementia in primary care: the effect of screeningAlzheimers Dement (Amst)201511879327239495
- LoobASazPMarcosGRevalidation and standardization of the cognition mini-exam (first Spanish version of the Mini-Mental status examination) in the general geriatric populationMed Clin (Barc)19991122076777410422057
- Martínez de la IglesiaJDueñas HerreroROnís VilchesMCAguado TabernéCAlbert ColomerCLuque LuqueRSpanish language adaptation and validation of the Pfeiffer’s questionnaire (SPMSQ) to detect cognitive deterioration in people over 65 years of ageMed Clin (Barc)2001117412913411472684
- BaztánJPérez del MolinoJAlarconTSan CristóbalEIzquierdoGManzarbeitiaIIndice de Barhtel: instrumento válido para la valoración funcional de pacientes con enfermedad cerebrovascular [Barthel index: a valid instrument for the functional assessment of patients with cerebrovascular disease]Rev Esp Geriatr Gerontol1993283240 Spanish
- LawtonMPBrodyEMAssessment of older people: self-maintaining and instrumental activities of daily livingGerontologist1969931791865349366
- Alvarez SolarMAtDARGurpeguiBCapacidad funcional de pacientes mayores de 65 años, según El Indice de Katz [Functional ability of patients aged 65 years or older according to the Katz index]Aten Primaria1992108128151457702
- BlessedGTomlinsonBERothMThe association between quantitative measures of dementia and of senile change in the cerebral grey matter of elderly subjectsBr J Psychiatry19681145127978115662937
- BrownAKirichekOBalkwillAComparison of dementia recorded in routinely collected hospital admission data in England with dementia recorded in primary careEmerg Themes Epidemiol2016131127800007
- European CommissionRevision of the European Standard Population. Report of Eurostat’s Task ForceLuxemburg2013 Available from: https://ec.europa.eu/eurostat/documents/3859598/5926869/KS-RA-13-028-EN.PDF/e713fa79-1add-44e8-b23d-5e8fa09b3f8fAccessed February 7, 2019
- R Development Core TeamR: A Language and Environment for Statistical Computing2018R Foundation for Statistical ComputingVienna, Austria Available from: https://www.R-project.org/Accessed February 7, 2019
- WilliamsonTMiyagishimaRCDerochieJDDrummondNManual review of electronic medical records as a reference standard for case definition development: a validation studyCMAJ Open201754E830E833
- JaakkimainenRLBronskillSETierneyMCIdentification of Physician-Diagnosed Alzheimer’s disease and related dementias in population-based administrative data: a validation study using family physicians’ electronic medical recordsJ Alzheimers Dis201654133734927567819
- HerrettEShahADBoggonRCompleteness and diagnostic validity of recording acute myocardial infarction events in primary care, hospital care, disease registry, and national mortality records: cohort studyBMJ20133463f235023692896
- Bermejo-ParejaFBenito-LeónJVegaSMedranoMJRománGCNeurological Disorders in Central Spain (NEDICES) Study GroupIncidence and subtypes of dementia in three elderly populations of central SpainJ Neurol Sci20082641–2637217727890
- LoboALopez-AntonRSantabárbaraJIncidence and lifetime risk of dementia and Alzheimer’s disease in a southern European populationActa Psychiatr Scand2011124537238321848704
- López-PousaSVilalta-FranchJLlinàs-ReglaJGarre-OlmoJRománGCIncidence of dementia in a rural community in Spain: the Girona cohort studyNeuroepidemiology200423417017715272219
- SkinnerTScottIMartinJDiagnostic errors in older patients: a systematic review of incidence and potential causes in seven prevalent diseasesInt J Gen Med2016913714627284262
- LangLCliffordAWeiLPrevalence and determinants of undetected dementia in the community: a systematic literature review and a meta-analysisBMJ Open201772e011146011148
- PiJOlivéJMRocaJMasanaLPrevalence of dementia in a semi-rural population of Catalunya, SpainNeuroepidemiology199615133418719047
- GavrilaDAntúnezCTormoMJPrevalence of dementia and cognitive impairment in southeastern Spain: the Ariadna studyActa Neurol Scand2009120530030719832772
- García GarcíaFJSánchez AyalaMIAPMThe prevalence of dementia and its main subtypes in subjects older than 65 years: impact of occupation and education. The Toledo StudyMed Clin (Barc)200111611401407 Spanish http://www.ncbi.nlm.nih.gov/pubmed/1133368611333686
- FernándezMCastro-FloresJPerez-de Las HerasSMandaluniz-LekumberriAGordejuelaMZarranzJ[Prevalence of dementia in the elderly aged above 65 in a district in the Basque Country]Rev Neurol20084628996 Spanish18247280
- LoboALaunerLJFratiglioniLPrevalence of dementia and major subtypes in Europe: a collaborative study of population-based cohorts. Neurologic diseases in the Elderly Research GroupNeurology20005411 Suppl 5S4910854354
- PrinceMBryceRAlbaneseEWimoARibeiroWFerriCPThe global prevalence of dementia: a systematic review and metaanalysisAlzheimers Dement201391637523305823
- BacigalupoIMayerFLacorteEA systematic review and meta-analysis on the prevalence of dementia in Europe: estimates from the Highest-Quality studies adopting the DSM IV diagnostic criteriaJ Alzheimers Dis20186641471148130412486
- MatthewsFEArthurABarnesLEA two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: results of the cognitive function and Ageing Study I and IILancet201338299021405141223871492
- Gonçalves-PereiraMCardosoAVerdelhoAThe prevalence of dementia in a Portuguese community sample: a 10/66 dementia research Group studyBMC Geriatr201717126129115922
- KosmidisMHVlachosGSAnastasiouCADementia prevalence in Greece: The Hellenic Longitudinal Investigation of Aging and Diet (HELIAD)Alzheimer Dis Assoc Disord201832323223929528855
- RoehrSPabstALuckTRiedel-HellerSGIs dementia incidence declining in high-income countries? A systematic review and metaanalysisClin Epidemiol2018101233124730271219
- LangaKMLarsonEBCrimminsEMA comparison of the prevalence of dementia in the United States in 2000 and 2012JAMA Intern Med201717715127893041
- LoboASazPMarcosGPrevalence of dementia in a southern European population in two different time periods: the ZARADEMP projectActa Psychiatr Scand2007116429930717803760
- CraikFIBialystokEFreedmanMDelaying the onset of Alzheimer disease: bilingualism as a form of cognitive reserveNeurology201075191726172921060095
- PhungTKWaltoftBLKessingLVMortensenPBWaldemarGTime trend in diagnosing dementia in secondary careDement Geriatr Cogn Disord201029214615320150733
- Database - Eurostat Available from: http://ec.europa.eu/eurostat/data/databaseAccessed July 13, 2018
- Vilalta-FranchJGarre-OlmoJLópez-PousaS[Feasibility of a telemedicine support system for diagnosing dementia in primary care]Rev Neurol2012555263269 Spanish22930137
- RaitGWaltersKBottomleyCPetersenIIliffeSNazarethISurvival of people with clinical diagnosis of dementia in primary care: cohort studyBMJ2010341c358420688840
- SharpESGatzMRelationship between education and dementia: an updated systematic reviewAlzheimer Dis Assoc Disord201125428930421750453
- Gascón-BayarriJReñéRdel BarrioJLPrevalence of dementia subtypes in El Prat de Llobregat, Catalonia, Spain: the PRATICON studyNeuroepidemiology200728422423417878737