
Abstract
Purpose
To report the clinical features, imaging manifestations, histopathology, and immunohistochemical features of several cases of orbital solitary fibrous tumors (SFTs) in a Chinese tertiary hospital, and to undertake a literature review of this rare disease.
Methods
A non-comparative retrospective review of clinical presentations, imaging manifestations, histopathology, and immunohistochemical features as well as the management and disease outcomes of patients with orbital SFT was conducted along with a review of orbital SFT cases in the literature.
Results
This study includes two male and two female patients, with an average age of 53 years. Common presentations among these patients included a palpable subcutaneous mass, swelling of the eyelid, proptosis, diplopia, and vision disturbance. Three patients (cases 2–4) underwent imaging scans. All patients had complete surgical excisions and the tissue was subjected to pathological analysis. One patient (Case 4) experienced a recurrence with malignant transformation and received a re-excision surgery and postoperative radiotherapy. All patients remain alive and well after a minimum follow-up of 12 months (range 12–34 months).
Conclusion
Despite its rare occurrence, we suggest that the possibility of orbital SFTs needs to be considered when a painless, slowly growing orbital mass is identified. Typical characteristic magnetic resonance imaging features of orbital SFTs are iso- or hypointense signals on T1 and T2-weighted images, with marked enhancement. A positive cluster of differentiation 34 (CD34) staining is an important diagnostic clue favoring SFT. Some orbital SFTs are infiltrating, aggressive, or recur with malignant transformation. Therefore, regular long-term follow-up after complete excision is mandatory.
Keywords:
Introduction
The solitary fibrous tumor (SFT) is a rare spindle cell tumor originating from the mesenchyme and was first described in pleural tissue in 1931.Citation1 A recent study has reported that SFT is found in extrapleural locations such as lung, liver, pericardium, peritoneum, mediastinum, nasal cavities, thyroid, parotid gland, and the orbit.Citation2 SFT in the orbit is extremely rare. Since the first report of an orbital SFT in 1994,Citation3,Citation4 only 90 cases have been described in the English literature to date.Citation5–Citation15 Most orbital SFTs are described as isolated case reports. Herein, we present four orbital SFT cases and conduct a review of the literature discussing the presentation, imaging, histopathology, management, and outcomes of this rare disease.
Methods
Clinical data
A non-comparative retrospective review was conducted for patients presenting to our hospital with a pathological diagnosis of orbital SFT between 2014 and 2017. The study was approved by the Human Subjects Ethics Subcommittee of the First Affiliated Hospital of Zhejiang University, and it adhered to the tenets of the Declaration of Helsinki. Written informed consent for the publication of case details was obtained from all patients in our study. Simultaneously, a review of the literature was done using PubMed to search combinations of the terms “orbital solitary fibrous tumor.”
Histopathology and immunohistochemistry
Surgical samples were collected and embedded in paraffin for histological and immunohistochemical analyses. Immunohistochemical studies for cluster of differentiation 34 (CD34), cluster of differentiation 99 (CD99), B-cell lymphoma 2 (Bcl-2), smooth muscle actin (SMA), S-100 protein, Ki-67, cytokeratin (CK), Desmin, and cluster of differentiation 117 (CD117) were undertaken on paraffin sections in all samples. All antibodies were obtained from OriGene (Rockville, MD, USA).
Results
Case 1
A 37-year-old woman was referred to our department with a complaint of swelling in the right lower eyelid for 4 years. A focal, firm, nontender swelling with well-defined margins was palpated in the inferomedial side of her right orbit.
The mass was completely excised via a subciliary approach. Gross examination of the surgical specimen disclosed a well-encapsulated 25×20 mm oval mass. On histopathological study, the tumor was composed of haphazardly arranged spindle cells with bland nuclei and inconspicuous nucleoli (). Immunohistochemical analysis showed that the tumor cells exhibited diffuse immunoreactivity for CD34 and CD99 and was approximately 5% positive for Ki-67 (). These observations were consistent with the diagnosis of SFT.
Table 1 Summary of the histological features of orbital SFT in the present series
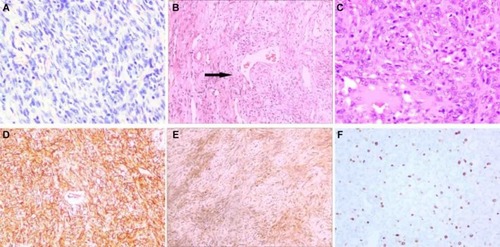
Figure 1 Histopathological and immunohistochemical staining of tumors in our cases.
Notes: (A) The tumor is composed of haphazardly arranged spindle cells with bland nuclei and inconspicuous nucleoli. (Case 1; HE staining; original magnification: ×200). (B) Variably collagenous and numerous endothelium-lined vascular channels are noted. (Case 2; arrow shows an occasional vascular channel with a staghorn appearance; HE staining; original magnification: ×200). (C) Tumor cells with oval nuclei, conspicuous nucleoli, and mitotic figure are noted. (recurrent sample of Case 4; HE staining; original magnification: ×200). (D) Tumor cells are positive for CD34. (recurrent sample of Case 4; original magnification: ×200). (E) The tumor cells are positive for Bcl-2 (Case 2; original magnification: ×200). (F) The tumor cells are positive for Ki-67 (>10%), which indicates malignant transformation (recurrent sample of Case 4; original magnification: ×200).
Abbreviations: HE, hematoxylin and eosin; CD34, cluster of differentiation 34; Bcl-2, B-cell lymphoma 2.
This patient is still alive and well, without local relapse after 27 months.
Case 2
A 51-year-old man came to our department with a palpable subcutaneous mass in the right lacrimal sac area which was first noticed 6 months earlier. Findings on ophthalmic examination were normal, except for a movable mass without tenderness.
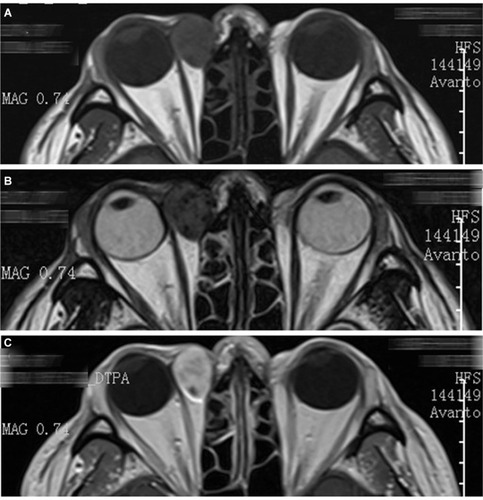
Orbital magnetic resonance (MR) imaging showed an approximately 20×15 mm, well-circumscribed circular tumor in the subcutaneous region of the right lacrimal sac area, presenting with slight low signal intensity on T1 and T2 images, heterogeneous intermediate signal intensity on fat-suppression images, and diffusely heterogeneous enhancement after intravenous gadolinium administration ().
Figure 2 MR scan of Case 2 shows a well-circumscribed circular mass in the subcutaneous region of the right lacrimal sac area.
Notes: (A) T1 image, (B) T2 image, and (C) post-contrast T1 image.
Abbreviation: MR, magnetic resonance.
The mass was completely removed via a medial canthus split approach. Histopathologically, the tumor was composed of spindle cells and the stroma was variably collagenous. The tumor showed numerous endothelium-lined vascular channels, some of which showed an occasional staghorn appearance (). Immunohistological study showed positivity for CD34 and Bcl-2, and weak positivity for Ki-67 (<5%; and ). These findings support the diagnosis of SFT.
This patient is alive and has kept well for 34 months.
Case 3
A 65-year-old woman was referred to our department, and presented with a 1-year history of a painless, palpable nasal mass in the left orbit. A 20×15 mm, well-circumscribed mass was palpated in the nasal region of the left upper lid, and the rest of the ophthalmic examination was unremarkable.
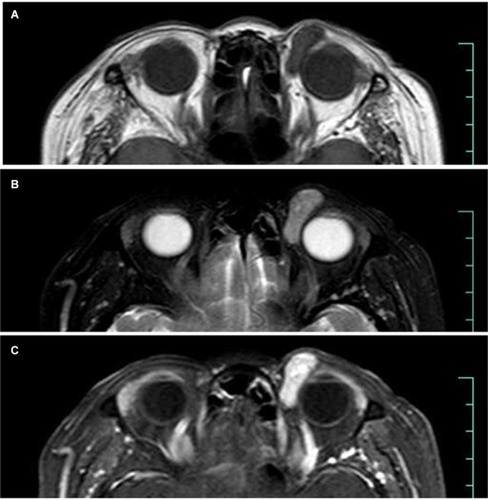
Orbital MR imaging revealed a well-circumscribed, 20×15 mm subcutaneous mass in the superomedial side of her left orbit, with homogeneous isointense signals on T1 images and hypointense signals on T2 images. The lesion showed strong gadolinium enhancement ().
Figure 3 MR scan of Case 3 shows a well-circumscribed subcutaneous mass in the superomedial side of her left orbit with homogeneous isointense signal on T1 images and hypointense signal on T2 images.
Notes: (A) T1 image, (B) T2 image, and (C) post-contrast T1 image.
Complete removal of the lesion was undertaken via an upper eyelid medial split approach. The mass was approximately 22×17×15 mm in size. Histopathological examination revealed the tumor was composed of uniform spindle cells containing fusiform nuclei, indistinct nucleoli, and a pale eosinophilic cytoplasm in a collagenous matrix. Small- to medium-sized endothelium-lined vascular channels were diffusely scattered. Moreover, immunohistochemistry showed strong positivity for CD34 staining and weak positivity for Ki-67 staining (<5%), consistent with a diagnosis of SFT ().
The patient is alive and healthy, without local relapse for at least 26 months.
Case 4
A 60-year-old man was referred to our department with complaints of proptosis and diplopia in his left eye for 2 months. He had a history of hepatocellular carcinoma and had undergone a transcatheter arterial chemoembolization operation 2 years before this presentation.
Ophthalmic examination showed an 8-mm proptosis, diffuse conjunctival congestion, and chemosis of his left eye as well as limitation of extraocular movement in all gazes. The visual acuity of the left eye had decreased to 1/20, and could not be corrected. A fundus examination showed papilloedema and venous congestion.
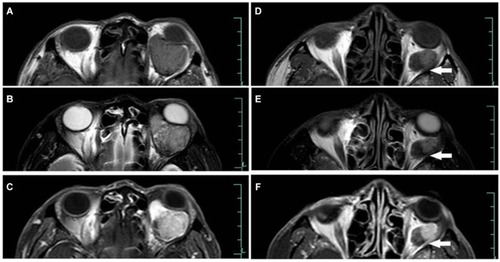
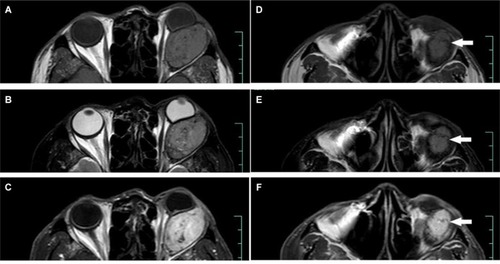
The orbital MR showed a giant, well-circumscribed mass in the muscle cone of the left orbit that could not be separated from the optic nerve and pushed the optic nerve to the nasal side. The lesion had two types of imaging features on MR. One presented with low signal intensity on T1 and T2 images, and the other presented with isointense signal intensity on T1 and T2 images. The latter presented a diffusely heterogeneous enhancement after intravenous administration of gadolinium ().
Figure 4 The MR scan of Case 4 (1st op). Arrows show the lesion had two types of imaging features on MRI. The medial part of the mass indicates a tissue with high collagen content whereas the lateral part indicates a tissue with hypervascular content.
Notes: (A, D) T1 image, (B, E) T2 image, and (C, F) post-contrast T1 image.
Abbreviation: op, operation.
The tumor was removed by lateral orbitotomy. A part of the mass was grayish white with a size of 18×15×15 mm, whereas the rest of the mass was wine-red with a size of 3.0×2.5×2.5 mm. Histopathological study revealed haphazardly arranged spindle cells with dense collagenous fibrosis. No mitoses or areas of necrosis were identified. The tumor contained numerous blood vessels, ranging from capillary to medium-sized vessels. Immunohistochemistry showed strong positivity for CD34 staining and weak positivity for Ki-67 staining (<5%), which confirmed our diagnosis of SFT ().
The mass recurred 14 months after the operation. Orbital MR imaging revealed a well-circumscribed 37×34×23 mm mass in the muscle cone of the left orbit with isointense signal intensity on T1 images, and isointense to slight hyperintense signal intensity on T2 images. A post-contrast T1-weighted image revealed a heterogeneous enhancement of the lesion ().
Figure 5 MR scan of Case 4 (2nd operation). Arrows show signal tubular structures, which might represent fast-flow vessels within the tumor.
Notes: (A, D) T1 image, (B, E) T2 image, and (C, F) post-contrast T1 image.
An extensive resection was done. Preoperatively, the recurrent mass was identified in the muscle cone and was found to be adherent to the optic nerve. Gross examination revealed the tumor was grayish white with a size of 35×30×25 mm. Histopathologically, the tumor was composed of spindle cells, a section of which had oval nuclei and conspicuous nucleoli. Mitotic figures were noted, with a transition into a high-grade component (). Moreover, these tumor cells showed strong and diffuse positivity for CD34 staining and >10% cells were positive on Ki-67 staining, suggesting malignant degeneration of the tumor ( and ).
The patient was referred to the department of radiation oncology for radiotherapy. There was no evidence of recurrence during a 12-month follow-up period.
Discussion
The SFT, first identified by Klemperer and Rabin in 1931, is a rare tumor which is described as a mesenchymal neoplasm originating in the pleural structures.Citation1 Subsequently, it has also been reported in extrapleural locations, such as the upper airway tract, nasal and paranasal sinuses, parotid and salivary glands, thyroid, lung, mediastinum, pericardium, peritoneum, liver, spine, soft tissues, and orbit.Citation16–Citation21 An orbital SFT was first described by Westra et al and Dorfman et al in 1994Citation3,Citation4 and, since then, approximately 90 cases have been reported in ophthalmologic and pathologic journals.Citation5–Citation15
Clinical features
Orbital SFT has been documented across a wide age range from 9 to 76 years, predominating in the fifth decade, with no sex predilection according to previous reports.Citation22–Citation25 In this study, the four cases described include two men and two women, with a mean age of 53 (range 37–65 years), which was consistent with previous reports ().
Table 2 Summary of clinical features of orbital SFT in the present series
In a study reported by Romer et al, 25 cases were identified in the left orbit and 14 in the right orbit.Citation26 In our study, two cases were found in the right orbit and two in the left ().
According to the reviews from Le et al, orbital SFTs may occur in a variety of areas in the orbital space: 20% in the superomedial orbital quadrant, 15% in the medial orbit, 13% in the superotemporal area, 9.5% in the lacrimal area, and 7% in the inferotemporal area.Citation5 In our study, the tumor in Case 1 was in the lower eyelid, and in the lacrimal sac area in Case 2. Tumors in cases 3 and 4 were located in the superomedial orbital quadrant and muscle cone, respectively.
Orbital SFT commonly presents as a slowly progressive, unilateral, painless proptosis and may be associated with eyelid swelling, vision disturbances, a palpable mass, tearing, and ptosis. In the present study, a palpable subcutaneous mass was the most frequent initial feature. Proptosis and vision disturbances were observed in Case 4 (). Orbital SFTs were less commonly associated with optic nerve dysfunction and extraocular muscle impairment depending on their size and location.Citation5
MR imaging presentation
On imaging, an orbital SFT presents as well-defined soft tissue masses with heterogeneously or homogeneously strong enhancement on computed tomography (CT) and MR images.Citation27 Furthermore, internal calcifications and necrosis have been reported occasionally.Citation16,Citation17 Compared with the cerebral cortex or extraocular muscle, the signal intensity of SFTs seen on MR images, in general, were isointense on T1-weighted images and isointense to hypointense on T2-weighted images. Sometimes, a hypointense signal intensity can be seen within the lesion on both T1- and T2-weighted images, reflecting fibrous tissue with high collagen content.Citation19,Citation23,Citation26,Citation28–Citation32 Moreover, a hyperintense signal can be observed within the lesion on T2-weighted images in some cases, causing signal intensity heterogeneity on T2-weighted images. These T2 hyperintense signals are related to internal hemorrhage, cystic degeneration, or relatively fresh fibrosis.Citation19,Citation32,Citation33 Variations of the signal intensity on MR images reflected the differences of cellular components, collagen, fibroblasts, and degenerative change contained within individual tumors.
Homogeneous or heterogeneously attenuated enhancement is reported to be the most prominent feature of SFT that is revealed with CT and MR imaging, which is attributed to the prominent vascular channels within the tumor.Citation19,Citation23,Citation31,Citation34–Citation37 Of the three lesions examined by MR in this study, one showed homogeneously marked enhancement (Case 3), and the rest showed heterogeneously marked enhancement (Cases 2 and 4). On the MR scan of Case 4, signal-intensity tubular structures were noted on T1, T2, and post-contrast T1-weighted MR images, which might represent fast-flow vessels within the tumor ().
Histopathologic and immunohistochemical features
As clinical signs and radiological features are not distinctive, histological examination plays an important role in the diagnosis of orbital SFT. Tumors appeared as regular round masses, of hard consistency, and were homogeneously grayish white upon sectioning. All tumors in the present study were firm; neither cystic spaces nor necrosis were found. Tumors in cases 1, 2, and 3 were grayish white in color, whereas the mass in Case 4 was wine-red. Histological study revealed alternating cellular and hypocellular areas with spindle-shaped cells presenting an ovoid and irregular nucleus, inconspicuous nucleoli, and a scant, undefined eosinophilic cytoplasm.Citation38 Spindle-shaped cells grow in a haphazard manner in a variable cellular stroma, which is described as a “patternless pattern” or keloid-like hyalinization. The tumor showed thick bands of collagen interspersed between the tumor cells, branching thin-walled vessels of varying caliber, and a “staghorn” vascular pattern, similar to a hemangiopericytoma (HPC). These features are consistent with those observed in our cases.
Microscopic features alone are insufficient to validate SFT. The key to identify SFT is to conduct immunohistological analysis.Citation25,Citation39 Strong and consistent positivity of CD34 is an important diagnostic marker of SFT, which demonstrates strong CD34 reactivity in 90–100% of cases,Citation2,Citation3 and the expression of CD34 may be lost in tumors that undergo malignant transformation.Citation40 Meanwhile, SFT has been documented to exhibit strong and diffuse positivity with vimentin, CD99, and Bcl-2.Citation38 Epithelial membrane antigen (EMA) and SMA might occasionally be detected, whereas SFT is usually negative for S-100 and CK.Citation41
Due to its histological similarities to other spindle-shaped cell tumors, SFT has been confused histologically with other lesions, such as HPC, fibrous histiocytoma, schwannoma, and meningioma. HPC displays a mixture of spindle-shaped tumor cells with oval nuclei and a small cytoplasm mixed with a network of thin-walled blood vessels or sinusoid-like spaces. HPC cells show high reactivity to the CD34 antibody and vimentin, but lack immunoreactivity to EMA.Citation42 Fibrous histiocytoma usually consists of fibroblasts and prominent round histiocytic cells in a characteristic storiform pattern. Immunohistochemical staining consistently reveals that histiocytes are CD68 positive but are usually CD34 negative. Schwannomas display a characteristic morphology of alternating Antoni A and Antoni B areas and Verocay bodies. Immunohistochemical staining shows strong reactivity to neural markers such as S-100 protein, which is negative in a SFT.Citation23 Fibrous meningioma often shows characteristic psammoma bodies, which are absent in SFTs. Besides, compared to SFT, a fibrous meningioma is usually better stained by an EMA antibody, but only mildly or focally positive on CD34 and Bcl-2 staining.Citation43
Malignant transformation and aggressive behavior
Most orbital SFTs are described in isolated case reports; thus their clinical behavior is currently unknown. It is generally believed that SFTs behave in a benign fashion and follow a non-aggressive course.
A few of the orbital SFT cases reported have displayed malignant histological features, defined by hypercellularity, pleomorphism, increased tumor size (≥5 cm), mitotic counts >4 per 10 high-power fields, and necrosis.Citation29,Citation38,Citation44–Citation47 Immunohistochemically, the expression of CD34 may be lost in tumors that undergo malignant transformation in cases of orbital SFTs.Citation40,Citation45 However, these pathologic factors do not always correlate with the clinical behavior of the tumor. Our literature search reviewed that only two of the five documented malignant orbital SFTs cases exhibited aggressive behavior, one of which had a recurrence whereas the other one had a local invasion.Citation7,Citation25,Citation44,Citation48,Citation49 Some tumors with malignant histologic findings remained indolent, whereas other tumors with completely benign histologic findings behaved aggressively. The aggressive behavior of orbital SFTs is defined by a local invasion, recurrence, and distant metastases.Citation7,Citation29,Citation44,Citation46,Citation50–Citation54 Nineteen of the 21 recurrent orbital SFTs were histologically benign. Young and Hardy reported a histologically benign orbital SFT case that invaded intracranial tissues.Citation54
Malignant transformation of a recurrent SFT has been described in lung, pleura, and thigh SFT cases.Citation55–Citation57 A malignant variant of a recurrent orbital SFT has been reported only in four cases, to our knowledge (). The intervals of malignant evolution varied from 6 months to 9 years after initial tumor excision.Citation44,Citation58–Citation60 Here, we report the fifth case (Case 4) of a recurrent orbital SFT with malignant transformation, which showed progressive histological dedifferentiation. Two types of malignant transformation have been reported previously: one is malignant or high-grade transformation from benign, low-grade, or intermediate-grade SFT, and the other is de novo occurrence of a malignant SFT.Citation61 Malignant transformation of an SFT may have a worse consequence and need close follow-up.
Table 3 Summary of reported recurrent orbital SFT with malignant transformation
Treatment and prognosis
Orbital SFTs are so rare that most published cases were individual case reports without documented extended follow-up; therefore, it is difficult to predict the true clinical course of these tumors.
Radical surgical resection seemed to be the most important prognostic factor. The extent of resection might be the most predictive factor for recurrence. In Chen et al’s research, all four patients who underwent gross total removal did not have recurrence, whereas five of the six patients who had subtotal removal had a recurrence with a median recurrence time of 48 months.Citation62 However, there are many factors that could prevent total resection, such as location, size, blood loss, and adhesion. Therefore, resecting as much tumor content as possible should be the goal of the treatment. In Case 4, the patient had a recurrence and malignant transformation. Therefore, a complete re-excision of the tumor and postoperative radiation therapy were carried out. Postoperative radiotherapy can be used as an adjuvant therapy when the lesion is not completely removed or in recurrent and malignant cases. Although there has been no sign of recurrence during a 12-month follow-up in this case, the prognosis should be guarded, and long-term follow-up is warranted.
Conclusion
Orbital SFTs should be suspected when confronting painless, slow-growing orbital masses although it is a rare entity. High CD34 expression is an important diagnostic marker favoring SFT. Some orbital SFTs are infiltrating, aggressive, or recurrent with malignant transformation. We report the fifth case (Case 4) of a recurrent orbital SFT with malignant transformation. Further research with a larger patient pool and extended follow-up is necessary to verify the clinical outcome of these tumors.
Acknowledgments
The work was supported by the Medical Health and Technology Project of Zhejiang Province (grant no. 201796807). The funding organization had no role in the design or conduct of this research.
Disclosure
The authors report no conflicts of interest in this work.
References
- KlempererPRabinCBPrimary neoplasms of the pleura: a report of five casesArch Pathol1931113387414
- BrunnemannRBRoJYOrdonezNGMooneyJEl-NaggarAKAyalaAGExtrapleural solitary fibrous tumor: a clinicopathologic study of 24 casesMod Pathol199912111034104210574600
- WestraWHGeraldWLRosaiJSolitary fibrous tumor. Consistent CD34 immunoreactivity and occurrence in the orbitAm J Surg Pathol199418109929987522416
- DorfmanDMToKDickersinGRRosenbergAEPilchBZSolitary fibrous tumor of the orbitAm J Surg Pathol19941832812878116796
- LeCPJonesSValenzuelaAAOrbital solitary fibrous tumor: a case series with review of the literatureOrbit201433214515124295271
- HashemiNLingJDSoparkarCTransarterial Onyx embolization of an orbital solitary fibrous tumorOcul Oncol Pathol2015129810227171911
- TenekeciGSariAVayisogluYSerinOGiant solitary fibrous tumor of orbitJ Craniofac Surg2015265e390e39226102546
- GencAToktasZAzmanCBozkurtSUKilicTSolitary fibrous tumor of the orbit: a case report and review of the literatureTurk Neurosurg201525698498726617156
- GuptaSVermaRSenRSinghIMarwahNKohliRSolitary fibrous tumor of the orbitAsian J Neurosurg201611178
- TataACohen-InbarOSheehanJPTreatment of orbital solitary fibrous tumour with gamma knife radiosurgery and systematic review of literatureBMJ Case Rep20162016 bcr2016217114
- TanakaKYanoHHayashiHHiranoATotal resection combined with osteotomy is more effective for orbital solitary fibrous tumor excision: a report of three casesInt Ophthalmol201838134535128054210
- JungSKPaikJSParkGSYangSWCD34 + tumours of the orbit including solitary fibrous tumours: a six-case seriesBMC Ophthalmol20171715928449640
- AlamSBackiavathyVMukherjeeBSubramanianKA rare case of giant multicystic solitary fibrous tumor of the orbitOrbit2018371697228816553
- VuAFChunduryRVBlandfordADPerryJDRecurrent orbital solitary fibrous tumor in a 12-year-oldOcul Oncol Pathol201732838628868275
- KünzelJHainzMZiebartTHead and neck solitary fibrous tumors: a rare and challenging entityEur Arch Otorhinolaryngol201627361589159826026772
- GoodladJRFletcherCDSolitary fibrous tumour arising at unusual sites: analysis of a seriesHistopathology19911965155221786936
- SusterSNascimentoAGMiettinenMSickelJZMoranCASolitary fibrous tumors of soft tissue. A clinicopathologic and immunohistochemical study of 12 casesAm J Surg Pathol19951911125712667573687
- ChanJKSolitary fibrous tumour—everywhere, and a diagnosis in vogueHistopathology19973165685769447390
- GanlyIPatelSGStambukHESolitary fibrous tumors of the head and neck: a clinicopathologic and radiologic reviewArch Otolaryngol Head Neck Surg2006132551752516702568
- RayappaCSMcArthurPDGangopadhyayKAntoniusJISolitary fibrous tumour of the infratemporal fossaJ Laryngol Otol199611065945978763387
- SatoJAsakuraKYokoyamaYSatohMSolitary fibrous tumor of the parotid gland extending to the parapharyngeal spaceEur Arch Otorhinolaryngol1998255118219592669
- BernardiniFPde ConciliisCSchneiderSKerstenRCKulwinDRSolitary fibrous tumor of the orbit: is it rare? Report of a case series and review of the literatureOphthalmology200311071442144812867407
- KrishnakumarSSubramanianNMohanERMaheshLBiswasJRaoNASolitary fibrous tumor of the orbit: a clinicopathologic study of six cases with review of the literatureSurv Ophthalmol200348554455414499820
- LeonciniGMaioVPuccioniMOrbital solitary fibrous tumor: a case report and review of the literaturePathol Oncol Res200814221321718493869
- TamESChenECNijhawanNHarveyJTHowarthDOestreicherJHSolitary fibrous tumor of the orbit: a case seriesOrbit200827642643119085297
- RomerMBodeBSchuknechtBSchmidSHolzmannDSolitary fibrous tumor of the orbit–two cases and a review of the literatureEur Arch Otorhinolaryngol20052622818815316820
- KimHJKimHJKimYDSolitary fibrous tumor of the orbit: CT and MR imaging findingsAJNR Am J Neuroradiol200829585786218272558
- KimHYLeeSYKangSJKimHJSolitary fibrous tumor of the orbit: a poorly recognized orbital lesionActa Ophthalmol Scand199977670470810634569
- HayashiSKuriharaHHiratoJSasakiTSolitary fibrous tumor of the orbit with extraorbital extension: case reportNeurosurgery20014951241124511846919
- JohnsonTEOnofreyCBEhliesFJEchography as a useful adjunct in the diagnosis of orbital solitary fibrous tumorOphthal Plast Reconstr Surg20031916874
- KimTABrunbergJAPearsonJPRossDASolitary fibrous tumor of the paranasal sinuses: CT and MR appearanceAJNR Am J Neuroradiol1996179176717728896635
- DunfeeBLSakaiOSpiegelJHPisteyRSolitary fibrous tumor of the buccal spaceAJNR Am J Neuroradiol20052682114211616155167
- KimHJLeeHKSeoJJMR imaging of solitary fibrous tumors in the head and neckKorean J Radiol20056313614216145288
- MeyerDRileyFSolitary fibrous tumor of the orbit: a clinicopathologic entity that warrants both a heightened awareness and an atraumatic surgical removal techniqueOrbit2006251455016527776
- ShinJHSungIYSuhJHSolitary fibrous tumor in the buccal space: MR findings with pathologic correlationAJNR Am J Neuroradiol200122101890189211733322
- JeongAKLeeHKKimSYChoKJSolitary fibrous tumor of the parapharyngeal space: MR imaging findingsAJNR Am J Neuroradiol200223347347511901021
- TateishiUNishiharaHMorikawaTMiyasakaKSolitary fibrous tumor of the pleura: MR appearance and enhancement patternJ Comput Assist Tomogr200226217417911884769
- FurusatoEValenzuelaIAFanburg-SmithJCOrbital solitary fibrous tumor: encompassing terminology for hemangiopericytoma, giant cell angiofibroma, and fibrous histiocytoma of the orbit: reappraisal of 41 casesHum Pathol201142112012821056898
- MentzelTBainbridgeTCKatenkampDSolitary fibrous tumor: clinicopathologic, immunohistochemical, and ultrastructural analysis of 12 cases arising in soft tissues, nasal cavity and nasopharynx, urinary bladder and prostateVirchows Arch199743064454539230909
- KanthanRTorkianBRecurrent solitary fibrous tumor of the pleura with malignant transformationArch Pathol Lab Med2004128446046215043457
- SusterSFisherCMoranCAExpression of bcl-2 oncoprotein in benign and malignant spindle cell tumors of soft tissue, skin, serosal surfaces, and gastrointestinal tractAm J Surg Pathol19982278638729669348
- HsuCHWeiYHPengYLiaoSLOrbital hemangiopericytoma in an Asian populationJ Formos Med Assoc2014113635656324820631
- TihanTViglioneMRosenblumMKOliviABurgerPCSolitary fibrous tumors in the central nervous system. A clinicopathologic review of 18 cases and comparison to meningeal hemangiopericytomasArch Pathol Lab Med2003127443243912683870
- CarreraMPratJQuintanaMMalignant solitary fibrous tumour of the orbit: report of a case with 8 years follow-upEye (Lond)200115Pt 110210411318269
- GirnitaLSahlinSOrregoASeregardSMalignant solitary fibrous tumour of the orbitActa Ophthalmol200987446446718823286
- PolitoETosiGMTotiPSchürfeldKCaporossiAOrbital solitary fibrous tumor with aggressive behavior: three cases and review of the literatureGraefes Arch Clin Exp Ophthalmol2002240757057412136289
- WellingLCLynchJCFerreiraLASolitary fibrous tumor with intracranial invasionArq Neuropsiquiatr2009673A70170319722055
- SuzukiSA case of malignant solitary fibrous tumor presenting with exophthalmosJpn J Clin Oncol200737540117599948
- PatelMMJakobiecFAZakkaFRIntraorbital metastasis from solitary fibrous tumorOphthal Plast Reconstr Surg2013293e76e79
- WooKISuhYLKimYDSolitary fibrous tumor of the lacrimal sacOphthal Plast Reconstr Surg1999156450453
- AlexandrakisGJohnsonTERecurrent orbital solitary fibrous tumor in a 14-year-old girlAm J Ophthalmol2000130337337611020428
- GriepentrogGJHarrisGJZambranoEVMultiply recurrent solitary fibrous tumor of the orbit without malignant degeneration: a 45-year clinicopathologic case studyJAMA Ophthalmol2013131226526723411904
- ParrozzaniRFusettiSMontescoCFaveroVMidenaEBiphasic solitary fibrous tumor of the orbit with distant metastasesInt Ophthalmol201333670170523329333
- YoungTKHardyTGSolitary fibrous tumor of the orbit with intracranial involvementOphthal Plast Reconstr Surg2011273e74e76
- InoueTOwadaYWatanabeYRecurrent intrapulmonary solitary fibrous tumor with malignant transformationAnn Thorac Surg20161021e43e4527343529
- TominagaNKawarasakiCKanemotoKRecurrent solitary fibrous tumor of the pleura with malignant transformation and non-islet cell tumor-induced hypoglycemia due to paraneoplastic overexpression and secretion of high-molecular-weight insulin-like growth factor IIIntern Med201251233267327223207122
- YoshimuraYSanoKIsobeKAokiKKitoMKatoHA recurrent solitary fibrous tumor of the thigh with malignant transformation: a case reportInt J Surg Case Rep20162111111426967903
- ManousaridisKStropahlGGuthoffRFRezidivierender maligner solitärer fibröser Tumor der Orbita [Recurrent malignant solitary fibrous tumor of the orbit]Ophthalmologe20111083260264 German [with English abstract]21103878
- WangXQianJBiYPingBZhangRMalignant transformation of orbital solitary fibrous tumorInt Ophthalmol201333329930323525957
- BlandamuraSAlaggioRBettiniGGuzzardoVValentiniEBedogniAFour cases of solitary fibrous tumour of the eye and orbit: one with sarcomatous transformation after radiotherapy and one in a 5-year-old child’s eyelidJ Clin Pathol201467326326724108432
- YokoiTTsuzukiTYatabeYSolitary fibrous tumour: significance of p53 and CD34 immunoreactivity in its malignant transformationHistopathology19983254234329639117
- ChenHXiaoCWWangTOrbital solitary fibrous tumor: a clinicopathologic study of ten cases with long-term follow-upActa Neurochir (Wien)2012154224925522203231