
Abstract
Patients with metastatic colorectal cancer (mCRC) are surviving longer now than ever before, but mortality rates are still high and more effective therapies are clearly needed. For patients with disease that is refractory to fluoropyrimidines, oxaliplatin, irinotecan, and biologic agents targeting the vascular endothelial growth factor and epidermal growth factor receptor pathways, novel treatment options trifluridine/tipiracil (TAS-102) and regorafenib can be effective disease stabilizers. However, objective clinical responses are rare and toxicities are manageable but common. In order to tackle poor clinical responses to TAS-102, there is an ongoing effort to effectively combine this drug with other agents, particularly those targeting angiogenesis. Certain subpopulations appear to benefit more than others from TAS-102; those that benefit often have underlying genetic defects in DNA repair pathways and/or develop neutropenia. In this review, we focus on the role of TAS-102 in the treatment of mCRC, including its use in combination with other agents, potential predictive biomarkers of response to TAS-102, and possible future directions.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
In 2017, it is estimated that there will be 135,430 new cases of colorectal cancer (CRC) and 50,260 deaths resulting from this disease, making it the second leading cause of cancer mortality in the USA.Citation1 At diagnosis, about 21% of patients have metastatic disease, and these individuals have a 5-year survival rate of only 13.9%.Citation2 Due to advances in chemotherapy for patients with metastatic colorectal cancer (mCRC), median overall survival (mOS) has increased to ≥30 months, compared with <12 months in the era of treatment with single-agent fluoropyrimidines.Citation3–Citation5
First-line chemotherapeutic options for mCRC involve fluoropyrimidines, such as 5-fluorouracil (5-FU) or capecitabine, combined with oxaliplatin and/or irinotecan. Standard treatment regimens include FOLFOX (leucovorin/5-FU/oxaliplatin), CAPOX (capecitabine/oxaliplatin), FOLFIRI (leucovorin/5-FU/irinotecan), and FOLFOXIRI (leucovorin/5-FU/oxaliplatin/irinotecan).Citation3,Citation6–Citation9 The advent of monoclonal antibodies (mAbs) bevacizumab (Avastin®; Genentech, South San Francisco, CA, USA),Citation9 an anti-vascular endothelial growth factor A (VEGF-A) antibody, and cetuximab (Erbitux; Eli Lilly and Company, Indianapolis, IN, USA),Citation10 an anti-epidermal growth factor receptor (EGFR) antibody, given in combination with fluoropyrimidine/oxaliplatin/irinotecan regimens, gave rise to the most promising treatment options available in the first line. EGFR targeting agents are restricted to patients with RAS wild-type tumors.Citation11,Citation12 When first-line therapies fail, patients are often treated with yet unused cytotoxic therapies combined with continued bevacizumab therapy,Citation13,Citation14 the anti-EGFR antibody, panitumumab (Vectibix®; Amgen, Thousand Oaks, CA, USA),Citation15 or other antiangiogenic agents including ziv-aflibercept (Zaltrap®; Sanofi/Regeneron, Tarrytown, NY, USA) and ramucirumab (Cyramza®; Eli Lilly and Company).Citation16,Citation17 Pembrolizumab, an anti-programmed death 1 (PD1) mAb immune checkpoint inhibitor, is now Food and Drug Administration (FDA) approved for microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) mCRC following treatment with fluoropyrimidine, oxaliplatin, and irinotecan regimens.Citation18–Citation20 Previously, patients who progressed on standard chemotherapy and biologics were often left to rely on best supportive care (BSC) or participate in a clinical trial. However, now there are new and approved treatment options available with proven efficacy and tolerability in patients with refractory mCRC.
One such treatment is trifluridine/tipiracil (TAS-102, Lonsurf®; Taiho Oncology, Princeton, NJ, USA), which contains the oral cytotoxic agent trifluridine that was developed more than half a century ago. In this review, we discuss the pharmacology and clinical data of TAS-102; compare TAS-102 with regorafenib (Stivarga®, Bayer AG, Leverkusen, Germany), an alternative treatment option for patients with refractory mCRC; and discuss other therapies used in combination with TAS-102. Additionally, we consider potential biomarkers that could predict response to therapy with TAS-102 and examine clinical trials of TAS-102 in patients with refractory mCRC.
Pharmacology
TAS-102, which consists of trifluridine and tipiracil in a 1:0.5 molar ratio, was approved by the FDA for the treatment of refractory mCRC in September 2015.Citation21 Trifluridine (5-trifluoro-2′-deoxythymidine) was developed by Heidelberger et al in 1964 as an alternative to 5-FU.Citation22 It is a thymidine analog that inhibits cell growth by affecting DNA synthesis (). Thymidine kinase (TK) phosphorylates trifluridine to its monophosphate form, trifluridine monophosphate (TF-TMP), which then inhibits thymidylate synthase (TS) and prevents methylation of 2′-deoxyuridine-5′-monophosphate (dUMP) to 2′-deoxythymidine-5′-monophosphate.Citation23–Citation26 dUMP is then alternatively phosphorylated to its triphosphate form, 2′-deoxyuridine-5′-triphosphate, which causes the incorporation of uracil into DNA, inhibiting DNA synthesis and leading to cell death.Citation27,Citation28 Additionally, in a separate pathway, TF-TMP is further phosphorylated to trifluridine triphosphate (TF-TTP), which causes cell death via direct incorporation into DNA.Citation29,Citation30 Despite the evident clinical activity of trifluridine in patients with CRC and breast cancer, its short half-life (12–18 minutes) and significant myelosuppression were found to limit its clinical utility.Citation31
Figure 1 Mechanism of action of TAS-102.
Abbreviations: TP, thymidine phosphorylase; FTY, 5-trifluoromethyl-2,4(1H,3H)-pyrimidinedione; hENT, human equilibrative nucleoside transporter; TK, thymidine kinase; TF-TMP, trifluorothymidine monophosphate; TF-TDP, trifluorothymidine diphosphate; TF-TTP, trifluorothymidine triphosphate; TS, thymidylate synthase; dTMP, 2′-deoxythymidine-5′-monophosphate; dTTP, 2′-deoxythymidine-5′-triphosphate; dUMP, 2′-deoxyuridine-5′-monophosphate; dUTP, 2′-deoxyuridine-5′-triphosphate.
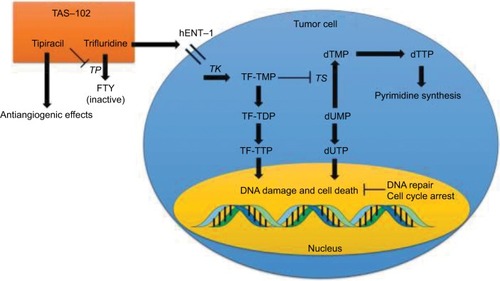
In the 1990s, it was discovered that the combination of tipiracil (5-chloro-6-[(2-iminopyrrolidin-1-yl)methyl]-1H-pyrimidine-2,4-dione) with trifluridine increased the bioavailability of trifluridine by inhibiting thymidine phosphorylase (TP), the enzyme that converts trifluridine into inactive 5-trifluoromethyl-2,4(1H,3H)-pyrimidinedione.Citation32 Inhibition of TP, a known platelet-derived endothelial cell growth factor, also has indirect antiangiogenic benefits.Citation33–Citation35 TAS-102 was effective in 5-FU-resistant CRC cell lines, due to direct TF-TTP incorporation into DNA and the resistance of trifluridine to degradation by DNA glycosylase, suggesting efficacy in 5-FU-refractory mCRC.Citation32,Citation36–Citation38
Clinical trials of TAS-102
Hong et al published the initial Phase I trial of TAS-102 in 14 patients with refractory mCRC ().Citation39 The maximally tolerated dose (MTD) was 50 mg/m2/day administered once daily on days 1–14 of a 21-day cycle (grade 3–4 granulocytopenia was the dose limiting toxicity [DLT] in 3 of 6 patients treated at the 60 mg/m2/day dose level). Of the 12 patients evaluable for response, the best response was in 4 patients with stable disease. Another Phase I study reported by Overman et al examined 2 TAS-102 dosing schedules.Citation40 In the 63 patients studied (52 with refractory mCRC), the recommended Phase II doses (RP2Ds) were 100 mg/m2/day administered once daily on days 1–5 and 8–12 of a 28-day cycle or 160 mg/m2/day once daily on days 1–5 of a 21-day cycle. Granulocytopenia was again the DLT in most cases. Thirty percent of patients had stable disease, but no objective clinical responses were seen.
Table 1 Completed TAS-102 trials in mCRC
Doi et al conducted another Phase I study using twice daily dosing in 21 Japanese patients (18 with refractory mCRC).Citation41 In this trial, the RP2D was 70 mg/m2/day split into 2 daily doses on days 1–5 and 8–12 of a 28-day cycle (the DLT again was grade 4 neutropenia). No objective responses were observed in patients with mCRC, but 50% had stable disease. Median progression-free survival (mPFS) was 2.4 months and mOS was 9.8 months. Three times daily dosing was also studied in a separate Phase I trial of 15 patients with advanced solid tumors. On a schedule of TAS-102 split into 3 daily doses on days 1–5 and 8–12 of a 28-day cycle, the MTD was 80 mg/m2/day and the DLT was granulocytopenia. Nine patients had prolonged stable disease.Citation42 Finally, Bendell et al conducted a Phase I study involving TAS-102 treatment of 27 US patients with refractory mCRC. The RP2D in this study was 70 mg/m2/day, split into 2 daily doses, administered on days 1–5 and 8–12 of a 28-day cycle, at which dose 70% of evaluable patients had stable disease lasting at least 6 weeks, and mPFS and mOS of the entire population were 5.3 and 7.5 months, respectively.Citation43
In the J003 Phase II trial published by Yoshino et al, 169 Japanese patients with refractory mCRC were randomized 2:1 to 35 mg/m2 TAS-102 or placebo, both administered twice daily on days 1–5 and 8–12 of a 28-day cycle.Citation44 The primary endpoint of the study was mOS, which was significantly longer in the TAS-102 group compared to placebo: 9.0 versus 6.6 months (hazard ratio [HR] for death 0.56, 80% confidence interval [CI] 0.44–0.71; P=0.0011). mPFS was also significantly longer in the TAS-102 group: 2.0 versus 1.0 month (HR 0.41, 95% CI 0.28–0.59; P<0.0001). In the subgroup analysis, patients with KRAS exon 2 mutated tumors were found to have a greater overall survival (OS) benefit (13.0 vs 6.9 months with placebo, P=0.0056) than patients with KRAS exon 2 wild-type tumors (7.2 vs 7.0 months, P=0.191). Regarding adverse events, patients who received TAS-102 had significantly more hematological adverse events (including 50% with grade 3–4 neutropenia), as well as diarrhea, nausea, and anorexia than those receiving placebo.
These early phase trials led to the randomized, double-blind, Phase III study of TAS-102 plus BSC versus placebo plus BSC in patients with mCRC refractory to standard chemotherapies (RECOURSE). The RECOURSE trial randomized 800 patients 2:1 to receive 35 mg/m2 TAS-102 or placebo twice daily on days 1–5 and 8–12 every 28 days, stratified by KRAS exon 2 mutation status, time between diagnosis of metastatic disease and randomization (<18 months or not), and region (Japan or US, Europe, and Australia).Citation45 mOS, the primary endpoint, and mPFS were significantly longer following TAS-102 treatment compared with placebo (mOS, 7.1 vs 5.3 months; HR 0.68, 95% CI 0.58–0.81; P<0.001; mPFS, 2.0 vs 1.7 months; HR 0.48, 95% CI 0.41–0.57; P<0.001). Response rates were low, with an objective response rate (ORR) following TAS-102 treatment of 1.6% compared with 0.4% following placebo (P=0.29). Contrary to results from the Phase II study by Yoshino et al,Citation44 there was no significant difference in OS benefit between patients with KRAS exon 2 wild-type and patients with KRAS exon 2 mutant tumors. In the study population as a whole, grade 3–4 neutropenia was more common with TAS-102 than placebo (38% vs 0%), and febrile neutropenia was rare (4% vs 0%). Time to an Eastern Cooperative Oncology Group performance status of ≥2 was also longer following TAS-102 therapy: 5.7 versus 4.0 months (HR 0.66, 95% CI 0.56–0.78; P<0.001). This trial led to the FDA approval of TAS-102 for patients with mCRC refractory to standard therapies.Citation21
Comparison with regorafenib
TAS-102 is often compared with regorafenib, another oral agent approved for refractory mCRC. Regorafenib is a polytyrosine kinase inhibitor that blocks many targets promoting angiogenesis (VEGF receptors 1–3, TIE2, platelet-derived growth factor receptor [PDGFR], and fibroblast growth factor receptor [FGFR]) along with other oncogenic kinases (including KIT, BRAF, and RET).Citation46 The landmark regorafenib monotherapy for previously treated mCRC (CORRECT) trial randomized 760 patients with refractory mCRC 2:1 to regorafenib 160 mg daily or placebo administered on days 1–21 of a 28-day cycle.Citation47 The primary endpoint of mOS was statistically significantly longer following regorafenib therapy: 6.4 versus 5.0 months (HR 0.77, 95% CI 0.64–0.94; P=0.0052). mPFS was also significantly extended by regorafenib (1.9 vs 1.7 months; HR 0.49, 95% CI 0.42–0.58; P<0.0001), but the observed increase in ORR was not significant (1.0% of patients treated with regorafenib had an objective response compared with 0.4% of those receiving placebo; P=0.19). Fifty-four percent of patients who received regorafenib had grade 3–4 adverse events compared with only 14% of those receiving placebo; adverse events included hand–foot skin reaction (17% vs <1%), fatigue (10% vs 5%), diarrhea (7% vs 1%), hypertension (7% vs 1%), and rash (6% vs 4%).
Although both oral agents are approved by the FDA for the treatment of refractory mCRC, TAS-102 and regorafenib have important differences in their side effect profiles; thus, 2 retrospective analyses from Japan demonstrated that TAS-102 and regorafenib have similar efficacy but that regorafenib leads to more hand–foot skin reaction and a greater elevation of liver enzymes and bilirubin, whereas TAS-102 causes more neutropenia, febrile neutropenia, leukopenia, and nausea.Citation48,Citation49 The decision of how to best sequence the order of the 2 drugs is typically based on their side effect profiles. Although efficacy has not been prospectively compared head-to-head, both agents are associated with similar survival outcomes and very low ORRs. Thus, these drugs can be effective at controlling disease but are not expected to elicit tumor shrinkage as single agents.
Predictive biomarkers
A biomarker that is able to predict which patients might benefit most from TAS-102 would be highly useful, and research on potential candidates is ongoing. Early neutropenia following initiation of TAS-102 may be predictive of improved OS. A retrospective study of 95 Japanese patients treated with TAS-102 demonstrated that patients who had grade 2 or greater chemotherapy-induced neutropenia (absolute neutrophil count <1,500/mm3) during the first cycle had an improved disease control rate (52.6% vs 29.2%; odds ratio 2.67, 95% CI 1.01–7.24; P=0.045) and mPFS (2.7 vs 2.0 months; HR 0.59, 95% CI 0.38–0.91; P=0.017), although improvements in mOS were not statistically significant (6.7 vs 5.0 months; HR 0.68, 95% CI 0.41–1.10; P=0.11).Citation50 One prospective cohort study of 149 US patients with refractory mCRC who were chosen for TAS-102 treatment compared subjects who had grade 2 or greater chemotherapy-induced neutropenia at 1 month with those who did not.Citation51 mOS (14.0 vs 5.6 months; P<0.0001) and mPFS (3.0 vs 2.4 months; P=0.0096) were both longer in the neutropenic group. While these results are intriguing, the etiology of this association between neutropenia and improved survival with TAS-102 remains unclear. The authors of the US study postulate that the patients in the non-neutropenic group are rapid TAS-102 metabolizers and therefore are not receiving the same therapeutic benefit. In a post hoc analysis of the Phase II J003 study, neutropenia during the first 2 cycles was also associated with an OS benefit.Citation52 Data from the RECOURSE trial confirm the association between neutropenia and survival: patients who received TAS-102 and had grade 3 or greater neutropenia during any cycle had an OS benefit compared with patients who did not develop neutropenia; additionally, delays between TAS-102 cycles due to neutropenia were also associated with an OS benefit.Citation53 Therefore, intensifying dose and schedule for patients not experiencing grade 2–4 neutropenia may need to be considered, although this strategy should be first evaluated in a prospective trial.
Another interesting post hoc analysis of the RECOURSE trial sorted patients according to number of lines of prior treatment due to progression of disease between lines of therapy. Patients who had >3 prior lines of treatment had significantly improved OS compared with placebo (HR 0.59, 95% CI 0.44–0.78) as opposed to patients with <3 prior lines (HR 0.89, 95% CI 0.65–1.22).Citation54 This study suggests that a greater number of prior lines of therapy may predict improved survival of patients later treated with TAS-102. Also, a prespecified analysis of the RECOURSE trial looked at TAS-102 efficacy in patients aged ≥65 years compared with younger patients (<65 years of age). There were no significant differences in adverse event profiles, and the OS benefit of TAS-102 was similar regardless of age group (≥65 years: n=352, 7.0 months [TAS-102] vs 4.6 months [placebo], HR 0.62, 95% CI 0.48–0.80; P=0.0002; <65 years: n=448, 7.1 vs 5.7 months, HR 0.74, 95% CI 0.59–0.94; P=0.0130).Citation55 Thus, patient age does not appear to be a predictive biomarker of survival with TAS-102.
Defects in the DNA repair pathway within CRC cells may predict susceptibility to TAS-102. When TF-TTP is incorporated into DNA, it induces single-strand breaks that ultimately cause double-strand breaks.Citation37 In response to DNA damage, the homologous recombination repair (HRR) path way mediates DNA repair mechanisms and interacts with cell cycle checkpoints to halt DNA synthesis.Citation56 Suenaga et al analyzed genomic DNA from 181 mCRC patients treated with TAS-102 and 52 patients treated with regorafenib, specifically looking at single nucleotide polymorphisms (SNPs) in HRR pathway genes (ATM, BRCA1, BRCA2, XRCC3, FANCD2, H2AX, and RAD51) and cell cycle checkpoint genes (ATR, CHEK1, CHEK2, CDKN1A, TP53, CHE1, PIN1, and PCNA).Citation57 Genetic variants in the HRR pathway genes—ATM rs609429 and XRCC3 rs861539—were found to be predictive biomarkers of OS upon TAS-102 treatment. Interestingly, there was also an association between neutropenia and ATM rs609429. This field requires further investigation, but combination therapies with TAS-102 and HRR pathway targeting agents have a rational scientific basis.
As it is known that TK phosphorylates trifluridine to TF-TMP, leading to both inhibition of TS and, in a separate pathway, the formation of TF-TTP, which is directly incorporated into DNA, the finding that TK and TS are frequently overexpressed in CRC cells is promising for using TAS-102 in patients with CRC.Citation58 In studies using CRC cell lines, TAS-102 resistance mechanisms included decreased expression of TK and human equilibrative nucleoside transporter (hENT), the transmembrane transport protein responsible for allowing cellular influx of trifluridine.Citation59 Thus, tumors with high TK expression should be more susceptible to TAS-102 due to increased formation of TF-TMP and TF-TTP. In a pooled retrospective analysis of patients with refractory mCRC, patients with high tumor TK1 expression (cytoplasmic TK) had significantly improved mOS upon treatment with TAS-102 compared with placebo. Interestingly, it was observed that patients with high TK1 who received placebo had an overall worse prognosis than those with low TK1.Citation60 Therefore, it was concluded that high TK1 expression is a negative prognostic factor in general but a positive predictor of TAS-102 efficacy. Similarly, the hENT-1 germline SNPs rs760370 and rs9394992 have also been shown to be candidate prognostic and predictive biomarkers in retrospective studies.Citation61 TK1 and hENT-1 expression should be validated as predictive and prognostic biomarkers in future prospective studies of TAS-102.
Combination therapies with TAS-102 and ongoing clinical trials
Given the low response rate associated with TAS-102, there is significant interest in combining it with other effective therapies. Preclinical CRC xenograft models have demonstrated synergy when combining TAS-102 with bevacizumab, panitumumab, or cetuximab.Citation62,Citation63 High quality data from the ML18147 and BRiTE studies support the use of bevacizumab beyond disease progression and into later lines of CRC therapy.Citation16,Citation17 In a Phase I/II trial of TAS-102 combined with bevacizumab, Kuboki et al confirmed that standard dosing of TAS-102 (35 mg/m2 twice daily on days 1–5 and 8–12 of a 28-day cycle) and bevacizumab (5 mg/kg every 14 days) were the RP2Ds, and the study met its primary endpoint; thus, the PFS rate at 16 weeks was 42.9% (95% CI 27.8%–59.0%) in 21 evaluable patients with refractory mCRC.Citation64 mPFS and mOS were relatively impressive at 5.6 and 11.2 months, respectively, although these findings should be validated in a randomized trial. One ongoing randomized Phase II trial is comparing TAS-102 plus bevacizumab therapy with capecitabine plus bevacizumab therapy in patients with untreated mCRC deemed unsuitable for intensive therapy (defined as combination 5-FU with oxaliplatin or irinotecan, TASCO1, NCT02743221, ). While both capecitabine and TAS-102 inhibit TS, TAS-102 could be more effective in untreated mCRC patients because of direct TF-TTP incorporation into DNA and resistance to degradation by DNA glycosylase as described in the “Pharmacology” section above. Our institution has an ongoing Phase II trial of TAS-102 plus bevacizumab as maintenance therapy for patients with mCRC and stable disease or better after first-line chemotherapy (ALEXANDRIA, NCT02654639).Citation65
Table 2 Ongoing TAS-102 trials in mCRC
Another potentially exciting clinical strategy is to combine TAS-102 with the anti-EGFR mAbs cetuximab and panitumumab. Kato et al are conducting the APOLLON trial, a Japanese Phase I/II study of panitumumab combined with TAS-102 in patients with RAS wild-type, refractory mCRC (NCT02613221). Phase I results confirmed that the RP2Ds are standard panitumumab (6 mg/kg every 14 days) and TAS-102 dosing (35 mg/m2 twice daily on days 1–5 and 8–12 of a 28-day cycle), and Phase II is ongoing.Citation66
Aside from the use of combination biological agents in the form of mAbs, there are also ongoing studies using chemotherapy in combination with TAS-102. The combination of TAS-102 and oxaliplatin is supported in mouse xenograft studies.Citation67 TAS-102 and oxaliplatin are being evaluated in an ongoing Phase I/II study of patients with refractory mCRC (NCT02848079). In a Phase I study of combination irinotecan and TAS-102, the RP2D of irinotecan was 150 mg/m2 on days 1 and 15, and the RP2D of TAS-102 was 50 mg/m2/day split into 2 daily doses on days 1–5 and 8–12, both on a 28-day cycle.Citation68 There is also an ongoing Phase I study evaluating TAS-102 in combination with irinotecan and bevacizumab (NCT01916447).
Nintedanib is an oral antiangiogenic agent that inhibits VEGF receptors 1–3, PDGFRs-α/β, FGFR1–3, RET, FLT3, Lck, and Lyn.Citation69,Citation70 An ongoing Phase III trial is comparing the efficacy of nintedanib (200 mg twice daily) plus BSC compared with that of placebo plus BSC, both in 21-day courses (LUME-Colon 1, NCT02149108).Citation71 Additionally, nintedanib is being studied in combination with TAS-102 in a Phase I/II Japanese study. In the Phase I portion of the study, the RP2D of TAS-102 was established at 50 mg/m2/day on days 1–5 and 8–12, and the RP2D of nintedanib was established at 200 mg twice daily, both on a 28-day cycle; the Phase II part of the study is ongoing (UMIN00017114).Citation72
Finally, there is considerable effort underway to combine immune checkpoint inhibitors with other agents to treat microsatellite stable (MSS) mCRC. While pembrolizumab is effective in dMMR or MSI-H mCRC, no objective responses have been seen in MSS mCRC.Citation18,Citation19 Ongoing studies include a Phase II study of nivolumab, an anti-PD1 mAb, combined with TAS-102 in refractory MSS mCRC (NCT02860546) and a Phase I study of TAS-102 and oxaliplatin with or without bevacizumab or nivolumab (NCT02848443). Results from these studies will help inform future combination strategies with TAS-102.
Conclusion
TAS-102 is an excellent addition to the armamentarium of treatments for mCRC. However, valid biomarkers of potential efficacy need to be established to improve patient selection for TAS-102 therapy. Given the better outcomes of patients who develop neutropenia, future studies might evaluate dose and schedule intensification in patients without neutropenia. In addition, there are limited prospective data regarding combination strategies. The increased efficacy of TAS-102 in combination with bevacizumab is supported by Phase II data and is frequently utilized in our clinical practice, although the benefit of bevacizumab in this setting has not been confirmed in a randomized trial. Ongoing studies are evaluating a range of TAS-102 combinations and the use of TAS-102 in earlier lines of therapy. Important strides are being made in the treatment of mCRC, but more effective therapies are still needed.
Acknowledgments
We would like to thank Marion L Hartley for her edits to this review.
Disclosure
The authors report no conflicts of interest in this work.
References
- American Cancer SocietyCancer facts & figures 20172017 Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2017/cancer-facts-and-figures-2017.pdfAccessed June 30, 2017
- SEERCancer of the colon and rectum – cancer stat facts2017 Available from: https://seer.cancer.gov/statfacts/html/colorect.htmlAccessed June 30, 2017
- de GramontAFigerASeymourMLeucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancerJ Clin Oncol200018162938294710944126
- CremoliniCLoupakisFAntoniottiCFOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE studyLancet Oncol201516131306131526338525
- HeinemannVvon WeikersthalLFDeckerTFOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase 3 trialLancet Oncol201415101065107525088940
- CheesemanSLJoelSPChesterJDA ‘modified de Gramont’ regimen of fluorouracil, alone and with oxaliplatin, for advanced colorectal cancerBr J Cancer200287439339912177775
- TournigandCAndreTAchilleEFOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR studyJ Clin Oncol200422222923714657227
- LoupakisFCremoliniCMasiGInitial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancerN Engl J Med2014371171609161825337750
- HochsterHSHartLLRamanathanRKSafety and efficacy of oxaliplatin and fluoropyrimidine regimens with or without bevacizumab as first-line treatment of metastatic colorectal cancer: results of the TREE StudyJ Clin Oncol200826213523352918640933
- Van CutsemEKohneCHHitreECetuximab and chemotherapy as initial treatment for metastatic colorectal cancerN Engl J Med2009360141408141719339720
- DouillardJYOlinerKSSienaSPanitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancerN Engl J Med2013369111023103424024839
- Van CutsemELenzHJKohneCHFluorouracil, leucovorin, and irinotecan plus cetuximab treatment and RAS mutations in colorectal cancerJ Clin Oncol201533769270025605843
- Van CutsemETaberneroJLakomyRAddition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimenJ Clin Oncol201230283499350622949147
- TaberneroJYoshinoTCohnALRamucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): a randomised, double-blind, multicentre, phase 3 studyLancet Oncol201516549950825877855
- DouillardJYSienaSCassidyJFinal results from PRIME: random-ized phase III study of panitumumab with FOLFOX4 for first-line treatment of metastatic colorectal cancerAnn Oncol20142571346135524718886
- BennounaJSastreJArnoldDContinuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): a randomised phase 3 trialLancet Oncol2013141293723168366
- GrotheyASugrueMMPurdieDMBevacizumab beyond first progression is associated with prolonged overall survival in metastatic colorectal cancer: results from a large observational cohort study (BRiTE)J Clin Oncol200826335326533418854571
- LeDTUramJNWangHPD-1 blockade in tumors with mismatch-repair deficiencyN Engl J Med2015372262509252026028255
- LeDTDurhamJNSmithKNMismatch-repair deficiency predicts response of solid tumors to PD-1 blockadeScience2017357634940941328596308
- FDAFDA grants accelerated approval to pembrolizumab for first tissue/site agnostic indication2017 Available from: https://www.fda.gov/drugs/informationondrugs/approveddrugs/ucm560040.htmAccessed July 12, 2017
- MarcusLLemerySJKhasarSFDA approval summary: TAS-102Clin Cancer Res201723122924292728213365
- HeidelbergerCParsonsDGRemyDCSyntheses of 5-trifluoromethy-luracil and 5-trifluoromethyl-2′-deoxyuridineJ Med Chem196471514186018
- HeidelbergerCBooharJKampschroerBFluorinated pyrimidines. XXIV. In vivo metabolism of 5-trifluoromethyluracil-2-C-14 and 5-trifluoromethyl-2′-deoxyuridine-2-C-14Cancer Res19652537738114281103
- ReyesPHeidelbergerCFluorinated pyrimidines. XXVI. Mammalian thymidylate synthetase: its mechanism of action and inhibition by fluorinated nucleotidesMol Pharmacol19651114304220791
- SantiDVSakaiTTThymidylate synthetase. Model studies of inhibition by 5-trifluoromethyl-2′-deoxyuridylic acidBiochemistry19711019359836075146573
- EcksteinJWFosterPGFiner-MooreJWatayaYSantiDVMechanism-based inhibition of thymidylate synthase by 5-(trifluoromethyl)-2′-deoxyuridine 5′-monophosphateBiochemistry1994335015086150947999767
- AherneGWHardcastleARaynaudFJackmanALImmunoreactive dUMP and TTP pools as an index of thymidylate synthase inhibition; effect of tomudex (ZD1694) and a nonpolyglutamated quinazoline antifolate (CB30900) in L1210 mouse leukaemia cellsBiochem Pharmacol19965110129313018787544
- WebleySDWelshSJJackmanALAherneGWThe ability to accumulate deoxyuridine triphosphate and cellular response to thymidylate synthase (TS) inhibitionBr J Cancer200185344645211487279
- EmuraTNakagawaFFujiokaAOhshimoHKitazatoKThymidine kinase and thymidine phosphorylase level as the main predictive parameter for sensitivity to TAS-102 in a mouse modelOncol Rep200411238138714719072
- MarkleyJCChirakulPSologubDSigurdssonSTIncorporation of 2′-deoxy-5-(trifluoromethyl)uridine and 5-cyano-2′-deoxyuridine into DNABioorg Med Chem Lett200111182453245511549445
- HeidelbergerCDexterDLWolbergWHClinical pharmacology of 5-trifluoromethyl-2′-deoxyuridine (F3TDR)Proc Am Assoc Cancer Res19701135
- FukushimaMSuzukiNEmuraTStructure and activity of specific inhibitors of thymidine phosphorylase to potentiate the function of antitumor 2′-deoxyribonucleosidesBiochem Pharmacol200059101227123610736423
- MoghaddamABicknellRExpression of platelet-derived endothelial cell growth factor in Escherichia coli and confirmation of its thymidine phosphorylase activityBiochemistry1992314812141121461457409
- BrownNSBicknellRThymidine phosphorylase, 2-deoxy-D-ribose and angiogenesisBiochem J1998334Pt 1189693094
- van TriestBPinedoHMBlaauwgeersJLPrognostic role of thymidylate synthase, thymidine phosphorylase/platelet-derived endothelial cell growth factor, and proliferation markers in colorectal cancerClin Cancer Res2000631063107210741735
- TemminkOHEmuraTde BruinMFukushimaMPetersGJTherapeutic potential of the dual-targeted TAS-102 formulation in the treatment of gastrointestinal malignanciesCancer Sci200798677978917441963
- SuzukiNNakagawaFNukatsukaMFukushimaMTrifluorothymidine exhibits potent antitumor activity via the induction of DNA double-strand breaksExp Ther Med20112339339722977515
- SuzukiNEmuraTFukushimaMMode of action of trifluorothymidine (TFT) against DNA replication and repair enzymesInt J Oncol201139126327021491084
- HongDSAbbruzzeseJLBogaardKPhase I study to determine the safety and pharmacokinetics of oral administration of TAS-102 in patients with solid tumorsCancer200610761383139016902987
- OvermanMJVaradhacharyGKopetzSPhase 1 study of TAS-102 administered once daily on a 5-day-per-week schedule in patients with solid tumorsInvest New Drugs200826544545418528634
- DoiTOhtsuAYoshinoTPhase I study of TAS-102 treatment in Japanese patients with advanced solid tumoursBr J Cancer2012107342943422735906
- OvermanMJKopetzSVaradhacharyGPhase I clinical study of three times a day oral administration of TAS-102 in patients with solid tumorsCancer Invest200826879479918798063
- BendellJCRosenLSMayerRJPhase 1 study of oral TAS-102 in patients with refractory metastatic colorectal cancerCancer Chemother Pharmacol201576592593226370544
- YoshinoTMizunumaNYamazakiKTAS-102 monotherapy for pretreated metastatic colorectal cancer: a double-blind, randomised, placebo-controlled phase 2 trialLancet Oncol20121310993100122951287
- MayerRJVan CutsemEFalconeARandomized trial of TAS-102 for refractory metastatic colorectal cancerN Engl J Med2015372201909191925970050
- WilhelmSMDumasJAdnaneLRegorafenib (BAY 73-4506): a new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activityInt J Cancer2011129124525521170960
- GrotheyAVan CutsemESobreroARegorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trialLancet2013381986330331223177514
- MasuishiTTaniguchiHHamauchiSRegorafenib versus trifluridine/tipiracil for refractory metastatic colorectal cancer: a retrospective comparisonClin Colorectal Cancer2017162e15e2227670892
- SuedaTSakaiDKudoTEfficacy and safety of regorafenib or TAS-102 in patients with metastatic colorectal cancer refractory to standard therapiesAnticancer Res20163684299430627466548
- HamauchiSYamazakiKMasuishiTNeutropenia as a predictive factor in metastatic colorectal cancer treated with TAS-102Clin Colorectal Cancer2017161515727522626
- KasiPMKotaniDCecchiniMChemotherapy induced neutropenia at 1-month mark is a predictor of overall survival in patients receiving TAS-102 for refractory metastatic colorectal cancer: a cohort studyBMC Cancer20161646727412464
- NishinaTYoshinoTShinozakiEOnset of neutropenia as an indicator of treatment response in the randomized phase II study of TAS-102 vs placebo in Japanese patients with metastatic colorectal cancer (study J003-10040030)J Clin Oncol201634Suppl Abstr 3557
- OhtsuAYoshinoTFalconeAOnset of neutropenia as an indicator of treatment response in the phase 3 RECOURSE trial of trifluridine/tipiracil (TAS-102) versus placebo in patients with metastatic colorectal cancerJ Clin Oncol201735Suppl 4S Abstr 775
- Van CutsemEOhtsuALegerCEffect of number of prior lines versus prior regimens in pts receiving trifluridine/tipiracil (TAS-102)J Clin Oncol201735Suppl 4S Abstr 720
- Van CutsemEBenedettiFMMizuguchiHTAS-102 versus placebo (PBO) in patients (pts) ≥ 65 years (y) with metastatic colorectal cancer (mCRC): an age-based analysis of the recourse trialJ Clin Oncol201634Suppl 4S Abstr 638
- HustedtNDurocherDThe control of DNA repair by the cell cycleNat Cell Biol20161911928008184
- SuenagaMSchirripaMCaoSGenetic variants of DNA repair-related genes predict efficacy of TAS-102 in patients with refractory metastatic colorectal cancerAnn Oncol20172851015102228453695
- ShintaniMUranoMTakakuwaYKurodaMKamoshidaSImmunohistochemical characterization of pyrimidine synthetic enzymes, thymidine kinase-1 and thymidylate synthase, in various types of cancerOncol Rep20102351345135020372850
- TemminkOHBijnsdorpIVPrinsHJTrifluorothymidine resistance is associated with decreased thymidine kinase and equilibrative nucleoside transporter expression or increased secretory phospholipase A2Mol Cancer Ther2010941047105720371715
- YoshinoTShinozakiEYamazakiKEffect of thymidine kinase 1 expression on prognosis and treatment outcomes in refractory metastatic colorectal cancer: results from two randomized studies of TAS-102 versus a placeboJ Clin Oncol201735Suppl 4S Abstr 529
- ZhangWSuenagaMSchirripaMGenetic variants of hENT-1 to predict efficacy of TAS-102 in patients with refractory metastatic colorectal cancerJ Clin Oncol201634Suppl Abstr 3580
- TsukiharaHNakagawaFSakamotoKEfficacy of combination chemotherapy using a novel oral chemotherapeutic agent, TAS-102, together with bevacizumab, cetuximab, or panitumumab on human colorectal cancer xenograftsOncol Rep20153352135214225812794
- BabaYTamuraTSatohYPanitumumab interaction with TAS-102 leads to combinational anticancer effects via blocking of EGFR-mediated tumor response to trifluridineMol Oncol20171181065107728486761
- KubokiYNishinaTShinozakiEAn investigator initiated multicenter phase I/II study of TAS-102 with bevacizumab for metastatic colorectal cancer refractory to standard therapies (C-TASK FORCE)J Clin Oncol201533Suppl Abstr 3544
- SalemMEWangHFakihMAn open-label, multi-center, phase 2 study of switch maintenance with TAS-102 plus bevacizumab following oxaliplatin or irinotecan-based fluoropyrimidine-containing induction chemotherapy in patients with metastatic colorectal cancer: ALEXANDRIA studyJ Clin Oncol201634Suppl Abstr TPS3624
- KatoTKagawaYKomatsuYA phase I/II study for panitumumab combined with TAS-102 in patients with RAS wild-type metastatic colorectal cancer (APOLLON study): phase I resultsJ Clin Oncol201735Suppl 4S Abstr 770
- NukatsukaMNakagawaFTakechiTEfficacy of combination chemotherapy using a novel oral chemotherapeutic agent, TAS-102, with oxaliplatin on human colorectal and gastric cancer xenograftsAnticancer Res20153594605461526254349
- DoiTYoshinoTFuseNPhase I study of TAS-102 and irinotecan combination therapy in Japanese patients with advanced colorectal cancerInvest New Drugs20153351068107726163340
- MrossKBuchertMFrostAVascular effects, efficacy and safety of nintedanib in patients with advanced, refractory colorectal cancer: a prospective phase I subanalysisBMC Cancer20141451025012508
- HilbergFRothGJKrssakMBIBF 1120: triple angiokinase inhibitor with sustained receptor blockade and good antitumor efficacyCancer Res200868124774478218559524
- Van CutsemEYoshinoTHockeJOum’HamedZStudenyMTaberneroJRationale and design for the LUME-colon 1 study: a randomized, double-blind, placebo-controlled phase III trial of nintedanib plus best supportive care versus placebo plus best supportive care in patients with advanced colorectal cancer refractory to standard treatmentClin Colorectal Cancer2016151919426603056
- NishinaTKubokiYShinozakiSA multicentre phase I/II study of TAS-102 with nintedanib in patients with metastatic colorectal cancer refractory to standard therapies (N-task force: EPOC1410); phase I resultsAnn Oncol201627Suppl 6 Abstr 472P