
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Purpose
To investigate the diagnostic values of human epididymis protein 4 (HE4), carbohydrate antigen 125 (CA125), carbohydrate antigen 19-9 (CA19-9), and carcinoembryonic antigen (CEA) for ovarian tumors.
Methods
The participants were divided into three groups: 386 healthy women (control group), 262 patients with benign ovarian tumors (the benign group), and 196 patients with malignant pelvic tumors (the malignant group). The serum levels of HE4, CA125, CA19-9, and CEA were analyzed by electrochemiluminescent immunoassay.
Results
It showed that serum levels of HE4, CA125, CA19-9, and CEA of patients with malignant ovarian tumors were significantly higher than those in the control group and benign group (P<0.01). HE4 had a high specificity (96.56%) in malignant ovarian tumors. The tumor markers HE4, CA125, CA19-9, and CEA had a sensitivity of 63.78%, 62.75%, 35.71%, and 38.78%, respectively. The combined use of two or more tumor markers (parallel test) had a higher diagnostic sensitivity but lower specificity than a single tumor marker. The combined efficiency of HE4 and CA125 was the highest, with a sensitivity and specificity of 80.10% and 69.08%, respectively. HE4 and CA125 combined with the Risk of Ovarian Malignancy Algorithm provided an efficient means of screening and diagnosis of ovarian malignancies. The diagnostic sensitivity increased to 88.52% when three or four tumor markers were used but showed no significant difference compared with the combination of HE4 and CA125 (P>0.05).
Conclusion
The combination of three or four tumor markers did not improve the diagnostic efficacy when compared with the combination of HE4 and CA125.
Introduction
The incidence of gynecological pelvic tumors is high. In particular, ovarian cancer is one of the most common malignant tumors in the female reproductive system, and the mortality rate is the highest.Citation1 There are nearly no clinical symptoms or signs at the early stage of most ovarian cancer patients. Studies have shown that only <25% of patients with ovarian cancer can be diagnosed at the early stage, and 70% of patients are diagnosed at the advanced stage.Citation2 In addition, the outcome of treatment and prognosis of ovarian cancer are poor, the 5-year survival rate is 20%–30%, and the recurrence rate is very high. In the early stage of ovarian cancer, the 5-year survival rate can reach 80%–90% if effective treatment is available.Citation2 Hence, finding effective early diagnostic markers is of great significance for the treatment and prognosis of malignant ovarian tumors.
Tumor markers play an important role in the early diagnosis and prognosis of gynecological malignancies. Carbohydrate antigen 125 (CA125) has been utilized to help predict the presence of malignancy in patients with a pelvic mass. However, the specificity of CA125 in tissues and organs is low; at the same time, it also appears in different degrees of increase in physiological condition (such as pregnancy) and nonmalignant diseases (such as endometriosis, pelvic inflammation, and uterine fibroids).Citation5 In addition, carbohydrate antigen 19-9 (CA19-9) and carcinoembryonic antigen (CEA) are traditional screening criteria for gynecological pelvic malignancies without high specificity. In many gynecological pelvic benign diseases such as inflammation and endometriosis, the levels of CA19-9 and CEA in the serum of pelvic benign tumor patients also increased.Citation6 Human epididymis protein 4 (HE4), a novel tumor marker, is highly expressed in ovarian cancer and endometrial cancer but lowly expressed in adjacent tissues, normal tissues, and benign tumors. As a single tumor marker, HE4 had the highest sensitivity for detecting ovarian cancer.Citation7
Studies have shown that combined detection of multiple tumor markers can improve the sensitivity and efficacy of diagnosis and help reduce the incidence of misdiagnosis.Citation8 In our previous study, we found that the combined use of HE4 and CA125 improved the diagnostic efficacy.Citation9 In this study, we tested the serum levels of HE4, CA125, CA19-9, and CEA in 458 patients with ovarian tumors in order to analyze the diagnostic value of the combined use of tumor markers in gynecological pelvic tumors.
Patients and methods
Patient participation groups
This study was carried out in Fujian Provincial Hospital and Fujian Provincial Hospital South Branch between June 2013 and June 2017. All participants were divided into three groups: 386 healthy women (the control group), who have no serious organ diseases such as heart, liver, lung, stomach, and gynecological diseases and have no family history of tumor; 262 patients with benign ovarian tumors confirmed by pathology (the benign group); and 196 patients with malignant ovarian tumors confirmed by pathology (the malignant group) ().
Table 1 Patient participant groups
Serum tumor marker detection
Fasting venous blood (3–4 mL) was preoperatively collected from 458 patients and centrifuged to obtain the serum. The serum levels of HE4, CA125, CA19-9, and CEA were analyzed by electrochemiluminescent immunoassay (Roche Modular E170 electrochemiluminescence). Reagent test kits were purchased from Roche Diagnostic Reagent Company (Shanghai, China). The cutoff values for the tumor markers are listed in . The test is positive when any index is higher than the reference range. The Risk of Ovarian Malignancy Algorithm (ROMA) was calculated by the ovarian cancer risk prediction model using serum HE4 and CA125 levels.
Table 2 The cutoff values for the four tumor markers
When the specificity of Roche Elecsys was 75%, pre-menopausal ROMA ≥11.4% was considered as high-risk ovarian epithelial cancer and postmenopausal ROMA ≥29.9% was considered as high-risk ovarian epithelial cancer.Citation9,Citation10
Statistical analyses
SPSS 22.0 software and MedcCalc software were used for statistical analysis. Non-normal quantitative data were expressed as in the form of the median and four quartiles of M (P25 and P75), comparison among groups was conducted using the nonparametric Kruskal–Wallis H test, and then the nonparametric Mann–Whitney U test was used for comparing two groups. The chi-square test was used for the analysis of categorical data. P<0.05 was considered as statistically significant. Logistic regression models were estimated, and receiver operator characteristic (ROC) curves were constructed. The area under the ROC curve (AUC) was compared between two markers or panels of markers.
Ethical review
The study was approved by Provincial Clinical College of Fujian Medical University’s Ethics Committee (no K2013-005-01), and a waiver for individual patient consent for this retrospective study was also obtained from this ethics committee. To maintain confidentiality, the names of patients were not retrieved. The records of patients were kept confidential, and persons outside the research team had no access to it. The data in the extraction forms were entered into a password-protected computer that was accessible to the researchers only.
Results
Comparison of tumor markers between benign and malignant groups
The most common benign neoplasms were mucinous and serous cystadenomas, which together accounted for 36.25% of the women with benign disease (). For the malignancies, there were 105 (53.57%) serous, 32 (16.32%) mucinous, 26 (13.27%) endometrioid, and 33 (16.84%) nonepithelial tumors. In patients with epithelial ovarian cancer, 17 (10.43%) patients were diagnosed with surgical Stage I disease, 22 (13.50%) patients were diagnosed with Stage II disease, 101 (61.96%) patients were diagnosed with Stage III disease, and 23 (14.11%) patients were diagnosed with Stage IV disease.
Serum levels of HE4, CA125, CA19-9, and CEA of the malignant groups were significantly higher than those in the control group and benign group (P<0.01). Serum levels of these four tumor markers in the malignant group were higher than those in the benign group (P<0.01, ).
Table 3 Serum levels of the four tumor markers in patients with malignant and benign ovarian tumors
The efficacy of the combined use of four tumor markers in benign and malignant groups
In this study, the cutoff values for the four tumor markers were 140 pM for HE4, 35 U/mL for CA125, 27 U/mL for CA19-9, and 5 ng/mL for CEA. The tumor markers HE4, CA125, CA19-9, and CEA had a sensitivity of 63.78%, 62.75%, 35.71%, and 38.78%, respectively.
The serum levels of such markers in patients with surgical Stage I disease were relatively lower. For example, when examining ovarian cancer patients with normal serum CA125 levels, HE4 levels were found to be elevated in >60% of these patients. Conversely, when examining patients with benign tumors who had elevated CA125 levels, HE4 levels were not as frequently elevated as those in the serum of these patients.
The combined use of two or more tumor markers (parallel test) had a higher diagnostic sensitivity in different degrees than any single tumor marker. The combined efficiency of HE4 and CA125 was the highest of the two tumor markers’ combination, with a sensitivity and specificity of 80.10% and 69.08%, respectively.
HE4 showed a higher overall specificity (96.56%) than CA125 (70.61%, P<0.01) in the diagnosis of ovarian cancer. ROMA had a high sensitivity (81.12%) and specificity (83.97%) in the diagnosis of ovarian cancer.
When three or four tumor markers were used, the diagnostic efficiency showed no significant difference compared with the HE4 and CA125 combination (P>0.05). There was no difference of sensitivity between different combined uses of tumor markers ().
Table 4 Efficacy of combined detection of the four tumor markers in 458 patients
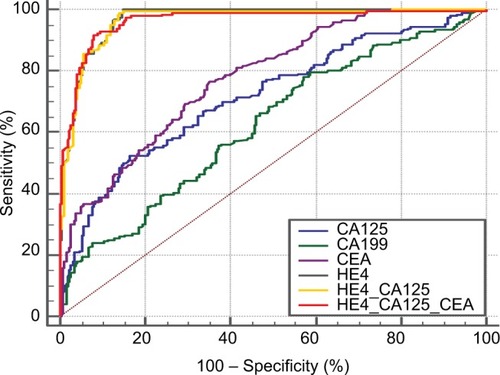
As shown in , the AUCs of the tumor markers ROC, CA125, CA199, and HE4 were 0.967 (95% CI, 0.947–0.985), 0.717 (95% CI, 0.673–0.758), 0.624 (95% CI, 0.578–0.668), and 0.777 (95% CI, 0.736–0.814), respectively. The AUC was 0.973 (95% CI, 0.949–0.989) when HE4 and CA125 were combined (). When HE4, CA125, and CEA were combined, the AUC was 0.972 (95% CI, 0.942–0.978).
Figure 1 The detection of the ROC curve of ovarian cancer by four tumor markers.
Abbreviation: ROC, receiver operator characteristic.
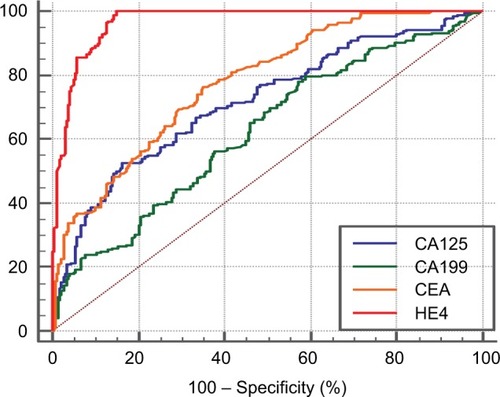
Figure 2 The ROC curve of four tumor markers in single and combined detections of ovarian cancer.
Abbreviation: ROC, receiver operator characteristic.
Discussion
Early detection and early diagnosis are essential to improve survival in patients with ovarian cancer. However, early ovarian cancer is almost asymptomatic, and there are no effective early diagnosis strategies. Therefore, improving the rate of early diagnosis is the fundamental way to improve the overall prognosis and reduce the cost of treatment for patients with ovarian cancer.Citation1,Citation3,Citation11 Tumor markers are expressed in tumor cells of the host to produce reaction substance, and there is little in serum in normal circumstances.Citation12 Different types of tumor markers with different tumors have certain specificity, and tumor markers are important to tumor diagnosis, assessment, prognosis, and recurrence and metastasis prediction in early detection of tumor markers.Citation13 At present, there are many tumor markers such as HE4, CA125, CA19-9, and CEA, which are used in tumor screening.Citation14,Citation15 Studies have shown that 93% of serous epithelial ovarian cancer, 100% of endometrial epithelial cancer, and 50% of clear-cell ovarian cancer were highly expressed of HE4, whereas mucinous ovarian cancer did not express HE4.Citation16,Citation17 HE4 has a high specificity and an appropriate sensitivity for ovarian cancer, making it useful in the early diagnosis of ovarian cancer.
CA125 is a widely used screening marker of gynecological malignant pelvic tumors. It is highly expressed in epithelial ovarian tumor cells and also highly expressed in serous ovarian adenocarcinoma and increases with tumor progression. Clinical studies have found that it has a relatively low tumor specificity and sensitivity in the early diagnosis of epithelial ovarian cancer.Citation19 The expression of CA125 is abnormal in ovarian cyst, uterine fibroids, endometriosis, and other benign gynecological diseases; therefore, the collaborative use of CA125 and other tumor markers in clinic is aimed to improve the diagnostic sensitivity and specificity.Citation20,Citation21
CA19-9, a low carbohydrate antigen, is a screening tool for digestive tract tumors, especially pancreatic cancer and colorectal cancer. CA19-9 has shown a good diagnostic value in ovarian pulp, ovarian serous, and mucinous adenocarcinoma.Citation22 CEA is a classic broad-spectrum tumor marker mainly used in the diagnosis of digestive tract cancer and lung cancer. CEA levels are elevated in some patients with ovarian cancer.Citation23
In view of the limitations of using single serum tumor markers in the diagnosis of malignant tumors, a variety of tumor markers have been combined to reduce the rate of misdiagnosis and to improve the diagnostic efficiency. The present study analyzed the levels of HE4, CA125, CA19-9, and CEA in the serum of 458 patients with ovarian tumors. The results showed that the expression levels of HE4, CA125, CA19-9, and CEA in the serum of patients with ovarian cancer were significantly higher than those in patients with benign ovarian tumors.
Further analysis demonstrated that the sensitivity and specificity of the four tumor markers differed from each other for ovarian tumor diagnosis. The sensitivity and specificity of HE4 were 63.78% and 96.56%, respectively. The sensitivity and specificity of CA125 in turn were 62.75% and 70.61%, respectively. The sensitivity and specificity of CA19-9 were 35.71% and 79.01%, respectively. The sensitivity and specificity of CEA were 38.78% and 88.5%, respectively.
In our previous study, we analyzed serum HE4 and CA125 in combination with ROMA in 63 patients with malignant pelvic tumors and found that HE4 had a higher diagnostic value for ovarian cancer than CA125.Citation9 The present study included 196 patients with ovarian cancer and revealed a satisfactory specificity of HE4 in the diagnosis of ovarian cancer. The overall specificity of HE4 (96.56%) in the diagnosis of ovarian cancer was significantly higher than that of CA125 (70.61%). ROMA demonstrated a sensitivity of 81.12% and a specificity of 83.97%.
For the diagnosis of malignant ovarian tumors, the results showed that HE4 had the highest specificity, CA125 had high sensitivity, and CA19-9 and CEA had lower sensitivity. After various combined tests, we found that the combined use of two tumor markers had higher diagnostic sensitivity than single tumor marker. When HE4 and CA125 were combined, the specificity and sensitivity of the diagnosis were 80.1% and 69.08%, respectively. The diagnostic sensitivity increased to 88.52% and 90.82% when three or four tumor markers were used together. AUC showed that the combination of three or four tumor markers did not significantly improve the diagnostic efficacy when compared with the combination of HE4 and CA125.
Conclusion
HE4, CA125, CA19-9, and CEA are of great value in the differential diagnosis of benign and malignant ovarian tumors. HE4 has a satisfactory specificity in the diagnosis of ovarian cancer. There are nearly no clinical symptoms or signs at the early stage of most ovarian cancer patients. If one of the markers (the cutoff values were 140 pM for HE4, 35 U/mL for CA125, 27 U/mL for CA19-9, and 5 ng/mL for CEA) is found to be elevated in the patients with a pelvic mass, further examinations were recommended.
The combined use of the tumor markers has more advantages than single tumor marker in the screening and diagnosis of malignant ovarian tumors. Serum HE4 and CA125 in combination with ROMA can be used as an efficient tool to screen and diagnose clinical ovarian malignancies, and combined detection of serum HE4 and CA125 levels was advised for all female patients suspected of pelvic mass. However, the combined detection of three or four markers failed to improve the diagnostic efficacy when compared with the combination of HE4 and CA125.
Disclosure
The authors report no conflicts of interest in this work.
References
- TorreLABrayFSiegelRLFerlayJLortet-TieulentJJemalAGlobal cancer statistics, 2012CA Cancer J Clin20156528710825651787
- OberaignerWMinicozziPBielska-LasotaMEurocare Working GroupSurvival for ovarian cancer in Europe: the across-country variation did not shrink in the past decadeActa Oncol201251444145322313338
- SiegelRNaishadhamDJemalACancer statistics, 2013CA Cancer J Clin2013631113023335087
- PatsnerBYimGWPredictive value of preoperative serum CA-125 levels in patients with uterine cancer: the Asian experience 2000 to 2012Obstet Gynecol Sci201356528128824328017
- NicklinJJandaMGebskiVLACE Trial InvestigatorsThe utility of serum CA-125 in predicting extra-uterine disease in apparent early-stage endometrial cancerInt J Cancer2012131488589021918977
- DistlerMPilarskyEKerstingSGrützmannRPreoperative CEA and CA 19-9 are prognostic markers for survival after curative resection for ductal adenocarcinoma of the pancreas – a retrospective tumor marker prognostic studyInt J Surg201311101067107224161419
- MooreRGBrownAKMilleMCUtility of a novel serum tumor biomarker HE4 in patients with endometrioid adenocarcinoma of the uterusGynecol Oncol2008110219620118495222
- MooreRGBrownAKMillerMCThe use of multiple novel tumor biomarkers for the detection of ovarian carcinoma in patients with a pelvic massGynecol Oncol2008108240240818061248
- ShenJHuangYChenWThe diagnostic value of serum HE4 and Ca-125 and ROMA index in pelvic malignant tumorJ Fujian Med Univ201448395399
- KarlsenMASandhuNHegdallCEvaluation of HE4, CA125, risk of ovarian malignancy algorithm (ROMA) and risk of malignancy index (RMI) as diagnostic tools of epithelial ovarian cancer in patients with a pelvic massGynecol Oncol2012127237938322835718
- AroraVQuinnMAEndometrial cancerBest Pract Res Clin Obstet Gynaecol201226331132422277287
- LamerzRRole of tumour markers, cytogeneticsAnn Oncol199910Suppl 414514910436809
- FiorettiPGadducciAFerdeghiniMThe concomitant determination of different serum tumor markers in epithelial ovarian cancer: relevance for monitoring the response to chemotherapy and follow-up of patientsGynecol Oncol19924421551601544592
- ZhangZLYuYXuFCombining multiple serum tumor markers improves detection of stage I epithelial ovarian cancerGynecol Oncol2007107352653117920110
- SkatesSJHorickNYuYPreoperative sensitivity and specificity for early-stage ovarian cancer when combining cancer antigen CA125, CA15-3, CA72-4, and macrophage colony-stimulating factor using mixtures of multivariate normal distributionsJ Clin Oncol200422204059406615381683
- HellstromIRaycraftJHayden-LedbetterMThe HE4 (WFDC2) protein is a biomarker for ovarian carcinomaCancer Res200363133695337012839961
- ZanottiLBignottiECalzaSHuman epididymis protein 4 as a serum marker for diagnosis of endometrial carcinoma and prediction of clinical outcomeClin Chem Lab Med201250122189219823096757
- BignottiERagnoliMZanottiLDiagnostic and prognostic impact of serum HE4 detection in endometrial carcinoma patientsBr J Cancer201110491418142521468050
- MalkasianGDJrKnappRCLavinPTPreoperative evaluation of serum CA 125 levels in premenopausal and postmenopausal patients with pelvic masses: discrimination of benign from malignant diseaseAm J Obstet Gynecol198815923413462457318
- ZurawskiVRJrKnappRCEinhornNAn initial analysis of preoperative serum CA 125 levels in patients with early stage ovarian carcinomaGynecol Oncol19883017142452773
- EinhornNSjovallKKnappRCProspective evaluation of serum CA 125 levels for early detection of ovarian cancerObstet Gynecol199280114181603484
- ScaràSBottoniPScatenaRCA19-9: biochemical and clinical aspectsAdv Exp Med Biol201586724726026530370
- KimJYKimNKSohnSKPrognostic value of postoperative CEA clearance in rectal cancer patients with high preoperative CEA levelsAnn Surg Oncol200916102771277819657698