
Abstract
Introduction
Acute myeloid leukemia (AML) rarely involves the central nervous system (CNS). Little is known about the clinical course in adult AML patients since most studies examined pediatric patients. Therefore, this study analyzed the data of patients treated in three prospective trials of the “Study Alliance Leukemia” (SAL) study group for CNS involvement.
Methods
In all, 3,261 AML patients included in the prospective AML96, AML2003, and AML60+ trials of the SAL study group were analyzed. Symptomatic patients underwent cerebrospinal fluid (CSF) puncture and CNS involvement was diagnosed depending on morphology and/or flow cytometry of the CSF. Cytogenetic, molecular, clinical, and laboratory parameters were analyzed in order to identify risk factors.
Results
A total of 55 patients had proven symptomatic CNS involvement. Significantly more patients revealed CNS involvement at relapse (34 patients, 2.9%) compared with first diagnosis (21 patients, 0.6%), p<0.001. CNS involvement at initial diagnosis had a significantly higher frequency in patients with complex aberrant karyotypes, high serum lactate dehydrogenase activity, French–American–British M5 subtype, FLT3–internal tandem duplication (ITD) mutations alone, and co-occurrence of a FLT3–ITD and NPM1 mutation. Furthermore, AML patients with CNS involvement at diagnosis had an inferior outcome compared with patients without CNS involvement even if treated with intrathecal chemotherapy with an overall survival of 11% versus 30% at 5 years, p=0.004.
Conclusion
This study analyzed the largest data set of adult AML patients with proven CNS involvement reported so far. The data demonstrated very low prevalence of CNS involvement at initial diagnosis in adult patients with AML, and described new risk factors. In patients with risk factors, intense diagnostic and treatment strategies should be employed in the future.
Introduction
In contrast to acute lymphoblastic leukemia, acute myeloid leukemia (AML) rarely involves the central nervous system (CNS) in adult patients while it is more common in pediatric AML patients.Citation1,Citation2 Therefore, routine diagnostic evaluation or prophylactic CNS therapy in adult AML is not performed, although some authors recommend a routine evaluation when hyperleukocytosis is present at diagnosis.Citation3,Citation4 Bojsen-Moller and Nielsen performed an autopsy study and found leukemic CNS infiltrates in 46% of all AML patients, which could point to higher rates of asymptomatic CNS involvement, but might be biased since the remission status of the studied patients was not approximated, and an autopsy study usually includes more patients with unfavorable and relapsed disease.Citation5 However, symptoms of CNS involvement may develop later during disease progression or at relapse, which might influence the outcome. Furthermore, CNS involvement might be diagnosed through the appearance of either leukemic blasts in the cerebrospinal fluid (CSF) and/or with intracerebral myeloid sarcoma or meningeal AML. Risk factors identified so far include high initial white blood cell (WBC) count in the peripheral blood and AML M5 French–American–British (FAB) morphology.Citation6 Several treatment options such as cranial and/or neuro-axis irradiation and intrathecal therapy (ITC) with methotrexate (MTX) and/or cytosine arabinoside (Ara-C) and glucocorticoids along with systemic chemotherapy are widely accepted.Citation7–Citation10 Little is known regarding CNS involvement in adult AML and its impact on survival since most studies examined pediatric patients or only a limited number of patients.Citation8,Citation11–Citation15 Therefore, the present study analyzed CNS involvement in patients with AML treated in the prospective AML96, AML2003, and AML60+ trials of the “Study Alliance Leukemia” (SAL) study group for a better understanding of this rare AML entity and to identify patient populations that are at increased risk for CNS disease. This report represents the largest cohort of AML patients analyzed with respect to CNS involvement to date.
Patients and methods
Between February 1996 and November 2009, 3,526 adult patients with non-acute promyelocytic leukemia AML were included in the prospective AML96, AML2003, and AML60+ trials of the SAL. The studies were approved by the ethics committees of the University of Dresden and all other participating centers. A list of participating centers and ethics committees can be found in the Supplementary material. The protocols were in agreement with the Helsinki declaration and registered with NCT numbers 00180115 (AML96), 00180102 (AML2003), and 00180167 (AML60+). Written informed consent was obtained from all patients. Data were collected and certified by the SAL Data Center.
In the AML96 protocol, patients <60 years of age were treated with double induction chemotherapy including standard- and intermediate-dose mitoxantrone, Ara-C, etoposide, and amsacrine and stratified post-remission therapy in different cytogenetic risk groups. Intermediate risk patients with a human leukocyte antigen (HLA)-identical sibling donor were referred to allogeneic hematopoietic stem cell transplant (HSCT). High risk patients were referred to related or unrelated HLA-compatible allogeneic HSCT.Citation16 Patients without donors were randomized to intermediate-dose or high-dose Ara-C and mitoxantrone and subsequent autologous HSCT. Patients >60 years of age received double induction chemotherapy with daunorubicin and standard-dose Ara-C followed by consolidation therapy consisting of intermediate-dose Ara-C and amsacrine.Citation17
In the AML60+ trial, patients >60 years of age were included and randomized between the treatment arm of the AML96 study for elderly patients and induction with intermediate-dose Ara-C and mitoxantrone. Allogeneic HSCT was optional for fit patients.Citation18
The AML2003 trial included patients below the age of 61 years. Patients were randomized up-front in a two-by-two factorial design with the two factors high-dose Ara-C alone versus high-dose Ara-C plus mitoxantrone and amsacrine for consolidation and standard versus risk adapted intensified consolidation including early allogeneic HSCT during induction therapy and autologous HSCT. All patients received a 3+7 regimen with daunorubicin and Ara-C as induction chemotherapy.
In the presence of neurologic or psychiatric abnormalities, lumbar puncture was performed to confirm or exclude CNS involvement through microscopy and/or flow cytometry of the CSF in all three prospective trials. CNS disease was treated with ITC with MTX, Ara-C, and glucocorticoids. Treatment response and treatment outcome were defined according to the recommended consensus criteria.Citation19 Data of proven extramedullary manifestations were available in 3,261 patients, which were included in this study. The patient characteristics are summarized in . The distributions of cytogenetic, molecular, clinical, and laboratory parameters were compared in order to identify risk factors for CNS involvement. The chi-square test was used for significance testing of comparisons in categorical variables and the Mann–Whitney U test for continuous variables. Kaplan–Meier method was used to estimate the overall survival (OS). Survival distributions were compared using the log-rank test.
Table 1 Comparison of patients’ characteristics between AML patients with and without CNS involvement at diagnosis
Results
For this study, all 3,261 patients were analyzed with a median follow-up of 5.1 years. A total of 21 patients had CNS involvement at the time of initial presentation resulting in a prevalence of 0.6%. CNS involvement at AML relapse had a statistically higher incidence of 2.9% with 34 affected patients among 1,154 patients at relapse versus 21 of 3,261 patients at initial diagnosis (p<0.010).
Characteristics and outcome of CNS disease at initial diagnosis were further analyzed (). The majority of patients (n=18, 86%) had de novo AML. The median age of these patients was 54 years (range 22–77 years). Gender and age were equally distributed between patients with CNS involvement and patients without CNS involvement. Extramedullary AML other than CNS was present more frequently in patients with CNS involvement as compared to patients without CNS involvement (n=13, 62% vs n=344, 11%, p<0.001).
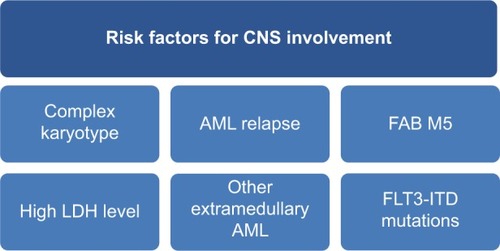
Significantly more patients with CNS involvement had FLT3–internal tandem duplication (ITD) mutations (n=8, 44% vs n=611, 21%, p=0.017) and when grouping FLT3–ITD and NPM1 mutations, there was a statistically significant higher occurrence of combined FLT3–ITD and NPM1 mutations in patients with CNS involvement as compared to those without CNS involvement (n=7, 44% vs n=335, 12%, p=0.002). Furthermore, patients with CNS involvement exhibited significantly higher levels of lactate dehydrogenase activity (LDH) (log U/l 2.81 vs 2.59, p=0.023) (base 10 logarithm), higher frequencies of FAB M5 morphology (n=8, 38% vs n=417, 13%, p=0.001) compared with patients without CNS involvement. When analyzing patients at initial diagnosis, complex aberrant karyotypes were significantly more frequent in patients with CNS involvement compared with those without CNS involvement (n=6, 29% vs n=398, 12%, p=0.025).
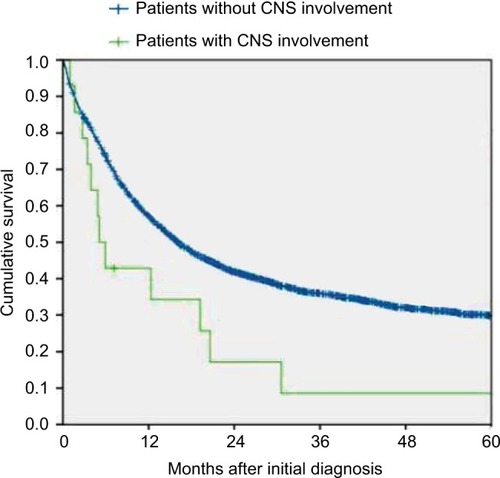
Fourteen of 21 patients with CNS involvement at initial diagnosis were treated with ITC. Survival and complete remission rates for these patients were analyzed. Patients with CNS involvement reached complete remission less frequently than patients without CNS involvement (n=10, 48% vs n=2,317, 72%, p=0.016), and had a significantly inferior outcome even if treated with ITC with an OS of 11% (95% confidence interval [CI], 0%–25%) versus 30% (95% CI, 28%–32%) at 5 years, p=0.004 ().
Figure 1 Overall survival of treated patients with CNS involvement at initial diagnosis of AML (n=21) and patients without CNS involvement at initial diagnosis of AML (n=3,240) within the SAL trials. Log-rank Mantel-Cox p=0.029.
Discussion
AML rarely involves the CNS in adults and there are only a few published studies with controversial results.Citation9,Citation20,Citation21 CNS involvement may remain asymptomatic. Diagnostic lumbar puncture or prophylactic ITC is not routinely recommended without CNS symptoms. Systemic therapy for isolated CNS involvement in parallel to cranial irradiation and/or ITC seems to be necessary in order to avoid marrow relapse.Citation22,Citation23
This study analyzes the largest data set of adult AML patients with proven CNS involvement reported so far. An overall prevalence of 0.6% was found at initial diagnosis which is lower than previously reported prevalence ranging between 2% and 8%.Citation1,Citation24,Citation25 One possible reason of higher rates in the earlier reports could be the fact that some of these studies were done in pediatric patients while others included promyelocytic leukemia, used imaging studies with magnetic resonance imaging instead of lumbar puncture, or included patients at relapse as well.Citation24–Citation28 However, some of these imaging data might be conflicting since they possibly rather represent intracerebral myeloid sarcoma, meningeal AML, or simply inflammatory enhancement. Furthermore, the data from the present analysis reflect only the patients in whom manifestation of CNS involvement was clinically apparent due to neurological and/or psychiatric symptoms. Thus, this could implicate that the real prevalence including asymptomatic CNS involvement is higher, although another study suggested that this might not be the case.Citation29
In this analysis, symptomatic CNS involvement was frequently accompanied by other extramedullary AML manifestations and higher prevalence of FLT3–ITD mutations, whereas NPM1 mutations alone had no significant higher incidence in these patients. As previously shown, FAB M5 morphology, complex aberrant karyotype, higher LDH levels, and higher WBC count at diagnosis represent risk factors for CNS involvement.Citation3,Citation8,Citation13,Citation25 Interestingly, other studies showed an association of CNS involvement in AML with certain cytogenetic abnormalities such as inv(16), del(5q), del(7q), trisomy of chromosome 8, t(8;21), and abnormalities of chromosome 11q23, which could not be confirmed for patients with CNS involvement at the initial diagnosis of AML.Citation25,Citation30,Citation31
However, upon extending the data analysis by including also CNS involvement of AML at relapse, statistically significant higher incidence of CNS involvement was confirmed for patients with trisomy of chromosome 8, trisomy of chromosome 22, t(9;11), t(6;11), and complex karyotype. The study could not confirm a higher prevalence for patients with t(8;21), inv(16), monosomy of chromosome 5, or monosomy of chromosome 7 (). In total, abnormalities of chromosome 11q23 were evident in 20% of all AML patients with CNS involvement either at initial diagnosis or at relapse of CNS involvement (n=11/55). In 7 patients 11q23 abnormalities were only detected using FISH analysis (Fluorescence in situ hybridization). In these cases the 11q23 translocation was cryptic by karyotyping. This reflects a higher prevalence of 11q23 abnormalities than the estimated 6% in AML with a higher occurrence in myelomonocytic AML.Citation32,Citation33 Hence, data from the present analysis confirm the previously reported higher occurrence of 11q23 abnormalities of patients with CNS disease as reported by others recently.Citation13,Citation25,Citation34
Table 2 Comparison of cytogenetic profile between AML patients with and without CNS involvement at diagnosis or relapse
The impact of CNS involvement on long-term treatment outcome has been discussed controversially.Citation4,Citation8,Citation10,Citation21 Recently, Shihadeh et al suggested that adult AML patients with CNS involvement have poor OS.Citation25 The present study could confirm this finding based on the largest number of patients with CNS involvement and define further risk factors (FLT3–ITD mutations, complex aberrant karyotypes) that might help to identify AML patients at risk for CNS involvement (). However, due to the low frequency and low ITC chemotherapy-initiation at diagnosis in the three reported AML trials, differently sized patient cohorts have been compared and the statistical impact must be interpreted carefully. In summary, this analysis suggests a very low frequency of symptomatic CNS AML involvement in adults. Because of the obviously poor prognosis of CNS involvement, screening for risk factors of CNS involvement at diagnosis in symptomatic AML patients with suspicion for CNS involvement may be useful to identify a patient population benefiting from intensified treatment strategies in the future.
Figure 2 Risk factors for symptomatic AML patients with potential CNS involvement at initial diagnosis of AML.
Acknowledgments
The contribution of all patients and physicians in the various trials of the German SAL is highly appreciated. This study was presented in part at the 17th Annual Congress of the European Hematology Association, June 14–17, 2012, Amsterdam, the Netherlands.
Disclosure
The authors report no conflicts of interests in this work.
References
- AbbottBLRubnitzJETongXClinical significance of central nervous system involvement at diagnosis of pediatric acute myeloid leukemia: a single institution’s experienceLeukemia200317112090209614523477
- ReesJKGrayRGSwirskyDHayhoeFGPrincipal results of the Medical Research Council’s 8th acute myeloid leukaemia trialLancet (London, England)19862851812361241
- CassilethPASylvesterLSBennettJMBeggCBHigh peripheral blast count in adult acute myelogenous leukemia is a primary risk factor for CNS leukemiaJ Clin Oncol1988634954983162514
- DöhnerHEsteyEHAmadoriSDiagnosis and management of acute myeloid leukemia in adults: Recommendations from an international expert panel, on behalf of the European LeukemiaNetBlood2010115345347419880497
- Bojsen-MøllerMNielsenJLCNS involvement in leukaemia. An autopsy study of 100 consecutive patientsActa Pathol Microbiol Immunol Scand A19839142092166575578
- StewartDJKeatingMJMcCredieKBNatural history of central nervous system acute leukemia in adultsCancer19814711841967459807
- BakstRLTallmanMSDouerDYahalomJHow I treat extramedullary acute myeloid leukemiaBlood2011118143785379321795742
- CastagnolaCNozzaACorsoABernasconiCThe value of combination therapy in adult acute myeloid leukemia with central nervous system involvementHaematologica19978255775809407724
- MayadevJSDouglasJGStorerBEAppelbaumFRStorbRImpact of cranial irradiation added to intrathecal conditioning in hematopoietic cell transplantation in adult acute myeloid leukemia with central nervous system involvementInt J Radiat Oncol Biol Phys201180119319820584584
- SandersKEHaCSCortes-FrancoJEKollerCAKantarjianHMCoxJDThe role of craniospinal irradiation in adults with a central nervous system recurrence of leukemiaCancer2004100102176218015139061
- BommerMvon HarsdorfSDöhnerHBunjesDRinghofferMNeoplastic meningitis in patients with acute myeloid leukemia scheduled for allogeneic hematopoietic stem cell transplantationHaematologica2010951119621972
- FrickJTitchPSHansenRMSuccessful treatment of meningeal leukemia using systemic high dose cytosine arabinosideJ Clin Oncol198423653686726293
- JohnstonDLAlonzoTAGerbingRBLangeBJWoodsWGRisk factors and therapy for isolated central nervous system relapse of pediatric acute myeloid leukemiaJ Clin Oncol200523369172917816361619
- KobayashiRTawaAHanadaRExtramedullary infiltration at diagnosis and prognosis in children with acute myelogenous leukemiaPediatr Blood Cancer200748439339816550530
- PuiCHHowardSCCurrent management and challenges of malignant disease in the CNS in paediatric leukaemiaLancet Oncol20089325726818308251
- SchaichMRölligCSoucekSCytarabine dose of 36 g/m2 compared with 12 g/m2 within first consolidation in acute myeloid leukemia: results of patients enrolled onto the prospective randomized AML96 studyJ Clin Oncol201129192696270221606413
- RölligCThiedeCGramatzkiMA novel prognostic model in elderly patients with acute myeloid leukemia: results of 909 patients entered into the prospective AML96 trialBlood2010116697197820442365
- RölligCKramerMHanelMInduction treatment in elderly patients with acute myeloid leukemia (AML): randomized comparison of intermediate-dose cytarabine plus mitoxantrone (IMA) versus standard-dose cytarabine plus daunorubicin (DA) in 492 aml patients >60 years – resultsBlood201511621334
- ChesonBDBennettJMKopeckyKJRevised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid LeukemiaJ Clin Oncol200321244642464914673054
- OshimaKKandaYYamashitaTCentral nervous system relapse of leukemia after allogeneic hematopoietic stem cell transplantationBiol Blood Marrow Transplant200814101100110718804039
- WoodsWGKobrinskyNBuckleyJIntensively timed induction therapy followed by autologous or allogeneic bone marrow transplantation for children with acute myeloid leukemia or myelodysplastic syndrome: a Childrens Cancer Group pilot studyJ Clin Oncol1993118144814578336184
- SimoneJVTreatment of meningeal leukemiaJ Clin Oncol1984253573586726292
- SteinherzPJerebBGalicichJTherapy of CNS leukemia with intra-ventricular chemotherapy and low-dose neuraxis radiotherapyJ Clin Oncol198539121712263861774
- GrierHEGelberRDCamittaBMPrognostic factors in childhood acute myelogenous leukemiaJ Clin Oncol198757102610323474356
- ShihadehFReedVFaderlSCytogenetic profile of patients with acute myeloid leukemia and central nervous system diseaseCancer2012118111211721692072
- Martínez-CuadrónDMontesinosPPérez-sirventMCentral nervous system involvement at first relapse in patients with acute myeloid leukemiaHaematologica20119691375137921565904
- de BottonSSanzMAChevretSExtramedullary relapse in acute promyelocytic leukemia treated with all-trans retinoic acid and chemotherapyLeukemia2006201354116307026
- SpecchiaGLo CocoFVignettiMExtramedullary involvement at relapse in acute promyelocytic leukemia patients treated or not with all-trans retinoic acid: a report by the Gruppo Italiano Malattie Ematologiche dell’AdultoJ Clin Oncol200119204023402811600603
- MorrisonFSKopeckyKJHeadDRLate intensification with POMP chemotherapy prolongs survival in acute myelogenous leukemia–results of a Southwest Oncology Group study of rubidazone versus adriamycin for remission induction, prophylactic intrathecal therapy, late intensification, and lLeukemia1992677087141625490
- HolmesRKeatingMJCorkAA unique pattern of central nervous system leukemia in acute myelomonocytic leukemia associated with inv(16)(p13q22)Blood1985655107110783857943
- GhaddarHMPlunkettWKantarjianHMLong-term results following treatment of newly-diagnosed acute myelogenous leukemia with continuous-infusion high-dose cytosine arabinosideLeukemia199488126912748057660
- GrimwadeDHillsRKMoormanAVRefinement of cytogenetic classification in acute myeloid leukaemia: determination of prognostic significance of rarer recurring chromosomal abnormalities amongst 5,876 younger adult patients treated in the UK Medical Research Council trialsBr J Haematol2010116354365
- SorensenPHBChenCSSmithFOMolecular rearrangements of the MLL gene are present in most cases of infant acute myeloid leukemia and are strongly correlated with monocytic or myelomonocytic phenotypesJ Clin Invest19949314294378282816
- ChangHBrandweinJYiQ-LChunKPattersonBBrienBExtramedullary infiltrates of AML are associated with CD56 expression, 11q23 abnormalities and inferior clinical outcomeLeuk Res200428101007101115289011