
Abstract
Purpose
We aimed to compare and validate the prognostic value of inflammation-based prognostic scores for patients with resectable pancreatic ductal adenocarcinoma (PDAC) and to establish a novel, effective nomogram incorporating inflammation-based prognostic scores to predict disease-free survival (DFS) in these patients.
Patients and methods
Clinicopathological characteristics and follow-up data were retrieved from our prospective database. A total of 420 patients with PDAC who underwent radical resection were evaluated between January 2007 and December 2016. Blood samples were obtained within 7 days prior to surgical intervention. Time-dependent receiver operating characteristic curves were generated to determine optimal cutoff values for independent prognostic factors. Nomograms for DFS were established based on multivariate Cox proportional hazard models, and the results were internally validated using bootstrap resampling.
Results
Neutrophil-lymphocyte ratio (NLR) >2.13 and platelet-lymphocyte ratio (PLR) >140 were independent prognostic factors for DFS and overall survival. Stratified analyses indicated that these associations were not present among patients with stage III disease. Independent predictors of DFS, including Eastern Cooperative Oncology Group performance status score, tumor stage, differentiation, adjuvant treatment, NLR, and PLR, were incorporated into two nomograms for prediction of DFS in a cohort of PDAC patients after curative surgery. The area under receiver operating characteristic curve of the nomogram including NLR and PLR (0.804) was higher than that without NLR and PLR (0.711). The bootstrap-corrected AUC for the model including NLR and PLR was 0.803, while that for the model without NLR and PLR was 0.711.
Conclusion
Our study demonstrates that high NLR and high PLR are important clinical predictors of poor survival in patients with resectable PDAC. Additionally, a nomogram including NLR and PLR can objectively and reliably predict DFS among patients with PDAC following curative surgery.
Introduction
Pancreatic ductal adenocarcinoma (PDAC) ranks third among the causes of cancer-related death, with approximately 338,000 new cases annually worldwide.Citation1 Prognosis remains poor, and the 5-year cumulative survival rates for PDAC are estimated at less than 10%.Citation2 Surgical resection offers the only chance of cure; however, over 80% of patients experience local or distant recurrence after radical surgery.Citation3 Current predictions of tumor recurrence depend primarily on the histopathological characteristics of resected tumor specimens, including tumor size, histological grade, the depth of infiltration, and lymph node involvement; however, patients with equivalent pathological status often exhibit highly heterogeneous survival rates, suggesting that conventional characteristics are insufficient for optimal prediction of an individual’s prognosis.Citation4–Citation6 Hence, the identification of novel prognostic factors to enable a better risk stratification for follow-up schedules and individualized treatment of PDAC, has become critical.
Inflammation is a recognized hallmark of various malignant solid tumors, including PDAC.Citation7 Chronic inflammation contributes substantially to the development and progression of malignancies, through its influence on tumor angiogenesis, invasion, and metastasis.Citation8 Conversely, malignancies can also trigger regional inflammatory responses and the release of pro-inflammatory cytokines, leading to the formation of an inflammatory tumor microenvironment which favors tumor progression.Citation8,Citation9 Several prognostic factors based on analysis of systemic inflammation scores, including neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), lymphocyte-monocyte ratio (LMR), and prognostic nutritional index (PNI), have been proposed to estimate the magnitude of systemic inflammation in patients with cancer.Citation10,Citation11 These proposed biomarkers are potentially useful prognostic indicators for stratification of patients with good and poor prognosis.Citation10,Citation12,Citation13 The results of published studies that have examined the relationship between inflammation-based prognostic indices and resectable PDAC have been somewhat inconsistent to date.Citation12,Citation14,Citation15 Possible explanations for these inconsistencies may include the relatively small numbers included in these studies (n<100), differences in inclusion criteria and clinical endpoints, unclear selection of cutoff values, and concomitant evaluation of resectable and unresectable disease; these limitations would affect the reproducibility and reliability of these markers. Furthermore, inflammation-based prognostic indices have yet to be appropriately validated for clinical decision-making. Therefore, the aim of this study was to compare the prognostic values of NLR, PLR, LMR, and PNI and to develop a nomogram incorporating inflammation-based prognostic indices to predict the disease-free survival (DFS) in a large cohort of 420 patients with PDAC who underwent curative resection.
Materials and methods
Study population
We conducted a retrospective study of patients with PDAC who underwent potentially radical resection from January 2007 to December 2016 at the Chinese PLA General Hospital, Beijing, China. Patients were excluded from the study if they met the following criteria: 1) without pathologically confirmed PDAC; 2) positive surgical margins; 3) presence of distant metastasis; 4) preoperative chemotherapy or radiotherapy for PDAC; 5) other malignancies diagnosed within 5 years; 6) clinical evidence of acute infection or other inflammatory conditions; 7) previous hematological or autoimmune disease; and 8) no complete record of preoperative hematological variables and follow-up data. Following these exclusions, a total of 420 patients with PDAC were eligible for the present study. Approval for the study was granted by the ethics committee of the Chinese PLA General Hospital, and the requirement to obtain written informed consent from patients was waived due to the retrospective nature of the investigation. To protect patient privacy, all personal information was appropriately anonymized and de-identified prior to analysis.
Data collection and clinical definition
Information regarding the clinicopathological characteristics, sociodemographic data, and lifestyle factors were retrieved from medical records. Laboratory data, including routine blood examination, albumin concentration, and levels of the tumor markers, CA19-9, CA125, and CEA, were obtained within 7 days prior to surgical intervention. Pathological data included tumor size, histological type, grade, the presence of micro-invasion (of nerves, lymphatics, and vessels), number of cancer positive lymph nodes, and microscopic status of all evaluated resection margins. Pathological staging was performed according to the tumor-node-metastasis (TNM) classification system; as the TNM classification system for PDAC changed during the study period, tumors were uniformly staged according to the eighth edition of this system. Alcohol intake was classified as either currently drinking almost/more than once a week or not. Smoking habit was defined as either smoking more than once a day or not. Body mass index (BMI) was calculated as weight divided by height squared (in kg m2). NLR was defined as the absolute neutrophil count divided by absolute lymphocyte count. PLR was calculated as the absolute platelet count divided by the absolute lymphocyte count. LMR was determined as the absolute lymphocyte count divided by absolute monocyte count. PNI was calculated as 10× albumin (g/dL) +0.005× total lymphocyte count (per mm3).
Follow-up data were collected prospectively, and all patients were followed-up every 3 months during the first and second postoperative year, every 6 months in the third to fifth years, and annually thereafter. If recurrence was confirmed, the follow-up interval was 3 months. The closing date for follow-up was February 30, 2018. The primary endpoint of the study was DFS. The secondary endpoint was overall survival (OS). DFS was defined as the time from surgical resection to local recurrence or distant metastasis. OS was defined as the interval between the date of a definitive diagnosis and cancer-related death. Patients were censored at the date of last follow-up.
Statistical analysis
Continuous variables are expressed as median (25th, 75th percentile) and categorical variables as frequency and percentage. Differences in the distribution of categorical variables were evaluated using the chi-squared test. Time-dependent receiver operating characteristic (ROC) curves were generated to determine the optimal cutoff values of independent prognostic factors. Kaplan–Meier analyses with log-rank tests were used to compare survival outcomes between patients with systemic inflammatory marker values above vs below optimal cutoff points. Cox proportional hazard models were used to assess the relationships between systemic inflammatory markers and survival outcomes. Unadjusted and multivariate adjusted models were applied, and HR and 95% confidence intervals (CIs) calculated. Nomograms for predicting 1-year DFS were established based on the results of multivariate Cox proportional hazard regression models. A backward model selection technique was used for the final model selection, and predictive accuracy was evaluated by calculation of the area under the ROC curve. The performance of the models was internally validated using bootstrapping (500 samples). Statistical significance was defined as a two-tailed P-value <0.05.
All statistical analyses were undertaken using the statistical software packages, R (http://www.R-project.org, The R Foundation) and EmpowerStats (http://www.empowerstats.com, X&Y Solutions, Inc., Boston, MA, USA).
Results
summarizes the detailed clinical characteristics of the 420 eligible patients. The median follow-up time was 38 months (range 1–75 months). Of the 420 resectable PDAC patients, 382 (91%) developed tumor recurrence and 346 (82.4%) died within the follow-up period. The median DFS and OS were 9.2 and 14.4 months, respectively.
Table 1 Baseline characteristics of patients
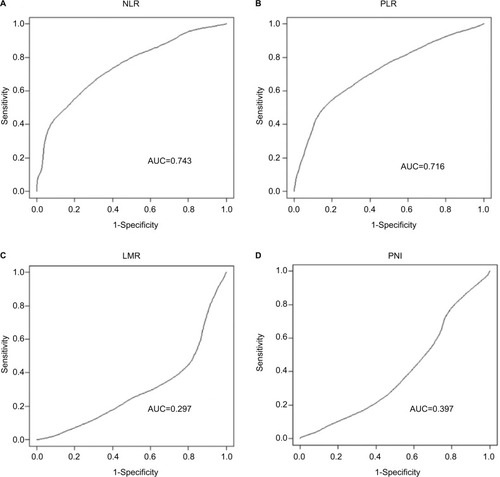
The AUCs of the time-dependent ROC curve analyses are presented in and ROC curves are shown in . The AUCs for NLR and PLR were 0.743 and 0.715, respectively. The optimal cutoff value for NLR was 2.13, with a sensitivity of 61.7% and a specificity of 74.1% for 1-year DFS. For PLR, the optimal cutoff value was 140 with a sensitivity of 54.1% and a specificity of 80.6%. LMR and PNI were not suitable for inclusion in subsequent analyses since their AUC values were <0.5.
Table 2 ROC curve analyses of the NLR, PLR, LMR, and PNI for 1-year DFS
Figure 1 ROC curves of NLR, PLR, LMR, and PNI for 1-year DFS.
Note: (A) NLR, (B) PLR, (C) LMR, and (D) PNI.
Abbreviations: AUC, area under the curve; DFS, disease-free survival; LMR, lymphocyte-monocyte ratio; NLR, neutrophil-lymphocyte ratio; PLR, platelet-lymphocyte ratio; PNI, prognostic nutritional index; ROC, receiver operating characteristic.
Patients were divided into low or high groups based on NLR and PLR cutoff values. Comparisons of the baseline characteristics of patients stratified by NLR and PLR are presented in . Compared to low NLR (<2.13), high NLR (>2.13) was significantly associated with unfavorable tumor characteristics including higher T stage, more positive lymph nodes, and advanced stage. Similar significant differences were also observed when the two groups were stratified by PLR.
Table 3 Baseline characteristics stratified by NLR and PLR
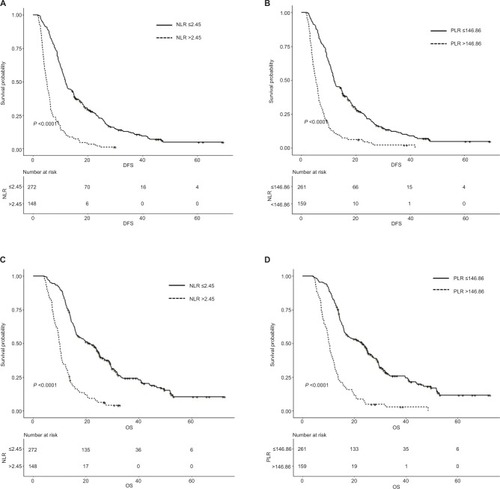
Kaplan–Meier analyses demonstrated that high preoperative NLR and PLR were associated with worse DFS and OS. The median DFS and OS of patients with an NLR of ≤2.13 was 12.4 and 23.1 months, respectively, whereas for patients with an NLR of >2.13 the equivalent values were 6.0 and 10.7 months, respectively (both P<0.01; ). Patients with PLR ≤140 had superior DFS (12.1 vs 5.9 months, P<0.001) and OS (23.5 vs 10.6 months, P<0.001) compared to those with PLR >140 ().
Figure 2 Kaplan–Meier curves of NLR and PLR for DFS and OS.
Notes: (A) NLR for DFS, (B) PLR for DFS, (C) NLR for OS, (D) PLR for OS.
Abbreviations: DFS, disease-free survival; NLR, neutrophil-lymphocyte ratio; OS, overall survival; PLR, platelet-lymphocyte ratio.
The results of univariate and multivariable Cox regression analyses are presented in . Both high NLR and high PLR were identified as independently associated with inferior DFS and OS in unadjusted analysis. The adjusted HR (95% CI), P-value of worse DFS and OS for patients with high NLR were 1.59 (1.27–2.00), <0.001 and 1.70 (1.33–2.16), <0.001, respectively. Patients with high PLR had inferior DFS (HR [95% CI]: 1.93 [1.53–2.45], P<0.001) and OS (HR [95% CI]: 2.23 [1.74–2.85], P<0.001) compared to their counterparts with low PLR.
Table 4 Multivariate analyses for DFS and OS
Given the close relationship between survival outcomes and tumor stage, we also performed an analysis with data stratified by tumor stage subgroups (). Both high NLR and high PLR remained independent risk factors for inferior DFS and OS in patients with stage I and II tumors; however, for patients with stage III disease, these associations were lost after adjustment for confounding factors.
Table 5 Multivariate analyses of NLR and PLR for DFS and OS stratified by pTNM stage
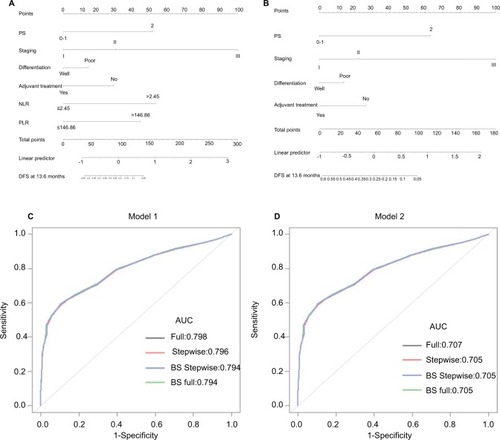
To predict the 1-year DFS of patients with resectable PDAC, nomograms () were established using a multivariate Cox regression model incorporating all significant independent predictors of DFS. Eastern Cooperative Oncology Group performance status (ECOG PS) score, stage, differentiation, adjuvant treatment, NLR, and PLR were incorporated into the DFS nomograms. The AUCs of the nomograms, either including or excluding NLR and PLR, were 0.804 and 0.711, respectively (). The respective C-indices of the nomograms including or excluding NLR and PLR were 0.750 and 0.679. The discriminative performance of the nomogram (bootstrap-corrected AUC) was 0.803 for the model including NLR and PLR, and 0.711 for that excluding NLR and PLR.
Figure 3 Nomograms and their accuracy for predicting 1-year DFS in patients with resectable PDAC.
Notes: (A) Nomogram including NLR and PLR, (B) nomogram without NLR and PLR, (C) bootstrap-corrected AUCs for model including NLR and PLR, (D) bootstrap-corrected (BS) AUCs for model without NLR and PLR.
Abbreviations: AUCs, areas under the curve; DFS, disease-free survival; ECOG PS, Eastern Cooperative Oncology Group performance status; NLR, neutrophil-lymphocyte ratio; PDAC, pancreatic ductal adenocarcinoma; PLR, platelet-lymphocyte ratio.
Discussion
In the present study, we demonstrated that NLR >2.13 and PLR >140 can be reliable predictive markers for shorter DFS and OS in a large and homogenous population of patients with resectable PDAC. After adjustment for a wide range of potential confounding factors, NLR >2.13 and PLR >140 remained independent unfavorable prognostic factors with clinically relevant HR values; however, these associations were not consistent among the patient subgroup with stage III tumors. Additionally, we presented a nomogram including NLR and PLR that predicts the 1-year DFS with good discriminative performance. To the best of our knowledge, this is the first nomogram for patients with resected PDAC incorporating inflammation-based prognostic indices to effectively predict DFS.
It is well-established that cancer progression is determined not only by oncogenes or tumor suppressor genes within the tumor itself but also by host-related factors such as age, sex, performance status, and inflammatory responses.Citation16 The relationship between systemic inflammation and cancer progression has been subject to increasing attention in investigation of various gastrointestinal malignancies, including PDAC.Citation17,Citation18 Cancer-related inflammation involves crosstalk of inflammatory cells and mediators, such as cytokines and chemokines; however, systemic levels of cytokines and chemokines are some way from routine clinical use. Therefore, several prognostic scores, based on shifts in the cellular components that occur during systemic inflammation have been proposed.Citation19–Citation21
Neutrophils, major components of the leukocyte population, can migrate from the venous system to tumors and may be triggered in the presence of cancer-related inflammatory factors, such as interleukin-6 (IL-6), granulocyte colony-stimulating factor, and by myeloid growth factors produced during neoplastic processes.Citation22 Neutrophils can release various factors, such as reactive oxygen species, leading to DNA damage, genetic instability, and tumor growth.Citation23,Citation24 In contrast, neutrophils interact with various other cell populations, leading to generation of numerous cytokines and effector molecules, particularly vascular endothelial growth factor (VEGF), which is important for tumor angiogenesis, growth, and metastasis.Citation25 In addition, neutrophil subpopulations in the vicinity of the tumor microenvironment may suppress the antitumor immune responses of natural killer cells and activated T cells mediated by integrin Mac-1 and hydrogen peroxide.Citation26
Lymphocytes, which are the cellular mediators of immunosurveillance and immunoediting, have crucial roles in antitumor reactions through induction of cytotoxic cell death and inhibition of tumor cell proliferation and migration.Citation8 During cancer-related inflammation, the presence of tumor-infiltrating lymphocytes with high CD4+/CD8+ and Th2/Th1 ratios is indicative of poor prognosis.Citation27
Platelets, the major transporter of VEGF, are regulated by pro-inflammatory cytokines, such as IL-1, IL-6, IL-11, and TNF-a.Citation28 Platelets can also contribute substantially to tumor vascular growth through secretion of a number of proangiogenic cytokines, including VEGF, platelet-derived growth factor, and thymidine phosphorylase.Citation29,Citation30 Platelet aggregation also facilitates tumor cell adhesion to the vascular endothelium, which can act as a physiological shield, protecting tumor cells against NK cell-mediated lysis.Citation31 Additionally, tumor cell infiltration and metastasis are induced via platelet-mediated activation of the TGFb/Smad pathway.Citation32
Overall, neutrophilia, thrombocytosis, and lymphopenia tend to contribute to cancer-related inflammatory responses, and the NLR and PLR, simple derivatives of routine blood counts, can reflect the dynamic balance between anti- and pro-tumor functions of the immune system.Citation33
Currently, there is no consensus on the appropriate cutoff values for NLR and PLR for prediction of prognosis in patients with PDAC; thus, various thresholds have been used in previous studies. For NLR, many studies have used a cutoff value of 5.0,Citation34–Citation36 while others used values varying from 2.2 to 4.0.Citation15,Citation37–Citation39 PLR cutoff values of 150, 160, and 300 have been used in previous studies.Citation14,Citation15,Citation36,Citation40,Citation41 In some studies, patients were even categorized according to quartiles or mean values of NLR or PLR;Citation42 however, despite these differences in cutoff values, all studies reported worse survival when NLR or PLR exceeded the threshold. Unlike studies that set cutoff values for NLR and PLR empirically, we used time-dependent ROC to determine the values, and calculated optimal thresholds of 2.13 for NLR and 140 for PLR. The AUCs of NLR and PLR were 0.743 and 0.715, respectively, indicating that both indices are promising predictors of DFS in patients with resectable PDAC. In contrast, the AUCs of LMR and PNI were both <0.5, demonstrating no prognostic power for predicting DFS. Further survival analyses showed that high NLR and high PLR (above the threshold values) were significantly associated with impaired DFS and OS, independent of a wide range of potential confounding factors. These results are consistent with previous publications.Citation15,Citation37 Interestingly, in analysis stratified by TNM stage, we demonstrated that patient subgroups with stage I–II tumors presented different DFS and OS according to their NLR or PLR values; however, these associations were not observed for patients with stage III tumors. The small number of patients with stage III disease may be an important factor contributing to this phenomenon. Although these results are insufficient to directly influence clinical practice at present, they provide valuable information regarding clinical risk stratification to facilitate improved personalized medical care, such as a closer follow-up once high NLR and/or high PLR are identified, even among patients with the same stage tumor.
Accurate information on prognostication is useful for medical decision-making and clinical counseling. Nomo-grams, statistical instruments that can evaluate multiple relevant clinical factors and predict the continuous probability of a particular outcome for an individual patient, have been used in an extensive array of applications, including cancer.Citation43 To allow physicians to tailor prognostication for patients with resectable PDAC who maintain an underlying constant systemic inflammatory status, we established a nomogram incorporating NLR and PLR and compared its discriminatory ability to an instrument not incorporating NLR and PLR. In our study, the independent predictors, ECOG PS score, tumor stage, differentiation, adjuvant treatment, NLR, and PLR, were incorporated into the two nomograms. The AUCs of the nomograms including or excluding NLR and PLR were 0.804 and 0.711, respectively, indicating that the former had superior discrimination ability for prediction of clinical outcomes. In addition, the nomogram incorporating NLR and PLR performed well on bootstrap validation, with a bootstrap-corrected AUC of 0.803. Thus, for example, a patient with an ECOG PS score of 0–1 (0 points), stage II tumor (65 points), well-differentiated tumor (0 points), NLR >2.13 (90 points), PLR ≤140 (0 points), and no adjuvant treatment (95 points) would score 250 total points, which converts to a probability for 1-year DFS of <10%. The predictors included in our nomogram are all available in routine clinical practice; therefore, we believe that it can be easily used by clinicians to make accurate individualized estimates of prognosis.
The strengths of our study are the large sample size and the long follow-up period. Moreover, our prediction model enables surgical PDAC patients to be monitored easily on an individual basis. Nevertheless, the investigation had several limitations that merit emphasis. First, although the current study adjusted for a considerable number of potential confounders, we cannot rule out the possibility that the results may have been affected by other variables that were not included in the analyses. Second, patients were included in the database over a period of 10 years; therefore, it is possible that advances in surgical techniques and medical oncology have combined to improve survival of patients with resected PDAC. Hence, we used the bootstrapping technique to obtain an almost unbiased internal assessment of accuracy. Although the results of the bootstrapping correction procedure are promising, they do not negate the need for future studies to externally validate whether our nomograms can be generalized to new patient populations. Furthermore, our conclusions were solely drawn from the objective clinical data, as it was beyond the scope of our study to elucidate the potential mechanism underlying the prognostic value of inflammatory markers.
Conclusion
In the present study, we demonstrated that high NLR and high PLR are clinically important predictors of poor survival in patients with resectable PDAC. Additionally, our predictive nomogram including NLR and PLR can objectively and reliably predict DFS among PDAC patients after curative surgery, and performed well on internal validation. Therefore, with their advantages of cost-effectiveness and simplicity, NLR and PLR may be useful for stratification of high-risk subpopulations of patients with resectable PDAC in terms of recurrence and poor survival, even where tumors are the same stage. A further large-scale prospective validation study is needed to determine whether these results are widely applicable.
Author contributions
Both authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- American Cancer Society [homepage on the Internet]Cancer Statistics Center Available from: http://cancerstatisticscenter.cancer.orgAccessed August 7, 2018
- SharmaCEltawilKMRenfrewPDWalshMJMolinariMAdvances in diagnosis, treatment and palliation of pancreatic carcinoma: 1990–2010World J Gastroenterol201117786789721412497
- KatzMHWangHFlemingJBLong-term survival after multidisciplinary management of resected pancreatic adenocarcinomaAnn Surg Oncol200916483684719194760
- FortnerJGKlimstraDSSenieRTMacleanBJTumor size is the primary prognosticator for pancreatic cancer after regional pancreatectomyAnn Surg199622321471538597508
- RautCPTsengJFSunCCImpact of resection status on pattern of failure and survival after pancreaticoduodenectomy for pancreatic adenocarcinomaAnn Surg20072461526017592291
- SchmidtCMMatosJMBentremDJTalamontiMSLillemoeKDBilimoriaKYAcinar cell carcinoma of the pancreas in the United States: prognostic factors and comparison to ductal adenocarcinomaJ Gastrointest Surg200812122078208618836784
- MckayCJGlenPMcMillanDCChronic inflammation and pancreatic cancerBest Pract Res Clin Gastroenterol2008221657318206813
- MantovaniAAllavenaPSicaABalkwillFCancer-related inflammationNature2008454720343644418650914
- GrivennikovSIGretenFRKarinMImmunityKMImmunity, inflammation, and cancerCell2010140688389920303878
- ProctorMJMorrisonDSTalwarDA comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome StudyEur J Cancer201147172633264121724383
- McMillanDCSystemic inflammation, nutritional status and survival in patients with cancerCurr Opin Clin Nutr Metab Care200912322322619318937
- ProctorMJMorrisonDSTalwarDAn inflammation-based prognostic score (mGPS) predicts cancer survival independent of tumour site: a Glasgow Inflammation Outcome StudyBr J Cancer2011104472673421266974
- KasymjanovaGMacDonaldNAgulnikJSThe predictive value of pre-treatment inflammatory markers in advanced non-small-cell lung cancerCurr Oncol20101745258
- StotzMGergerAEisnerFIncreased neutrophil-lymphocyte ratio is a poor prognostic factor in patients with primary operable and inoperable pancreatic cancerBr J Cancer2013109241642123799847
- SmithRABosonnetLRaratyMPreoperative platelet-lymphocyte ratio is an independent significant prognostic marker in resected pancreatic ductal adenocarcinomaAm J Surg2009197446647218639229
- ElinavENowarskiRThaissCAHuBJinCFlavellRAInflammation-induced cancer: crosstalk between tumours, immune cells and microorganismsNat Rev Cancer2013131175977124154716
- GencerDKästle-LarraldeNPilzLRPresentation, treatment, and analysis of prognostic factors of terminally ill patients with gastrointestinal tumorsOnkologie200932738038619556814
- SiddiquiAHeinzerlingJLivingstonEHHuertaSPredictors of early mortality in veteran patients with pancreatic cancerAm J Surg2007194336236617693283
- LeitchEFChakrabartiMCrozierJEComparison of the prognostic value of selected markers of the systemic inflammatory response in patients with colorectal cancerBr J Cancer20079791266127017923866
- CondeelisJPollardJWMacrophages: obligate partners for tumor cell migration, invasion, and metastasisCell2006124226326616439202
- HuhJWLeeJHKimHRPrognostic significance of tumor-infiltrating lymphocytes for patients with colorectal cancerArch Surg2012147436637222508783
- LiangWFerraraNThe Complex Role of Neutrophils in Tumor Angiogenesis and MetastasisCancer Immunol Res201642839126839309
- McCollSRPaquinRMénardCBeaulieuADHuman neutrophils produce high levels of the interleukin 1 receptor antagonist in response to granulocyte/macrophage colony-stimulating factor and tumor necrosis factor alphaJ Exp Med199217625935981386877
- WeitzmanSAGordonLIInflammation and cancer: role of phagocyte-generated oxidants in carcinogenesisBlood19907646556632200535
- KusumantoYHDamWAHospersGAMeijerCMulderNHPlatelets and granulocytes, in particular the neutrophils, form important compartments for circulating vascular endothelial growth factorAngiogenesis20036428328715166496
- PillayJKampVMvan HoffenEA subset of neutrophils in human systemic inflammation inhibits T cell responses through Mac-1J Clin Invest2012122132733622156198
- KohrtHENouriNNowelsKJohnsonDHolmesSLeePPProfile of immune cells in axillary lymph nodes predicts disease-free survival in breast cancerPLoS Med200529e28416124834
- BambaceNMHolmesCEThe platelet contribution to cancer progressionJ Thromb Haemost20119223724921040448
- MöhleRGreenDMooreMANachmanRLRafiiSConstitutive production and thrombin-induced release of vascular endothelial growth factor by human megakaryocytes and plateletsProc Natl Acad Sci U S A19979426636689012841
- OkamotoEOsakiMKaseSAdachiHKaibaraNItoHThymidine phosphorylase expression causes both the increase of intratumoral microvessels and decrease of apoptosis in human esophageal carcinomasPathol Int200151315816411328530
- GayLJFelding-HabermannBContribution of platelets to tumour metastasisNat Rev Cancer201111212313421258396
- LabelleMBegumSHynesRODirect signaling between platelets and cancer cells induces an epithelial-mesenchymal-like transition and promotes metastasisCancer Cell201120557659022094253
- HanahanDCoussensLMAccessories to the crime: functions of cells recruited to the tumor microenvironmentCancer Cell201221330932222439926
- GarceaGLadwaNNealCPMetcalfeMSDennisonARBerryDPPreoperative neutrophil-to-lymphocyte ratio (NLR) is associated with reduced disease-free survival following curative resection of pancreatic adenocarcinomaWorld J Surg201135486887221312035
- ClarkEJConnorSTaylorMAMadhavanKKGardenOJParksRWPreoperative lymphocyte count as a prognostic factor in resected pancreatic ductal adenocarcinomaHPB20079645646018345294
- JamiesonNBDenleySMLogueJA prospective comparison of the prognostic value of tumor- and patient-related factors in patients undergoing potentially curative surgery for pancreatic ductal adenocarcinomaAnn Surg Oncol20111882318232821267785
- SzkanderaJStotzMEisnerFExternal validation of the derived neutrophil to lymphocyte ratio as a prognostic marker on a large cohort of pancreatic cancer patientsPLoS One2013811e7822524223776
- TeoMMohd SharialMSMcDonnellFConlonKCRidgwayPFMcDermottRSPrognostic role of neutrophil-to-lymphocyte ratio in advanced pancreatic ductal adenocarcinoma: impact of baseline fluctuation and changes during chemotherapyTumori201399451652224326841
- BhattiIPeacockOLloydGLarvinMHallRIPreoperative hematologic markers as independent predictors of prognosis in resected pancreatic ductal adenocarcinoma: neutrophil-lymphocyte versus platelet-lymphocyte ratioAm J Surg2010200219720320122680
- WangDSLuoHYQiuMZComparison of the prognostic values of various inflammation based factors in patients with pancreatic cancerMed Oncol20122953092310022476808
- AliustaogluMBiliciASekerMThe association of pre-treatment peripheral blood markers with survival in patients with pancreatic cancerHepatogastroenterology20105799–10064064520698242
- AsaokaTMiyamotoAMaedaSPrognostic impact of preoperative NLR and CA19-9 in pancreatic cancerPancreatology201616343444026852169
- IasonosASchragDRajGVPanageasKSHow to build and interpret a nomogram for cancer prognosisJ Clin Oncol20082681364137018323559