
Abstract
Background
The purpose of the present study was to examine the relationship among the number of negative lymph nodes (LNs), the local and systemic immune response, and survival in patients with colon cancer.
Patients and methods
One thousand one hundred and fifty-seven patients with colon cancer who underwent surgery at Sun Yat-sen University Cancer Center between 2009 and 2014 were included. We examined negative LNs in relation to the local and systemic immune response, including percentage carcinoma, neutrophil and lymphocyte infiltration, Crohn’s-like reaction, neutrophil to lymphocyte ratio, platelets, and C-reactive protein (CRP). Disease-free survival and overall survival were also examined. We performed subgroup analysis based on the distribution of negative LNs.
Results
An increased number of negative LNs was associated with greater neutrophil invasion (p=0.001), more lymphocyte invasion (p=0.001), and more Crohn’s-like reaction (p=0.001). No significant correlation was observed between negative LNs and the neutrophil to lymphocyte ratio. More than 12 negative LNs were associated with increased platelets and CRP levels. A higher number of negative LNs was independently associated with longer disease-free survival in stage I+II patients (p=0.004) and stage III patients (p=0.015), while negative LNs were also independent prognostic factors in stage IV patients (p=0.007).
Conclusion
Our study suggests that negative LNs are indicators of the immune response and are associated with a better prognosis in patients with colon cancer.
Introduction
Lymph node (LN) metastasis has important prognostic implications in patients with cancer.Citation1 Recently, the number of negative LNs has also attracted attention for its prognostic value. It has been reported that an increased number of negative LNs was associated with longer survival in breast cancer,Citation2,Citation3 lung cancer,Citation4 gastric cancer,Citation5,Citation6 esophageal cancer,Citation7 cervical cancer,Citation8 and colorectal cancer.Citation9–Citation12 The mechanism underlying the relationship between the number of negative LNs and the patient survival remains elusive. One possible reason is that increased numbers of negative LNs indicate accurate staging and higher care quality.Citation9 However, Zhuo et al reported that negative LNs are also prognostic factors in metastatic gastric cancer,Citation5 which cannot be explained by accurate staging or surgical intervention.
Another possible explanation for the prognostic value of negative LNs is that the increased negative LN number indicates higher tumor and host immune interaction. Until now, little evidence has been reported to support this hypothesis.Citation12 Therefore, we performed this study to evaluate the relationship between negative LNs and the host immune response, including both the local and the systemic tumor environment. We also studied the prognostic value of negative LNs in patients with colon cancer. Moreover, we performed subgroup analysis based on tumor stage in order to minimize its impact on our assessment of patients’ survival.
Patients and methods
Patient selection
The data set of Sun Yat-sen University Cancer Center was built prospectively. The records were retrospectively analyzed. Patients who met the following criteria were enrolled: 1) diagnosed with colon cancer between 2009 and 2014; 2) underwent primary tumor resection; 3) available records of routine blood tests before any treatment; 4) available paraffin-embedded tissue blocks; and 5) available follow-up information. The exclusion criteria were patients with infection, hyperpyrexia, hematological disease, enterobrosis, or intestinal obstruction at the time of first diagnosis. Written informed consent was obtained from all patients. The study was approved by the ethics review board in Sun Yat-sen University Cancer Center (GZR2015-034).
Measurement of neutrophil, lymphocytes, platelets (PLT), CRP, and carcinoembryonic antigen (CEA)
Neutrophil, lymphocytes, and PLT were measured using routine blood tests. These tests were conducted using the Sysmex XE-5000™ Automated Hematology System (Shanghai, People’s Republic of China). CRP was measured using the Hitachi Ltd. Automatic Analyzer 7600-020 (Tokyo, Japan). CEA was evaluated using electrochemiluminescence with the Hoffman-La Roche Ltd. Elecsys 2010 Chemistry Analyzer (Basel, Switzerland). The neutrophil to lymphocyte ratio (NLR) was categorized into two groups (>3 and ≤3).
Assessment of mismatch repair (MMR) status
Immunohistochemistry for the four most common MMR proteins was performed with the standard Envision (Dako Denmark A/S, Glostrup, Denmark) two-step procedure. The slides were dried overnight at 37°C, dewaxed in xylene, rehydrated through graded alcohol, and immersed in 3% hydrogen peroxide for 20 minutes to block endogenous peroxidase activities. They were then pretreated in antigen retrieval buffer (EDTA buffer, pH 8.0, 100°C, 2 minutes in a pressure cooker), and incubated with 10% normal goat serum at room temperature for 10 minutes to reduce nonspecific binding. Subsequently, the slides were incubated overnight at 4°C using the following antibodies: MLH1 (1:50; Beijing Zhong Shan Golden Bridge Biological Technology, Beijing, People’s Republic of China), PMS2 (1:50; Beijing Zhong Shan Golden Bridge Biological Technology), MSH2 (1:50; Beijing Zhong Shan Golden Bridge Biological Technology), and MSH6 (1:50; Beijing Zhong Shan Golden Bridge Biological Technology). After rinsing five times with 0.01 mol/L PBS (pH=7.4) for 10 minutes, detection of the primary antibody was performed using a secondary antibody (Envision) for 1 hour at room temperature and stained with diaminobenzidine (DAB) after washing in PBS again. Finally, the sections were counterstained with Mayer’s hematoxylin, dehydrated and mounted. PBS was used instead of the primary antibody in the negative control. Nonneoplastic colonic mucosa, stromal cells, and infiltrating lymphocytes or the centers of lymphoid follicles were used as internal positive controls. Known MMR-deficient (dMMR) colon carcinomas served as external negative controls. Two experienced pathologists evaluated the staining results independently and without any prior knowledge of the patients’ clinical data. Normal expression was defined as nuclear staining within tumor cells, whereas negative protein expression was defined as the complete absence of nuclear staining within tumor cells with concurrent internal positive controls. Tumors with the loss of MLH1/PMS2/MSH2/MSH6 proteins, as visualized using light microscopy, were classified as MLH1/PMS2/MSH2/MSH6 negative. If internal nonneoplastic tissues showed invalid negative staining, the procedure was repeated. When the opinions of the two pathologists were different, an agreement was reached by careful discussion.
Assessment of local tumor microenvironment
The carcinoma percentage, neutrophil infiltration (both in the central region and at the invasive margin), lymphocyte infiltration (both central region and invasive margin), and Crohn’s-like reaction were assessed as previously reportedCitation13–Citation15 by two pathologists who were blinded to the clinical data. Inflammatory cell reactions (neutrophil and lymphocytes) were estimated in H&E-stained sections by studying the central areas of the tumor and at the invasive margin. Four to six sections were routinely evaluated per tumor. We evaluated all of the sections and those with the most invasive part of the primary tumor were chosen to avoid bias. Dr Wan-Ming Hu and Dr Hui-Zhong Zhang assessed these markers. When the opinions of the two pathologists were different, agreement was reached by careful discussion.
Patient follow-up and statistical analysis
Disease-free survival (DFS), defined as the time from diagnosis to the time of the first event (loco-regional recurrence, metastasis, or death), and overall survival (OS), defined as the time from diagnosis to the date of death or the date of last follow-up, were examined in this study. The date of last follow-up was December 31, 2016.
All statistical analyses were performed using SPSS version 22. Frequencies and descriptive statistics were used to compare patient characteristics. Chi-square test was used to detect difference. Survival curves were calculated with the Kaplan–Meier method, and the differences were compared using the log-rank test. Multivariate analysis using a Cox proportional hazards model was used to test independent significance by backward elimination of insignificant explanatory variables. A p-value of <0.05 was considered significant.
Results
Patient characteristics
Seven hundred and thirteen men and 444 women were included. The median age was 59 (range from 19 to 87) years. Four hundred and thirty-five (37.6%) patients had right-sided colon cancer, and 703 (60.8%) had left-sided colon cancer. One hundred and six patients (9.2%) had stage I disease, 504 (43.6%) had stage II, 264 (22.8%) had stage III, and 283 (24.4%) had stage IV. The mean total LN counts was 15.9. The mean negative LN counts was 14.5. The distributions of clinicopathological features and their relationship with negative LNs are shown in . Increased negative LNs were associated with right-sided colon cancer (p=0.001), well or moderately differentiated disease (p=0.005), a lower CEA level (p=0.001), dMMR status (p=0.005), less neural invasion (p=0.001), and venous invasion (p<0.001).
Table 1 Correlations between the number of negative lymph nodes and patients’ characteristics
Negative LNs, the local tumor environment, and systemic inflammatory response
The relationship between negative LNs, the local tumor microenvironment, and the systemic inflammatory response is shown in . An increased number of negative LNs was associated with greater neutrophil invasion (p=0.001), higher-grade lymphocyte invasion (p=0.001), and more Crohn’s-like reactions (p=0.001). For the systemic inflammatory response, no significant correlation was observed between negative LNs and the NLR. More than 12 negative LNs were associated with increased PLT and CRP levels.
Table 2 Correlation between mismatch repair status, the local tumor microenvironment, and the systemic inflammatory response
Impact of negative LNs on recurrence and survival
Since only 106 patients had stage I disease, we grouped them together with the 504 patients with stage II disease. Among the patients with stage I and stage II disease, 58 experienced recurrence or distant metastasis during the follow-up time. Seven of 35 (20.0%) patients with 0–3 negative LNs, 7/50 (14.0%) patients with 4–6 negative LNs, 20/167 (12.0%) patients with 7–12 negative LNs, and 24/358 (6.7%) patients with ≥13 negative LNs experienced recurrence or distant metastasis. As shown in , an increased number of negative LNs was associated with longer DFS (p=0.036). In multivariable analyses, the impact of negative LNs (p=0.004) was independent of age, sex, primary tumor location, T stage, differentiation, venous invasion, neural invasion, MMR status, neutrophil infiltration, lymphocyte infiltration, CEA level, CRP level, and the NLR (Table S1). Among patients with stage III disease, 6/14 (42.9%) patients with 0–3 negative LNs, 17/36 (47.2%) patients with 4–6 negative LNs, 22/85 (25.9%) patients with 7–12 negative LNs, and 21/129 (16.3%) patients with ≥13 negative LNs experienced recurrence or distant metastasis. As shown in , an increased number of negative LNs was a predictor of longer DFS (p<0.001). In multivariable analyses, the impact of negative LNs (p=0.015) was also independent of age, primary tumor location, T stage, differentiation, venous invasion, neural invasion, MMR status, neutrophil infiltration, lymphocyte infiltration, CEA level, CRP level, and the NLR (Table S2).
Figure 1 Disease-free survival.
Notes: Disease-free survival of patients with stage I+II colon cancer (A) and stage III colon cancer (B) grouped by negative lymph nodes (LNs); overall survival of patients with stage IV colon cancer (C) grouped by negative LNs.
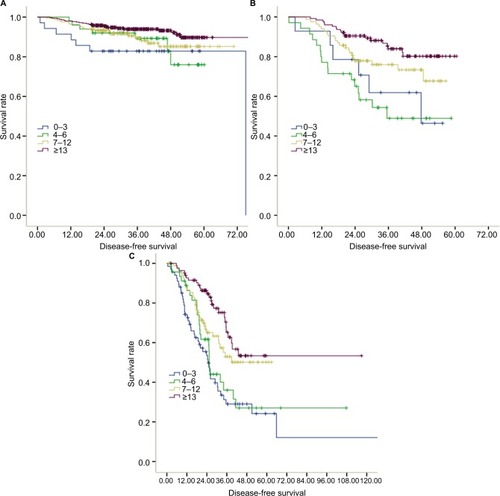
For patients with stage IV disease, the median OS was 19.8 months for those with 0–3 negative LNs, 23.2 months for those with 4–6 negative LNs, 23.2 months for those with 7–12 negative LNs, and 27.1 months for those with ≥13 negative LNs. Similarly, an increased number of negative LNs was associated with longer OS (p<0.001). In multivariable analyses, the impact of negative LNs (p=0.007) was an independent factor for OS (Table S3).
Subgroup analysis by location of LN
Previous studies reported that the location of positive LNs has an important prognostic value.Citation16 However, the impact of the distribution of negative LNs has not been fully studied. Thus, we performed subgroup analysis by grouping LNs into pericolic nodes, intermediate nodes, and nodes at the origin of the inferior mesenteric artery. Associations were observed between negative LNs and the inflammatory response, even when the distribution of negative LNs was taken into account (Tables S4–S9). However, no association was observed between age and the number of negative pericolic nodes (p=0.351) nor was any association observed between the NLR and the number of negative intermediate nodes (p=0.196). We found that the number of negative pericolic nodes had no prognostic value, whereas an increased number of negative intermediate nodes were associated with better survival in patients with all stages of colon cancer (Figure S1). Increased numbers of negative nodes at the origin of the inferior mesenteric artery were only associated with longer survival in patients with stage IV colon cancer (p=0.006, Figure S1).
Discussion
Negative LNs have been reported as prognostic factors in colon cancer, gastric cancer, breast cancer, esophageal cancer, and cervical cancer.Citation2–Citation4,Citation6–Citation9,Citation11,Citation12 In this study, we confirmed a significant correlation between the number of negative LNs and the survival of patients with colon cancer, even in metastatic colon cancer. The correlation was independent of tumor stage and other routine clinicopathological features. More importantly, we have provided clear evidence that an increased number of negative LNs was also an indicator of greater neutrophil and lymphocyte infiltration, both in the invasive margin and in the central region of tumor microenvironment. Negative LNs were also a predictor of a Crohn’s-like reaction in patients with colon cancer.
The mechanism underlying the relationship between the number of negative LNs and the survival remains unclear. Several hypotheses have been proposed. One possible reason is that assessing the numbers of negative LNs helps to reduce the likelihood of misclassification of stage III disease as stage II.Citation9 Furthermore, increased numbers of negative LNs might be an indicator of better therapy, including both surgical treatment and pathological assessment. However, the survival advantage associated with negative LNs in patients with metastatic colon cancer cannot be explained by these reasons.
An alternative explanation is that an increased number of negative LNs indicates a stronger immune reaction to the tumor, which is a well-known predictor of a better prognosis.Citation12 Once the immune system detects a tumor, the local LNs become enlarged in response. Enlarged LNs can be more easily detected surgically and pathologically. However, little evidence to date has supported this hypothesis. By analyzing the tumor microenvironment, we found that negative LNs are correlated with local neutrophil and lymphocyte infiltration, which supports this hypothesis. Furthermore, patients with increased numbers of negative LNs are more likely to be young, have colon cancer on the right side, have a larger primary tumor, and have dMMR status. These characteristics are associated with a higher lymphocytic reaction to the tumor. A better understanding of this interaction would lead to improved risk stratification and therapeutic intervention.
Recently, the concept of negative LNs has attracted increased attention in various types of cancer.Citation17–Citation19 Ahmadi et al observed that LN yield and negative LNs were influenced by patient age, site of disease, and T stage in patients with colorectal cancer.Citation20 By analyzing 1,167 patients with colorectal cancer, Tsai et al found that age, tumor size, and higher T stage were independent factors affecting the examinations of LN.Citation21 Zhang et al reported a higher predicted accuracy of survival through the incorporation of negative LN into American Joint Committee on Cancer stages.Citation22 Others presumed the immune response and the node count are interrelated, since antitumor immune response may lead to the enlargement of LNs and facilitate detection.Citation23 Those studies, together with our finding, highlight the importance of negative LNs in patients with colorectal cancer.
Guinney et al classified most colon cancers into four consensus molecular subtypes (CMSs).Citation24,Citation25 The CMS1 group, including most dMMR colon cancers, is characterized by right-sided lesions, a higher histopathological grade, enrichment of BRAF mutations and strong immune cell infiltration, particularly T lymphocytes.Citation24 Notably, patients with ≥13 negative LNs also have these characteristics. Ogino et al also observed a positive correlation between BRAF mutations and increased numbers of negative LNs.Citation12 Although we did not classify patients into different CMS types, it is possible that patients with CMS1 colon cancer have more negative LNs, indicating that immune classification is associated with tumor molecular subtypes.
Li et al reported that the negative to positive LN ratio was a superior prognostic factor in patients with stage III colorectal cancer.Citation10 In this study, we did not evaluate the ratio since it was also influenced by the number of positive LNs. Our study suggests that LNs could provide more prognostic information besides N stage and require more attention in clinical practice.
This study has several limitations. First, it is a retrospective study in a single institute; thus, the results should be interpreted with caution. Second, we determined the MMR status using only immunohistochemistry, and we did not use PCR. Data regarding several important molecular features, including RAS and BRAF mutations, were also absent since these factors are not routinely tested in our institute. Third, only DFS was analyzed in patients with stages I, II, and III disease since OS had not been reached yet. Fourth, due to the retrospective nature of this study, we do not know the name of the Dr who harvested the LNs. The size of mesentery was also unavailable. Those factors could lead to bias in our data.
In conclusion, our study suggests that negative LNs are indicators of immune response and are associated with a better prognosis in patients with colon cancer.
Availability of data
The data of the study were deposited in the Research Data Deposit system of Sun Yat-sen University Cancer (RDDA2018000547).
Acknowledgments
This work was supported by grants from the Natural Science Foundation of Guangdong, China (2015A030313010), Science and Technology Program of Guangzhou, China (1563000305), and National Natural Science Foundation of China (81272641 and 81572409). We have engaged the services of Editage [www.editage.cn], an English language editing service, to improve the language of the revised manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- BaxterNNVirnigDJRothenbergerDALymph node evaluation in colorectal cancer patients: a population-based studyJ Natl Cancer Inst200597321922515687365
- WuSGWangYZhouJNumber of negative lymph nodes should be considered for incorporation into staging for breast cancerAm J Cancer Res20155284485325973321
- WangQXCaiYFChenYYAdditional prognostic value of lymph node ratio (LNR) and number of negative lymph nodes (NLNs) in Chinese patients with triple negative breast cancerAnn Clin Lab Sci2017471687528249920
- LeDTDurhamJNSmithKNMismatch repair deficiency predicts response of solid tumors to PD-1 blockadeScience2017357634940941328596308
- ZhuoCYingMLinRWuXGuanSYangCNegative lymph node count is a significant prognostic factor in patient with stage IV gastric cancer after palliative gastrectomyOncotarget2017841711977120529050356
- LiXZhangWZhangXThe prognostic value of negative lymph node count for patients with gastric cancer who received preoperative radiotherapyOncotarget2017829469464695428159939
- ZhuZChenHYuWNumber of negative lymph nodes is associated with survival in thoracic esophageal squamous cell carcinoma patients undergoing three-field lymphadenectomyAnn Surg Oncol20142192857286324740827
- ChenYZhangLTianJRenXHaoQCombining the negative lymph nodes count with the ratio of positive and removed lymph nodes can better predict the postoperative survival in cervical cancer patientsCancer Cell Int2013131623374254
- JohnsonPMPorterGARicciardiRBaxterNNIncreasing negative lymph node count is independently associated with improved long-term survival in stage IIIB and IIIC colon cancerJ Clin Oncol200624223570357516877723
- LiQLiangLJiaHNegative to positive lymph node ratio is a superior predictor than traditional lymph node status in stage III colorectal cancerOncotarget2016744722907229927474167
- LiXLuHXuKNegative lymph node count is an independent prognostic factor for patients with rectal cancer who received preoperative radiotherapyBMC Cancer201717122728351352
- OginoSNoshoKIraharaNNegative lymph node count is associated with survival of colorectal cancer patients, independent of tumoral molecular alterations and lymphocytic reactionAm J Gastroenterol2010105242043319809407
- KlintrupKMakinenJMKauppilaSInflammation and prognosis in colorectal cancerEur J Cancer200541172645265416239109
- MeskerWEJunggeburtJMSzuhaiKThe carcinoma-stromal ratio of colon carcinoma is an independent factor for survival compared to lymph node status and tumor stageCell Oncol200729538739817726261
- ParkJHPowellAGRoxburghCSMismatch repair status in patients with primary operable colorectal cancer: associations with the local and systemic tumour environmentBr J Cancer2016114556257026859693
- HuhJWKimYJKimHRDistribution of lymph node metastases is an independent predictor of survival for sigmoid colon and rectal cancerAnn Surg20122551707822133895
- OginoSGalonJFuchsCSDranoffGCancer immunology–analysis of host and tumor factors for personalized medicineNat Rev Clin Oncol201181271171921826083
- AkagiYAdachiYKinugasaTLymph node evaluation and survival in colorectal cancer: review of population-based, prospective studiesAnticancer Res20133372839284723780968
- GleisnerALMogalHDodsonRNodal status, number of lymph nodes examined, and lymph node ratio: what defines prognosis after resection of colon adenocarcinoma?J Am Coll Surg201321761090110024045143
- AhmadiOStringerMDBlackMAMcCallJLClinico-pathological factors influencing lymph node yield in colorectal cancer and impact on survival: analysis of New Zealand Cancer Registry dataJ Surg Oncol2015111445145825663298
- TsaiHLHuangCWYehYSFactors affecting number of lymph nodes harvested and the impact of examining a minimum of 12 lymph nodes in stage I-III colorectal cancer patients: a retrospective single institution cohort study of 1167 consecutive patientsBMC Surg2016161727079509
- ZhangZYGaoWLuoQFA nomogram improves AJCC stages for colorectal cancers by introducing CEA, modified lymph node ratio and negative lymph node countSci Rep201663902827941905
- GeorgeSPrimroseJTalbotRWill Rogers revisited: prospective observational study of survival of 3592 patients with colorectal cancer according to number of nodes examined by pathologistsBr J Cancer200695784184716969342
- GuinneyJDienstmannRWangXThe consensus molecular subtypes of colorectal cancerNat Med201521111350135626457759
- DienstmannRVermeulenLGuinneyJConsensus molecular subtypes and the evolution of precision medicine in colorectal cancerNat Rev Cancer2017172799228050011