
Abstract
Background
Aspirin has been revealed to probably decrease the risk of cholangiocarcinoma (CCC), which, nevertheless, is of controversy. To this end, a systematic review and meta-analysis was performed to investigate the above-described association.
Methods
We thoroughly searched PubMed, EMBASE, and ISI Web of Science for relevant studies published prior to October 2017, followed by random-effects model for calculation of pooled ORs and corresponding 95% CIs. Additionally, subgroup and sensitivity analyses were carried out to confirm whether the outcomes were stable.
Results
Nine articles, consisting of 12,535 CCC patients and 92,97,450 healthy controls, were enrolled in this study. We demonstrated a significantly decreased risk of CCC in those using aspirin, with studies being heterogeneous (OR=0.69; CI=0.43–0.94; I2=97.4%). Moreover, this relationship was detected only in case-control studies (OR=0.65; 95% CI=0.38–0.93), rather than cohort studies (OR=0.94; 95% CI=0.70–1.27). Besides, in separated analysis of intrahepatic CCC and extrahepatic CCC, aspirin was more strongly correlated with a declined risk of intrahepatic CCC (OR=0.33, 95% CI=0.26–0.39; I2=93.6%) than the risk of extrahepatic CCC (OR=0.56, 95% CI=0.41–0.73; I2=0%).
Conclusion
Collectively, the aspirin administration was correlated with a significant 31% decreased risk of CCC, particularly in the intrahepatic CCC.
Introduction
Cholangiocarcinoma (CCC) is a type of malignancy derived from the bile duct epithelium, which was first described by Durand-Fardel in 1840.Citation1 These tumors can be categorized into intrahepatic (ICC), extrahepatic(ECC), and hilar cholangiocarcinoma according to tumor location.Citation2 Hilar cholangiocarcinoma is usually considered as ECC.Citation3 CCC ranks the second among all primary hepatic carcinoma (HCC) in terms of incidence, accounting for 10%–25% of malignant HCCs and 3% of all gastrointestinal neoplasms.Citation4,Citation5 In addition, the incidence of CCC has continued to increase in recent years. Interestingly, there are certain differences of the epidemiological features between ICC and ECC. To be specific, there has been an increased incidence of ICC, while a decreased incidence of ECC in certain countries, including the UK and the USA.Citation6 In the USA, the age-adjusted incidence rate of ICC has risen by 165% in the last two decades, whereas that of ECC has declined by 14%.Citation7 In addition, CCC patients harbor a particularly poor prognosis. The overall 1-, 3-, and 5-year relative survival rates have been demonstrated to be 25.0%, 9.7%, and 6.8%, respectively, nearly without any changes in recent decades.Citation8 The causes of CCC are still not well defined, with only several risk factors being identified, including parasitic infections, bile duct cysts, hepatolithiasis as well as primary sclerosing cholangitis.Citation9 Recent studies have reported that some factors may increase CCC risk, including cirrhosis, hepatitis B or C, diabetes mellitus, gallstones, alcohol, and smoking.Citation10–Citation15 These risk factors have a common feature, which may be involved in the pathogenesis of CCC through a chronic biliary tract inflammatory process. Bile duct inflammation is a recognized cause of duct carcinogenesis.Citation11 Recently, a certain study has reported that aspirin, an inhibitor of COX-2, might suppress cancer progression by suppressing inflammatory processes.Citation16 Moreover, aspirin has been demonstrated to probably decrease CCC risk. Nevertheless, the results are conflicting. Accordingly, this meta-analysis was conducted for a better evaluation of the relationship between aspirin use and CCC risk.
Methods
The present research was carried out in line with PRISMA StatementCitation17 and the guidelines for Meta-analysis Of Observational Studies in Epidemiology (MOOSE).Citation18
Data sources and search strategy
PubMed, EMBASE, and Web of Science databases were thoroughly searched for relevant published studies using the following keywords: (“aspirin” OR “non-steroidal anti-inflammatory drugs” OR “NSAIDs” OR “salicylate” OR “cyclooxygenase-2 inhibitors” OR “COX-2 inhibitors”) and (“biliary tract neoplasms” OR “cholangiocarcinoma” OR “bile duct cancer” OR “biliary tract cancer”). Neither language nor date of publication was restricted.
Inclusion criteria
Eligible studies were included if they met the following criteria: study design (case control or cohort); aspirin as the exposure factor and CCC or bile duct cancer or biliary tract cancer as the outcome; accessible OR/risk ratio (RR) values and corresponding 95% CIs or adequate data for calculation. In the case of the same data reported by two studies, the study with a larger sample was selected.
Data extraction and quality evaluation
The extraction of necessary data was independently conducted by two investigators (WX and JB) from the selected studies following standardized protocol. The following data were extracted from every article: name of first author, year of publication, country, study design (case-control or cohort), period of follow-up, number of subjects, adjusted confounding variables, sources of controls, and OR/RR values and 95% CIs.
The study quality was assessed by the Newcastle–Ottawa Scale (NOS),Citation19 and quality categories were assigned in line with the scores of every research. The maximal score was 9 points. To be specific, NOS scores of <4, 4–6, and 7–9 suggested low-, medium-, and high-quality studies, respectively.Citation20 All discrepancies were handled by consensus.
Statistical analysis
The association between CCC risk and aspirin use was assessed by OR/RR values and corresponding 95% CIs, followed by quantification by random-effects model, which was proposed by DerSimonian and Laird.Citation21 HRs were considered as equivalent to RRs.
The ICitation2 statistic was employed for quantification of heterogeneity between studies, where ICitation2 values of 25%, 50%, and 75% indicated low, medium, and high heterogeneity, respectively.Citation22 A P-value <0.1 implicated the presence of heterogeneity. Meta-regression was used to evaluate the extent to which heterogeneity between the results was related to study design, geographical locations, and confounders adjusted for smoking status, alcohol use, and cholangitis. Funnel plots and Begg’sCitation23 and Egger’sCitation24 tests were employed to assess publication bias, where a P-value <0.05 or funnel plot asymmetry was indicative of bias.Citation25
Subgroup analyses were further conducted according to study design, geographic regions, tumor subtype, and whether smoking, alcohol consumption, or cholangitis were adjusted. Moreover, the stability of the outcomes was assessed by sensitivity analysis via sequential omission of one by one, which was conducted by altering the pooling model (fixed-effects model or random-effects model) and eliminating researches with NOS sources under 7 as well.Citation26
STATA version 12.0 (Stata) was employed for statistical analysis.
Results
Study selection and study features
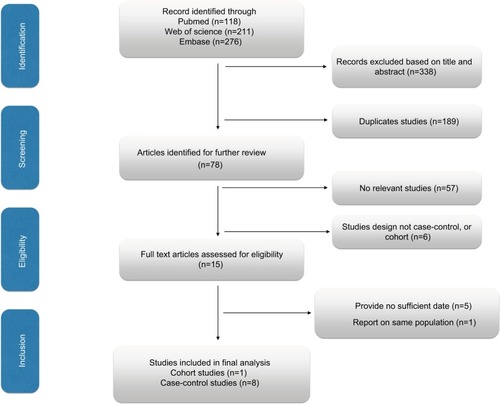
The selection process is shown in . In total, 605 studies were initially selected (118, 276, and 211 from PubMed, EMBASE, and Web of Science, respectively), while, 189 researches were repeated. Another 338 researches were eliminated after reviewing title and abstract. After further elimination of another five studies in consideration of inadequate information,Citation27–Citation31 nine eligible observational researches were ultimately enrolled in this meta-analysis.Citation32–Citation40
Figure 1 The process of study selection for the meta-analysis.
The major features of nine enrolled researches are sum-marized in .Citation32–Citation40Among them, four, three, and two studies were conducted in the USA, the UK, and China, respectively, all of which, were observational ones. Eight of these studies were case-control design, while the remaining one was cohort design. A total of 12,535 CCC subjects and 92,97,450 healthy controls were included to examine the role of aspirin on CCC risk in this meta-analysis, ranging from 1977 to 2016. The NOS scores of all selected researches varied from 5 to 9, with seven high-quality researches and two of medium quality ().
Table 1 The main characteristics of the included studies
Table 2 Scores of the Newcastle–Ottawa scale for included studies
Overall results
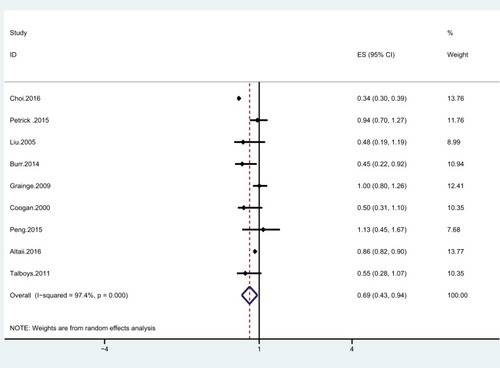
Of the nine researches, a significantly lower CCC risk was observed in those taking aspirin in three studies, while in the remaining six studies, there was no such correlation between the two. The pooled estimate was significant (OR=0.69; 95% CI=0.43–0.94), with studies being significantly heterogeneous (ICitation2=97.4%; P=0.001; ). Compared with non- use, aspirin administration was correlated with a significant 31% declined CCC risk. Nevertheless, the above correlation was detected only in case-control studies (OR=0.65; 95% CI=0.38–0.93), but not in cohort studies (OR=0.94; 95% CI=0.70–1.27; ).
Table 3 Subgroup and sensitivity analyses of the effect of aspirin and the risk of cholangiocarcinoma
Figure 2 Forest plot showing the relationship between aspirin and the risk of cholangiocarcinoma.
Notes: Points represent the risk estimates for each individual study. Horizontal lines represent 95% CIs, and diamonds represent the summary risk estimates with 95% CIs.
Abbreviation: ES, effect size.
Subgroup and sensitivity analyses
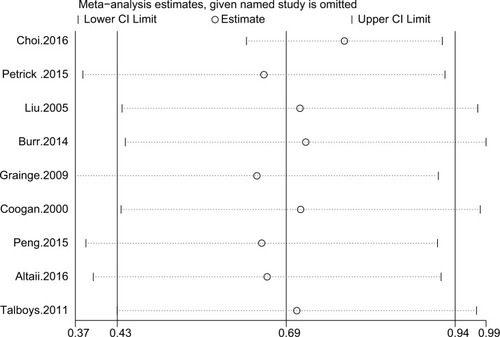
The outcomes of subgroup and sensitivity analyses are displayed in . In the separated analyses of ICC and ECC, we found that aspirin was more strongly correlated with a declined risk of ICC (OR=0.33; 95% CI=0.26–0.39; ICitation2=93.6%) than that of ECC (OR=0.56; 95% CI=0.41–0.73; ICitation2=0%). Sensitivity analysis indicated that after elimination of studies with NOS sources <7, aspirin use was stably related to CCC risk (). Moreover, the overall outcomes of the correlation between aspirin and CCC were stable in changing the pooling model (fixed-effects model: OR=0.64; 95% CI=0.61–0.67 and random-effects model: OR=0.69; 95% CI=0.43–0.94; ). In sequential omission of research one by one for evaluation of the outcomes stability, the pooled risk estimate was not affected by any study (). Meta-regression analyses were also performed to examine the potential source of heterogeneity, which, however, did not indicate that the study design (P=0.980), geographical locations (P=0.965), or confounders adjusted for smoking status (P=0.914), alcohol use (P=0.759), or cholangitis (P=0.745) was a source of heterogeneity.
Figure 3 Sensitivity analysis of the association between aspirin and the risk of cholangiocarcinoma.
Publication bias
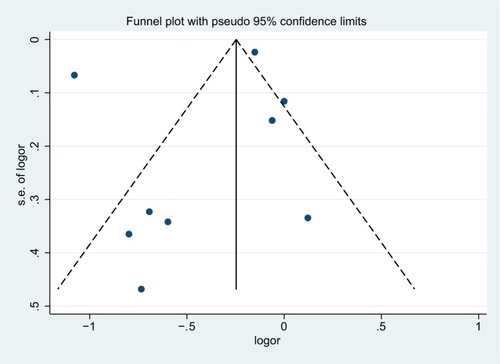
The funnel plot failed to demonstrate any substantial asymmetry, neither did Begg’s (P=0.468) nor Egger’s tests reveal any substantial publication bias (P>0.05; ).
Figure 4 Funnel plot of studies included in the meta-analysis of the relationships between aspirin and the risk of cholangiocarcinoma.
Abbreviations: logor, logodds ratio; s.e., standard error.
Discussion
Aspirin has been widely applied in prevention and treatment of diverse cerebrovascular disorders, such as myocardial infarction and stroke. At present, great attention has been paid to other potential benefits of aspirin globally. For instance, aspirin has been suggested to reduce the risk of certain types of malignancies, including colorectum, stomach, esophagus, breast, ovary, and lung.Citation41–Citation45 As far as we know, this is the first comprehensive meta-analysis exploring the association of aspirin use with CCC risk. We collected nine researches to explore the role of aspirin on CCC risk, which demonstrated that aspirin administration was related to a significant 31% decreased risk of CCC, especially in ICC.
Our finding of a decreased risk of CCC in patients taking aspirin has multiple possible explanations. Firstly, a previous study reported that overexpression of COX-2 might be a critical characteristic human CCC,Citation46 indicating COX-2 as potentially important targets relevant to chemoprevention or adjunct therapy of CCC.Citation47,Citation48 Thus, inhibition of COX-2 by aspirin may prevent CCC development through inhibition of inflammatory processes. Secondly, bile duct inflammation is a recognized cause of bile duct carcinogenesis.Citation11 Therefore, suppression of COX-2 by aspirin might also inhibit CCC progression by suppressing inflammatory processes.Citation16
The advantages of the study are as follows. To begin with, this is the first meta-analysis consisting of a large sample (12,535 CCC subjects and 92,97,450 healthy controls) in investigation of the role of aspirin in CCC risk, which might supply certain insight into the correlation of aspirin with CCC risk, and might be attractive in terms of CCC research. Moreover, further investigation concerning the mechanism of relationship of aspirin and CCC might give rise to novel therapeutic targets. Secondly, we further carried out subgroup and sensitivity analyses to identify the possible factors influencing the outcomes, which renders reliability of the present findings. Thirdly, the PubMed, EMBASE as well as Web of Science databases were comprehensively searched to collect possible researches in determining the factors affecting CCC risk. This systematic and comprehensive approach strengthened our findings. Additionally, the majority of enrolled researches harbored high quality in this meta-analysis. The above-described characteristics make our conclusions more reliable.
There exist certain shortcomings in the study. To begin with, the majority of the enrolled researches were case-control ones, thereby possibly leading to the generation of recall as well as selection biases. Besides, the current outcomes are subject to diagnostic bias. Those taking aspirin are prone to receive physical examination more frequently, which might result in more diagnoses than controls in general. Secondly, we did not search for unpublished studies or for original data. Besides, we did not take into account the possible interactions with other drugs due to a lack of relative data. Aspirin administration is often associated with other drugs use, such as statin and angiotensin converting enzyme inhibitors, which could have concealed a possible relationship with aspirin.Citation49 Thirdly, we only investigated a correlation, which might be affected by confounding bias. The followings are well-defined risk factors for CCC, including parasitic infections, bile duct cysts, hepatolithiasis as well as primary sclerosing cholangitis,Citation9 which, however, have been adjusted in a few studies. Fourthly, we failed to conduct a meta-analysis concerning the roles of different duration or doses of aspirin due to the restricted number of enrolled researches. Nevertheless, three studies reported results on the impact of both the dose of aspirin and the duration of aspirin treatment. Two studiesCitation34,Citation36 indicated that the impact of aspirin was dose dependent, with strong effect estimates in patients with >3 years of aspirin use in comparison with those harboring shorter use duration. Additionally, Choi et alCitation34 reveal that lower dose of aspirin (81–162 mg/day) may be more beneficial for CCC, than high dose aspirins (>325 mg/day). Petrick et al,Citation39 however, failed to discover a significantly different effect of aspirin when used for >163 mg or less. Finally, studies enrolled were significantly heterogeneous due to the differences in the study design, methods of measuring exposure, quality scores, and demographic characteristics inconsistency. In spite of inability to guarantee the source of heterogeneity, several sensitivity as well as subgroup analyses have been conducted to handle this issue.
In summary, our study indicated that aspirin administration was related to a significantly decreased CCC risk compared with those who never use aspirin. In the separate analysis of ICC and ECC, aspirin was suggested to be more strongly correlated with a decreased risk of ICC than that of ECC. More prospective and basic researches are warranted to confirm the correlation of aspirin with CCC risk as well as the potential mechanisms.
Acknowledgments
The study was funded by National key project research and development projects (S2016G9012), International Science and Technology Cooperation Projects (2015DFA30650), and the Capital Special Research Project for Clinical Application (Z151100004015170).
Author contributions
JPX conceived the study and wrote the manuscript. JPX and HCH searched database, reviewed studies, and selected date. WYX, YB, and JB performed statistical analyses. YYX, HTZ, and XL critically revised the article for essential intellectual content and administrative support. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- OlnesMJErlichRA review and update on cholangiocarcinomaOncology200466316717915218306
- PatelTCholangiocarcinomaNat Clin Pract Gastroenterol Hepatol200631334216397610
- TysonGLEl-SeragHBRisk factors for cholangiocarcinomaHepatology201154117318421488076
- VautheyJNBlumgartLHRecent advances in the management of cholangiocarcinomasSemin Liver Dis19941421091148047893
- ShaibYEl-SeragHBThe epidemiology of cholangiocarcinomaSemin Liver Dis200424211512515192785
- Taylor-RobinsonSDToledanoMBAroraSIncrease in mortality rates from intrahepatic cholangiocarcinoma in England and Wales 1968–1998Gut200148681682011358902
- ShaibYHDavilaJAMcglynnKEl-SeragHBRising incidence of intrahepatic cholangiocarcinoma in the United States: a true increase?J Hepatol200440347247715123362
- LepageCCottetVChauvenetMTrends in the incidence and management of biliary tract cancer: a French population-based studyJ Hepatol201154230631021056501
- KhanSAThomasHCDavidsonBRTaylor-RobinsonSDCholangiocarcinomaLancet200536694931303131416214602
- CaiHKongWTChenCBCholelithiasis and the risk of intra-hepatic cholangiocarcinoma: a meta-analysis of observational studiesBMC Cancer20151583126526500
- PalmerWCPatelTAre common factors involved in the pathogenesis of primary liver cancers? A meta-analysis of risk factors for intrahepatic cholangiocarcinomaJ Hepatol2012571697622420979
- WelzelTMGraubardBIEl-SeragHBRisk factors for intra-hepatic and extrahepatic cholangiocarcinoma in the United States: a population-based case-control studyClin Gastroenterol Hepatol20075101221122817689296
- ShaibYHEl-SeragHBNookaAKRisk factors for intrahepatic and extrahepatic cholangiocarcinoma: a hospital-based case-control studyAm J Gastroenterol200710251016102117324130
- ShaibYHEl-SeragHBDavilaJAMorganRMcglynnKARisk factors of intrahepatic cholangiocarcinoma in the United States: a case-control studyGastroenterology2005128362062615765398
- GuptaADixonEEpidemiology and risk factors: intrahepatic cholangiocarcinomaHepatobiliary Surg Nutr20176210110428503557
- HayashiNYamamotoHHiraokaNDifferential expression of cyclooxygenase-2 (COX-2) in human bile duct epithelial cells and bile duct neoplasmHepatology2001344 Pt163865011584358
- MoherDLiberatiATetzlaffJAltmanDGPRISMA GroupPreferred reporting items for systematic reviews and meta-analyses: the PRISMA StatementOpen Med200933e12313021603045
- StroupDFBerlinJAMortonSCMeta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) groupJAMA2000283152008201210789670
- StangACritical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analysesEur J Epidemiol201025960360520652370
- ZhangYPLiWQSunYLZhuRTWangWJSystematic review with meta-analysis: coffee consumption and the risk of gallstone diseaseAliment Pharmacol Ther201542663764826198295
- DerSimonianRLairdNMeta-analysis in clinical trialsControl Clin Trials1986731771883802833
- HigginsJPThompsonSGQuantifying heterogeneity in a meta-analysisStat Med200221111539155812111919
- BeggCBMazumdarMOperating characteristics of a rank correlation test for publication biasBiometrics1994504108811017786990
- EggerMDavey SmithGSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBr Med J199731571096296349310563
- StuckAERubensteinLZWielandDBias in meta-analysis detected by a simple, graphical test. Asymmetry detected in funnel plot was probably due to true heterogeneityBr Med J19983167129469469
- XiongJLinJWangATea consumption and the risk of biliary tract cancer: a systematic review and dose-response meta-analysis of observational studiesOncotarget2017824396493965728454105
- Long-term use of aspirin linked to reduced risk of developing bile duct cancerNurs Stand2016303815
- FriisSPoulsenAHJohnsenSPCancer risk among statin users: a population-based cohort studyInt J Cancer2005114464364715578694
- Cichoz-LachHCelińskiKCan nonsteroidal anti-inflammatory drugs favourably affect the alimentary canal?Ann Univ Mariae Curie Sklodowska Med200257239940212898869
- MorganGBeneficial effects of NSAIDs in the gastrointestinal tractEur J Gastroenterol Hepatol199911439340010321755
- SakodaLCGaoYTChenBEProstaglandin-endoperoxide synthase 2 (PTGS2) gene polymorphisms and risk of biliary tract cancer and gallstones: a population-based study in Shanghai, ChinaCarcinogenesis20062761251125616361272
- TalboysRJBurrNSavvaSThe role of non-steroidal anti-inflammatory drugs and statins in the aetiology of cholangiocarcinoma: preliminary results from a case control study in two UK centresGas-troenterology20111405S-595
- BurrNETalboysRJSavvaSAspirin may prevent cholangiocarcinoma: a case-control study from the United kingdomDig Dis Sci20145971567157224535250
- ChoiJGhozHMPeeraphatditTAspirin use and the risk of cholangiocarcinomaHepatology201664378579626940227
- GraingeMJWestJSolaymani-DodaranMAithalGPCardTRThe antecedents of biliary cancer: a primary care case-control study in the United KingdomBr J Cancer2009100117818019018260
- LiuESakodaLCGaoYTAspirin use and risk of biliary tract cancer: a population-based study in Shanghai, ChinaCancer Epidemiol Biomarkers Prev20051451315131815894693
- PengYCLinCLHsuWYStatins are associated with a reduced risk of cholangiocarcinoma: a population-based case-control studyBr J Clin Pharmacol201580475576125808421
- AltaiiHAl-KindiSGOliveiraGHYaqoobZRomero-MarreroCAspirin use and risk of cholangiocarcinoma: external validation with big dataHepatology20176541421142228052348
- PetrickJLSahasrabuddheVVChanATNSAID use and risk of hepatocellular carcinoma and intrahepatic cholangiocarcinoma: the liver cancer pooling projectCancer Prev Res201581211561162
- CooganPFRosenbergLPalmerJRNonsteroidal anti-inflammatory drugs and risk of digestive cancers at sites other than the large bowelCancer Epidemiol Biomarkers Prev20009111912310667472
- FlossmannERothwellPMEffect of aspirin on long-term risk of colorectal cancer: consistent evidence from randomised and observational studiesThe Lancet2007369957316031613
- HochmuthFJochemMSchlattmannPMeta-analysis of aspirin use and risk of lung cancer shows notable resultsEur J Cancer Prev201625425926826067033
- CaoYNishiharaRWuKPopulation-wide impact of long-term use of aspirin and the risk for cancerJAMA Oncol20162676276926940135
- TangLHuHLiuHJianCWangHHuangJAssociation of non-steroidal anti-inflammatory drugs and aspirin use and the risk of head and neck cancers: a meta-analysis of observational studiesOncotarget2016740651966520727533449
- HuangXZChenYWuJAspirin and non-steroidal anti-inflammatory drugs use reduce gastric cancer risk: a dose-response meta-analysisOncotarget2017834781479527902474
- EndoKYoonBIPairojkulCDemetrisAJSiricaAEERBB-2 over-expression and cyclooxygenase-2 up-regulation in human cholangiocarcinoma and risk conditionsHepatology200236243945012143054
- SiricaAELaiGHEndoKZhangZYoonBICyclooxygenase-2 and ERBB-2 in cholangiocarcinoma: potential therapeutic targetsSemin Liver Dis200222330331412360423
- SiricaAELaiGHZhangZBiliary cancer growth factor pathways, cyclooxygenase-2 and potential therapeutic strategiesJ Gastroenterol Hepatol200116436337211357901
- TakkoucheBEtminanMCaamañoFRochonPAInteraction between aspirin and ACE Inhibitors: resolving discrepancies using a meta-analysisDrug Saf200225537337812020174