
Abstract
Purpose
Comparing rates of childhood infectious disease hospitalisations across countries may uncover areas for improvement in the prevention of severe childhood infections. We compared rates of childhood infectious disease hospital contacts across Denmark, Finland, Norway, and Sweden with the overall objective to elucidate potential differences in burden of disease and in organisational and registration practices.
Methods
Using national registries, we estimated incidence rates for infectious disease hospital contacts between 2008 and 2017 among children aged 0–14 years. We investigated the rates for different types of contacts (inpatient or outpatient including emergency room), duration of admission, and by sex.
Results
During the study period, the rate of all hospital contacts per 1000 person-years was highest in Sweden (125.2) followed by Finland (87.1), Denmark (79.0), and Norway (62.1). The rates aligned for inpatient contacts with overnight stays; 19.3 (Denmark), 16.6 (Finland), 16.3 (Norway), and 13.0 (Sweden); these were highest in early infancy in all countries. A peak around 1 year of age was seen in all countries except in Sweden. The rates were higher among boys compared with girls in early childhood, after 13 years of age the rates among girls surpassed the boys.
Conclusion
Large cross-country differences were observed for outpatient and short-term hospital contacts for infectious diseases, affected by differences in organisational structures and coding practices across and within countries over time. Inpatient contacts requiring overnight stays reflected more comparable levels of severe infections across countries. Childhood infectious disease morbidity was greatest among boys and before 2 years of age.
Introduction
Infectious diseases are common in childhood.Citation1,Citation2 Minimizing the burden of paediatric infectious diseases is of public health interestCitation3 with national preventive strategies, eg, vaccination programs in place to fulfil this aim.Citation4 In high-income countries, measures of hospital care utilisation for infections are often used to ascertain the burden of paediatric infectious diseases. Cross-country comparisons of burden of childhood infectious diseases are important to understand and inform health-care policy. However, differences in the organisation of health care, definitions of hospital contacts, and registration practices that can influence hospitalisation rates need to be considered when making cross-country comparisons.Citation5
The Nordic countries Denmark, Finland, Norway, and Sweden have many similarities, including the welfare state model promoting universal tax-funded healthcare for all.Citation5,Citation6 Previous Nordic studies describing paediatric hospitalisations for infections are limited to single country investigations,Citation1,Citation7–Citation16 and are often restricted to specific types of infections,Citation7–Citation11,Citation13,Citation14,Citation16 hampering cross country comparison.
In the present study, we aimed to compare the rates of childhood infectious disease hospital contacts by type of contact (all contacts or inpatients only) and duration of inpatient admission across the Nordic countries according to time, age, sex, and group of infection. Our overall objective was to investigate differences between countries and to elucidate whether differences might be related to differences in health-care organisations and registration practices or differences in burden of disease. We thus aim to identify metrics of infectious disease hospitalisations that may increase consistency in measures of infectious disease hospital contacts across countries and through comparison of these measures, identify potential areas for improvement in the handling and prevention of paediatric infections.
Materials and Methods
We conducted an observational study using nationwide register data from Denmark, Finland, Norway, and Sweden for infectious disease hospital contacts in children aged 0–14 years from 2008 to 2017. This age interval was chosen based on availability of data. Our primary aim was to compare the rates by type of contact and duration of admission over time and according to age. Secondary aims included comparisons by group of infection and sex.
Setting
The Nordic countries are characterized by the Nordic welfare state model.Citation6 In Denmark and Norway, all hospital care is free of charge.Citation17,Citation18 In Finland and some regions in Sweden, a small patient fee up to an annual maximum may be charged for inpatient contacts.Citation19,Citation20 A more detailed comparison of the Nordic countries and health-care systems is described elsewhere.Citation3
Data Sources
Individual-level information on hospital contacts, including type of contacts, diagnoses (international classification of disease version 10 (ICD-10)) and dates of admission and discharge, was obtained from the Danish National Patient Registry, Finnish Care Register for Health Care, Norwegian Patient registry, and the National Patient register in Sweden.Citation3 Date of birth and sex were obtained from the Civil Registration System in Denmark,Citation21 Statistics Norway (only year and month of birth), and Statistics Sweden.Citation22 In Finland, this information was obtained from the patient register.
Information on the underlying population at risk was obtained from publicly available population statistics.Citation23–Citation26
Defining Infectious Disease Hospitalisation Contacts
ICD-10 codes related to infections were selected based on an evaluation of codes used in previous studies (Appendix 1). The infectious disease codes were grouped as upper respiratory tract infections (URTI), lower respiratory tract infections (LRTI), gastrointestinal infections (GI), and other infections (OI), and further into subgroups (Appendix 1).
We identified infectious disease hospital contacts (including inpatient, outpatient, and emergency room contacts) and included both primary and secondary diagnoses, as coding practices may differ across countries and time. Infectious disease hospital contacts occurring within 14 days after discharge from a previous infectious disease hospital contact were regarded as the same infectious disease episode and counted as a single hospital contact.
We defined four different types of contacts: 1) all hospital contacts (inpatient, outpatient, emergency room); 2) all inpatient hospital contacts (including those with no overnight stays); 3) inpatient hospital contacts with overnight stays; 4) inpatient hospital contacts lasting at least two nights.
Statistical Analyses
We estimated the incidence rate (IR) as the number of infectious disease hospital contacts per 1000 children in the population, corresponding to approximately 1000 person-years (PY). Since common infectious diseases are linked to seasonal incidence patterns,Citation2 we defined an epidemiological year as running from July 1 to June 30 the following year. Our study period was July 1, 2008 to June 30, 2017.
We estimated age-standardized rates among all children aged 0–14 years according to epidemiological year using the average population of each 1-year age group across countries and epidemiological years as the standard. Rates according to epidemiological years were calculated for each type of contact and by group of infection.
We also estimated the age-specific rates in 1-month intervals among children aged 0–35 months and 1-year intervals among children aged 3–14 years for each type of contact. For inpatient contacts with overnight stays, we further estimated the age-specific rates according to group of infection and sex.
To assess potential differences in coding practices, we calculated the frequency (%) of the most common subgroups of infection registered within each main group of infection (Appendix 1). Most GI infections cannot be discerned based on symptoms only. Thus, we grouped all GI together, which precluded an analysis by subgroup of infections.
We used Stata version 16.0 (StataCorp, College Station, Texas, USA) to conduct the analyses and R version 3.3.3 to visualize data.
Ethics
Ethical approval is not required for registry-based studies in Denmark and Finland. However, the study was approved by the Danish Data Protection Agency and by the Institutional Review Board of the Finnish Institute for Health and Welfare. In Norway, study approval was obtained from the Regional Ethics Committee, South-East. In Sweden, study approval was obtained from the Regional Ethical Review Board, Stockholm, Sweden.
Results
Rates Across Time by Type of Contact
The age-standardized incidence rates of all infectious disease hospital contacts (including inpatient, outpatient, and emergency room contacts) for children aged 0–14 years in the study period varied across countries: the rates per 1000 PY ranged from 62.1 in Norway to 125.2 in Sweden (sTable 1). The rates were higher in Sweden compared with the other countries in all epidemiological years (, panel 1). Until year 2012/13 the rates were also higher in Finland compared with Denmark and Norway, whereafter a steep increase was observed in Denmark from 62.5 in 2012/2013 to 107.5 in 2014/2015. The Finnish rates increased from 73.4 in 2013/2014 to 102.5 in 2015/16.
Figure 1 Age-standardized incidence rate (per 1000 person-years) of infectious disease episodesa with hospital contacts among children aged 0–14 years by epidemiological year (2008/2009‒2016/2017), country and type of hospital contact. aHospital contacts with infections, which occur less than 14 days after discharge/visit date of a previous contact with infection are defined as the same infectious disease episode.
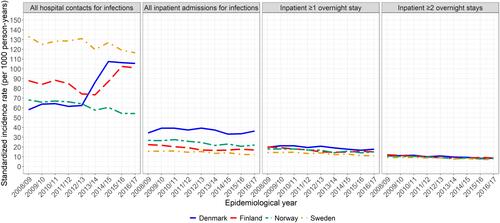
Including only inpatient contacts resulted in lower and more comparable rates across the four countries: the IR across the study period ranged from 14.3 in Sweden to 36.7/1000 PY in Denmark (sTable 1). The rates were stable with a minor decreasing trend across the epidemiological years with consistently higher rates in Denmark (, panel 2). Cross-country differences diminished with longer duration of admission (, panel 3+4 and sTable 1).
Rates by Age
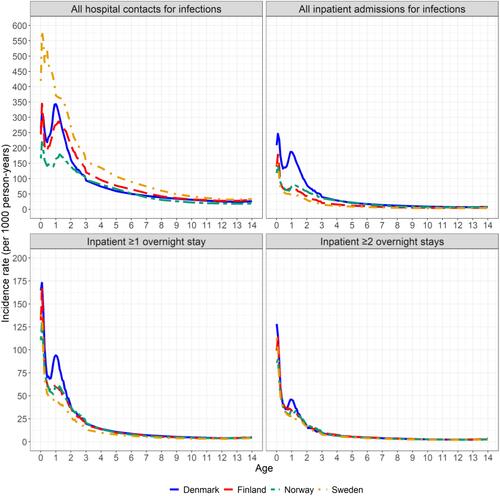
The rates including all hospital contacts were highest in the first two years of life in all countries (, top left panel and sTable 2). The rates were highest in Sweden at all ages. Including only inpatient contacts, the rates were highest in the first year of life with peak incidence before 3 months of age in all countries followed by a smaller peak around 1 year of age in Denmark, Norway, and Finland ( and sTable2). The rates were higher in Denmark across all age groups, but cross-country differences gradually decreased with longer duration of admission and older age of the children.
Figure 2 Incidence rate (per 1000 person-years) of infectious disease hospital episodesa for epidemiological years 2008/2009‒2016/2017, by age, country, and type of hospital contact. aHospital contacts with infections, which occur less than 14 days after discharge/visit date of a previous contact with infection are defined as the same infectious disease episode.
Rates by Group of Infection
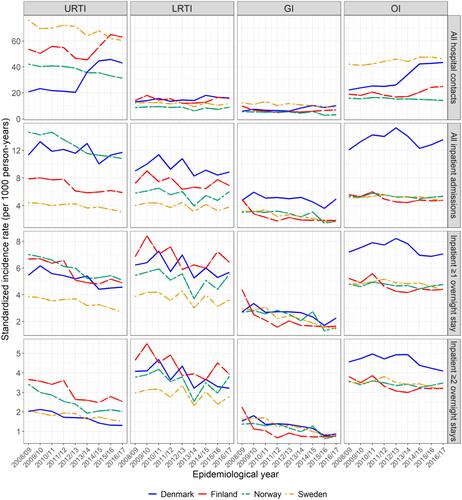
Including all contacts, higher rates of URTI were observed in Sweden and Finland across all epidemiological years (, first row). Sweden experienced the highest rates of OI across the study period. From year 2012/13 in Denmark and 2013/14 in Finland, the rate of URTI and OI increased. Looking only at inpatient contacts, Denmark and Norway had the highest rates of URTI, followed by Finland and Sweden, whereas Denmark had higher rates of LRTI, GI and OI than the other countries (, second row). For inpatient contacts with overnight stays, the rates were relatively similar across countries (, third row). A general downward-going trend was observed for URTI in all countries. However, higher rates of GI in 2008/09 in Finland and OI across all years in Denmark were observed. The rates of URTI and LRTI were lower in Sweden than in the other countries across the study period. Similar patterns were observed for inpatient hospital contacts lasting at least two nights, but with smaller differences between the countries (, fourth row).
Figure 3 Age-standardized incidence rate (per 1000 person-years) of infectious disease hospital contactsa among children aged 0–14 years by group of infectionb, epidemiological year (2008/2009‒2016/2017), country and type of hospital contact. aHospital contacts with infections, which occur less than 14 days after discharge/visit date of a previous contact with infection are defined as the same infectious disease episode. bDifferent types of infections within an infectious disease hospital episode are counted, thus summing the rates over types of infections will give greater rate, than the rates presented in .
Age-Specific Rates of Inpatient Hospital Contacts with Overnight Stays by Group of Infection and Sex
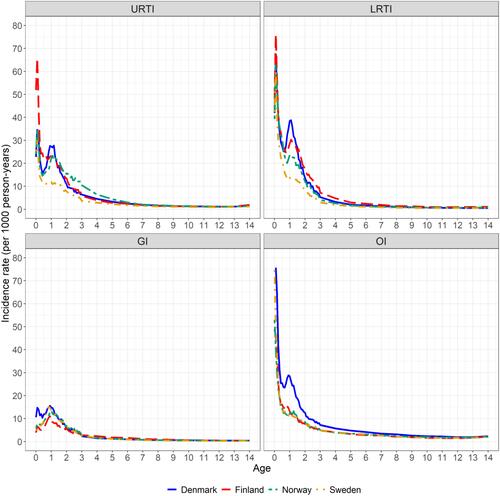
In all countries, LRTI and OI were the most frequently registered infections within inpatient contacts with overnight stays in early infancy (before 3 months of age) followed by admissions with URTI (). A second peak was registered around 1 year of age for LRTI and URTI in Denmark, Finland, and Norway, with the highest rates in Denmark. The Swedish rates levelled off at this age and at lower rates compared with the other countries.
Figure 4 Incidence rate (per 1000 person-years) of inpatient contacts with minimum 1 overnight stay for epidemiological years 2008/2009‒2016/2017 by group of infectiona, age, and country. aDifferent types of infections within an infectious disease hospital episode are all counted toward that type of infections (eg if both ICD-10 codes for GI and LRTI is registered during an infectious disease hospital episode the contact is counted both as GI and LRTI), thus summing the rates over types of infections will give greater rates, than the rates presented in .
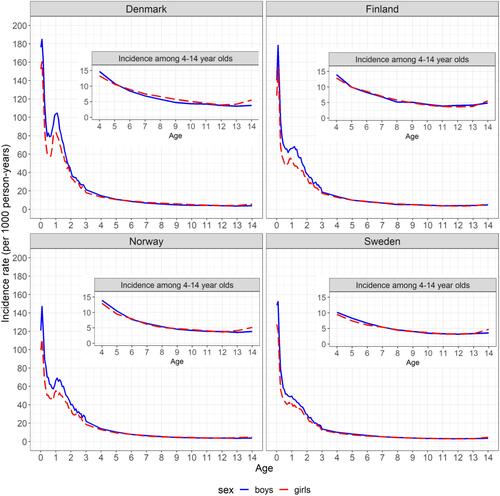
In all countries, the rates of inpatient hospital contacts with overnight stays were higher among boys compared with girls until 5–7 years of age (). Thereafter, the rates were similar until 13 years of age when the rates for girls surpassed that of boys.
Figure 5 Incidence rate (per 1000 person-years) of infectious disease inpatient hospital episodesa with minimum 1 overnight stay for epidemiological years 2008/2009‒2016/2017 by age, sex, and country. aHospital contacts with infections, which occur less than 14 days after discharge/visit date of a previous contact with infection are defined as the same infectious disease episode.
Analysis of Subgroups of Infections
The proportion of registrations of specific subgroups of infections within each group of infections during inpatient hospitalisations with at least one overnight stay varied across countries (), eg, pneumonia diagnoses ranged from 32% to 33% in Finland and Norway to 52% in Denmark, and pyelonephritis ranged from 13% to 14% in Denmark, Norway, and Sweden to 23% in Finland.
Table 1 Distribution of the Most Common Subgroups of Infections for Inpatient Hospital Episodes with at Least One Overnight Stay, by Group of Infection and Country
Discussion
We observed large differences in the rates of infectious disease hospital contacts both across the Nordic countries and within countries over time when including both inpatient, outpatient, and emergency room contacts. The rates gradually aligned as we restricted the analyses to inpatient contacts and longer duration of admission. The rates of inpatient contacts with overnight stays were highest in early infancy in all countries, mostly driven by LRTI and OI. The rates of inpatient contacts with overnight stays were higher among boys compared with girls until about 5 years of age, whereas they were higher among girls compared with boys after the age of 13 years.
Strengths and Limitations
In the Nordic countries, reporting to the patient registries is mandatory. The registries contain both inpatient, outpatient, and emergency room contacts and diagnoses are coded according to ICD-10 in all countries.Citation3,Citation5 This facilitated the cross-country comparison in the present study.
Including both primary and secondary diagnoses increased the likelihood of capturing all infectious disease contactsCitation27 regardless of coding practices over time and across countries. However, it also entailed a risk of including infections from admissions with non-infectious primary causes and thus overestimating the rates.
Due to a lack of documentation and registration, it was not clear which services that constitute an outpatient contact. As such, it was not possible to separate, eg, phone consultations from in-person outpatient contacts, nor was it clear to which extent such contacts contributed to the registered rates. This may in part explain the cross-country differences in outpatient contacts seen in this study.
Furthermore, outpatient contacts cannot be separated from emergency room contacts in Sweden, thus limiting the possibility to examine these two types of contacts separately. Furthermore, we did not include information from primary care. Therefore, it was not possible from this study to identify the overall burden of infectious diseases leading to medical contacts.
Differences in Organisation and Access to Care
Sweden followed by Finland had higher rates of all types of hospital contacts for infections than Denmark and Norway, dominated by higher rates of URTI. All specialized outpatient clinics operated by doctors report to the patient registries in Sweden. In Finland, also day-surgery at private ear-, nose-, and throat-clinics is registered at the patient register. These may explain the higher rates of URTI. Reporting from specialized outpatient clinics outside hospital settings is incomplete in Norway and thus not included in the data for the present study, and only services from public hospitals are included in the Danish Patient Registry.
In Sweden, paediatric outpatient clinics, which manage common and mild conditions in early childhoodCitation28,Citation29 further contribute to the observed higher rates, including higher rates of OI. In the other countries, such conditions are usually handled in primary care and thereby not included in the patient registries.
The steep increase in rates, including all contacts in Denmark around year 2014 coincides with the introduction of a new out-of-hours primary care medical service organised within the emergency room department in the capital region of Denmark.Citation30 This organisational change resulted in registration of contacts in the patient registry, which previously would have been recorded in primary care. Similar organisational changes in emergency care and registration in the patient registry were developed from 2009 in FinlandCitation31 and further implemented during 2013 and 2014,Citation32 which coincides with the increase in the Finnish rates in 2013/14. Different rates of infectious hospital contacts that include outpatient and emergency room contacts are thus unlikely to reflect different levels of infectious disease morbidity but are instead heavily affected by different organisation of care and coding practices within and across countries. This points to the potential for reducing hospital contacts and cost of care, to the extent that children are allocated to specialist care with diseases that could have been dealt with in general practice.
Across the study period, Denmark had notably higher rates of inpatient contacts including contacts without overnight stays, mainly for the youngest children, compared with the other countries. Norway also experienced slightly higher rates compared with Finland and Sweden. The difference was dominated by higher rates of URTI and OI and may be an artefact of different registration practices given that admissions without overnight stays are commonly registered as outpatient contacts in Finland and Sweden.
Inpatient Contacts with Overnight Stays
The greater similarity between countries in rates of inpatient hospital contacts with overnight stays likely reflects that more severe infections requiring hospitalisation overnight are less likely to be influenced by health-care organisation and coding practices. In all countries, the highest rates were observed among young infants (up to three months of age). This may be a result of neonatal complications and hospitalisation of children born preterm with a higher risk of infectionsCitation33 but may also reflect secondary diagnoses among otherwise healthy new-borns (ie, eye infections)Citation1 as well as low thresholds for admitting the youngest children with otherwise uncomplicated infections overnight.
Despite the similarity, the rates remained higher in Denmark across all epidemiological years, dominated by higher rates of OI and LRTI among 1-year-olds. It is not possible, based on the available data, to determine whether these excess hospitalisations are due to increased burden of disease or lower threshold for admitting young children for infectious diseases in Denmark. Finland and Norway also experienced higher rates among 1-year-olds compared with Sweden, which coincides with the common age for entry into day care. The lower rates across epidemiological years in Sweden were explained by lower rates of LRTI and URTI among 1-year-olds. Swedish parents may extend their parental leave up to 68 weeks after birth,Citation34 which might explain the lower incidence in Sweden.
Patient fees may affect health care seeking behaviour and thus influence the rates of infectious disease hospitalization. Reassuringly, the rates in Finland, where patients must pay a minor fee for inpatient care, were similar to the rates in Norway, where no fee is charged. Thus, this study does not provide indication that low-level patient fees withhold parents from seeking care for their children for infections leading to hospitalisation.
Sex Differences
The age-specific patterns of sex differences were similar across countries, indicating sex-differential susceptibility to infections requiring hospitalisation according to age. Sex differences in infectious diseases are well established, but not fully understood.Citation35 Girls have been found to mount stronger immunological responses which may reduce susceptibility towards some infections and explain the lower rates in this study.Citation35 In addition, sex hormones affect the immune system differently at different ages,Citation35 which has been proposed to contribute to the divergent sex differences in infections according to age.Citation1 This aligns with our observation that boys had higher rates of inpatient contacts with overnight stays until approximately 5 years of age and lower rates after 13 years of age compared with girls.
Rates by Group of Infections and Correlation with Health Interventions
The rates of GI dropped in Finland from 2009, and in Norway from 2014 which coincides with the national introduction of rotavirus vaccinationCitation36,Citation37 (sFigure 1). However, the incidence of inpatient contacts with overnight stays for GI also decreased across years in Denmark, where rotavirus vaccination was not offered, and in Sweden, where rotavirus vaccine was only implemented in some regions in 2014.Citation38 The rates of URTI decreased over time in all countries, which may partly be attributable to reductions in otitis media following introduction of pneumococcal conjugate vaccines in all countriesCitation39,Citation40 (sFigure 1). All vaccines within the national immunisation programmes are administered free of charge. Furthermore, the proportion of adult smokers has also decreased across the study period in all countries,Citation41 which may contribute to the downward going trend for respiratory tract infections as a result of decreased passive smoking exposure.Citation42
The proportions of specific subgroups of infections varied greatly across the countries, which is unlikely to be explained solely by differences in burden of disease. Instead, reporting of specific subgroups of infections depends on the diagnostic accuracy for that infection and registration practices. A previous Danish validation study found that the positive predictive value was 72% for all medical contacts when identification was made on a 5-digit ICD-10 level, but increased to 81% on the 3-digit-level.Citation27 These previous findings coincide with the findings from the present study, as the combined rates by the broader groups of infections (LRTI, URTI, GI, and OI) were similar across countries, while the distribution of the more specific subgroups differed.
Comparison to Other Studies
Few studies have reported on the overall rates of childhood infectious disease hospitalisations. In the United States, the incidence of infectious inpatient hospitalisations was estimated at 70.1/1000 children below 1 year of age in 2003,Citation2 which is considerably lower than in Denmark, but comparable to the other Nordic countries. Many paediatric infections are first cared for in emergency room departments in the United States, whereof only 5% resulted in hospitalisation.Citation43
Conclusion
Differences across countries and over time to a large extent reflect differences in health-care organisation and registration practices for outpatient contacts and inpatient contacts without overnight stays. When focusing on the comparable outcome, rates of inpatient contacts with overnight stays, we found that these differed similarly across countries with regard to age and sex of the child, with the anticipated highest rates in the youngest males. Some of the between-country and within-country differences observed coincide with introduction of vaccines, decreased prevalence of smoking, and entrance into day-care and point towards areas for improvement of prevention of childhood infectious disease.
Register data offer an excellent opportunity to study large, comprehensive, and representative cohorts under routine care for long periods of time with relatively low resources. The present study displays that valid cross-country comparison is enhanced with increasing duration of admission as a measure of infectious disease severity. Meanwhile, differences in diagnostic accuracy and reimbursement incentives may hamper cross-country comparison for some subgroups of infections.
Data Sharing Statement
Data on hospital contacts used in this study arises from nationwide registers. Due to data protection rules, we are not allowed to share the individual-level data, but other researchers fulfilling the requirements from the data providers could obtain similar data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
AAP and HN are investigators in vaccine-related studies for which THL has received funding from GSK, Pfizer and Sanofi Pasteur. Dr Signe Sørup reports grants from NordForsk, during the conduct of the study. The remaining authors report no relation that could be construed as a conflict of interest.
Additional information
Funding
References
- Larsen JWW, Sørensen AF, Jensen AKG, et al. Hospitalizations for infections by age and sex: register-based study of Danish children 1977–2014. Infect Dis. 2020;52(2):97–106. doi:10.1080/23744235.2019.1682657
- Yorita KL, Holman RC, Sejvar JJ, et al. Infectious disease hospitalizations among infants in the United States. Pediatrics. 2008;121(2):2442–2452. doi:10.1542/peds.2007-1392
- Laugesen K, Ludvigsson JF, Schmidt M, et al. Nordic health registry-based research: a review of health care systems and key registries. Clin Epidemiol. 2021;13:533–554. doi:10.2147/CLEP.S314959
- World Health Organization. Vaccines and immunization: what is vaccination?; 2021. Available from: https://www.who.int/news-room/q-a-detail/vaccines-and-immunization-what-is-vaccination?adgroupsurvey={adgroupsurvey}&gclid=EAIaIQobChMI_suNmaaP8wIVhdV3Ch1clgXVEAAYASAAEgIH_vD_BwE. Accessed April 16, 2022.
- Maret-Ouda J, Tao W, Wahlin K, et al. Nordic registry-based cohort studies: possibilities and pitfalls when combining Nordic registry data. Scand J Public Health. 2017;45(17_suppl):14–19. doi:10.1177/1403494817702336
- Greve B, Kvist J. What characterise the Nordic welfare state model. J Soc Sci. 2007;3(2):43–51. doi:10.3844/jssp.2007.43.51
- Berglund A, Ekelund M, Fletcher MA, et al. All-cause pneumonia hospitalizations in children <2 years old in Sweden, 1998 to 2012: impact of pneumococcal conjugate vaccine introduction. PLoS One. 2014;9(11):e112211. doi:10.1371/journal.pone.0112211
- Bruun T, Salamanca BV, Bekkevold T, et al. Burden of rotavirus disease in Norway: using National Registries for Public Health Research. Pediatr Infect Dis J. 2016;35(4):396–400. doi:10.1097/INF.0000000000001055
- Fischer TK. Incidence of hospitalizations due to rotavirus gastroenteritis in Denmark. Acta Paediatr. 2001;90(9):1073–1075. doi:10.1111/j.1651-2227.2001.tb01366.x
- Flem E, Vainio K, Døllner H, et al. Rotavirus gastroenteritis in Norway: analysis of prospective surveillance and hospital registry data. Scand J Infect Dis. 2009;41(10):753–759. doi:10.1080/00365540903161515
- Haataja P, Korhonen P, Ojala R, et al. Hospital admissions for lower respiratory tract infections in children born moderately/late preterm. Pediatr Pulmonol. 2018;53(2):209–217. doi:10.1002/ppul.23908
- Kamper-Jorgensen M, Wohlfahrt J, Simonsen J, et al. Temporal trend in paediatric infections in Denmark. Arch Dis Child. 2006;91(5):401–404. doi:10.1136/adc.2005.085787
- Munson S, Raluy-Callado M, Lambrelli D, et al. Clinical burden of pneumonia, meningitis and septicemia in Norway 2 years after 7-valent pneumococcal conjugate vaccine introduction. Scand J Public Health. 2015;43(6):657–666. doi:10.1177/1403494815581695
- Senstad AC, Surén P, Brauteset L, et al. Community-acquired pneumonia (CAP) in children in Oslo, Norway. Acta Paediatr. 2008;98(2):332–336. doi:10.1111/j.1651-2227.2008.01088.x
- Stordal K, Lundeby KM, Brantsæter AL, et al. Breast-feeding and infant hospitalization for infections: large cohort and sibling analysis. J Pediatr Gastroenterol Nutr. 2017;65(2):225–231. doi:10.1097/MPG.0000000000001539
- Svensson C, Berg K, Sigurs N, et al. Incidence, risk factors and hospital burden in children under five years of age hospitalised with respiratory syncytial virus infections. Acta Paediatr. 2015;104(9):922–926. doi:10.1111/apa.13061
- Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
- Saunes IS, Karanikolos M, Sagan A. Norway: health system review. Health Syst Transit. 2020;22(1):1–163.
- KELA. Treatment costs in public health care; 2020 [cited March 10, 2022]. Available from: https://www.eu-healthcare.fi/what-you-pay/costs-of-treatment-in-finland/treatment-costs-in-public-health-care/. Accessed April 16, 2022.
- Knutson H. Patientavgifter och högkostnadsskydd; 2020 [cited August 3, 2020]. Available from: https://www.1177.se/sa-fungerar-varden/kostnader-och-ersattningar/patientavgifter/. Accessed April 16, 2022.
- Schmidt M, Pedersen L, Sorensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
- Ludvigsson JF, Almqvist C, Bonamy A-KE, et al. Registers of the Swedish total population and their use in medical research. Eur J Epidemiol. 2016;31(2):125–136. doi:10.1007/s10654-016-0117-y
- Statistics Denmark. Available from: http://www.statistikbanken.dk/10021. Accessed April 16, 2022.
- Statistics Finland. Available from: http://pxnet2.stat.fi/PXWeb/pxweb/en/StatFin/StatFin__vrm__vaerak/statfin_vaerak_pxt_004.px/?rxid=71b6be23. Accessed April 16, 2022.
- Statistics Norway. Available from: https://www.ssb.no/en/statbank/table/07459/. Accessed April 16, 2022.
- Statistics Sweden. Available from: http://www.statistikdatabasen.scb.se/pxweb/en/ssd/START__BE__BE0101__BE0101A/BefolkningNy/?rxid=f5bf3beb. Accessed April 16, 2022.
- Schmidt M, Schmidt SAJ, Sandegaard JL, et al. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
- Schöldéen Å. Barn- och ungdomsmedicinska mottagningar (BUMM); 2019 [cited March 17, 2020]; Available from: https://www.1177.se/Stockholm/sa-fungerar-varden/varden-i-stockholms-lan/hjalp-att-valja-mottagning/barn–och-ungdomsmedicinska-mottagningar-bumm/. Accessed April 16, 2022.
- Socialstyrelsen. Oppen-specialiserad-vard-2019-patientregistret; 2019. Available from: https://www.socialstyrelsen.se/utveckla-verksamhet/e-halsa/klassificering-och-koder/andra-kodverk/sjukhuskoder/. Accessed April 16, 2022.
- Gubbels S, Nielsen KS, Sandegaard J, et al. The development and use of a new methodology to reconstruct courses of admission and ambulatory care based on the Danish National Patient Registry. Int J Med Inform. 2016;95:49–59. doi:10.1016/j.ijmedinf.2016.08.003
- Artama M, Rinta-Kokko H, Nohynek H, et al. Register-based ecologic evaluation of safety signals related to pneumococcal conjugate vaccine in children. Curr Drug Saf. 2018;13(2):107–112. doi:10.2174/1574886313666180406164151
- Huovinen S, Koskela A. Decree of the Ministry of Social Affairs and Health on the grounds of urgent care and the conditions for on-call care in different medical areas of activity, Ministry of Social Affairs and Health, Editor; 2014. Available from: https://www.finlex.fi/sv/laki/alkup/2014/20140782. Accessed April 16, 2022.
- Collins A, Weitkamp JH, Wynn JL. Why are preterm newborns at increased risk of infection? Arch Dis Child Fetal Neonatal Ed. 2018;103(4):F391–f394. doi:10.1136/archdischild-2017-313595
- Gíslason IV, Eydal GB. Parental Leave, Childcare and Gender Equality in the Nordic Countries. Nordic Council of Ministers; 2011.
- Muenchhoff M, Goulder PJ. Sex differences in pediatric infectious diseases. J Infect Dis. 2014;209 Suppl 3(Suppl 3):S120–6. doi:10.1093/infdis/jiu232
- Leino T, Baum U, Scott P, et al. Impact of five years of rotavirus vaccination in Finland – and the associated cost savings in secondary healthcare. Vaccine. 2017;35(42):5611–5617. doi:10.1016/j.vaccine.2017.08.052
- Bruun T, Salamanca BV, Bekkevold T, et al. Impact of the rotavirus vaccination program in Norway after four years with high coverage. Pediatr Infect Dis J. 2021;40(4):368–374. doi:10.1097/INF.0000000000003020
- Oldin C, Golsäter M, Schollin Ask L, et al. Introduction of rotavirus vaccination in a Swedish region: assessing parental decision-making, obtained vaccination coverage and resulting hospital admissions. Acta Paediatr. 2019;108(7):1329–1337. doi:10.1111/apa.14674
- Dagan R, Van Der Beek BA, Ben-Shimol S, et al. Effectiveness of the seven- and thirteen valent pneumococcal conjugate vaccines against vaccine-serotype otitis media. Clin Infect Dis. 2021;73:650–658. doi:10.1093/cid/ciab066
- Palmu AA, Rinta-Kokko H, Nohynek H, et al. Impact of national ten-valent pneumococcal conjugate vaccine program on reducing antimicrobial use and tympanostomy tube placements in Finland. Pediatr Infect Dis J. 2018;37(1):97–102. doi:10.1097/INF.0000000000001810
- OECD. Stat non-medical determinants of health: tobacco consumption; 2021. Available from: https://stats.oecd.org/index.aspx?queryid=30127. Accessed April 16, 2022.
- Huttunen R, Heikkinen T, Syrjänen J. Smoking and the outcome of infection. J Intern Med. 2011;269(3):258–269. doi:10.1111/j.1365-2796.2010.02332.x
- Hasegawa K, Tsugawa Y, Cohen A, et al. Infectious disease-related emergency department visits among children in the US. Pediatr Infect Dis J. 2015;34(7):681–685. doi:10.1097/INF.0000000000000704