
Abstract
Background
Choriocarcinoma usually occurs in females and sometimes occurs in the testicles of males. Extragonadal choriocarcinoma in males was previously described in case reports, and our understanding of this type of cancer has remained limited. The purpose of this study was to explore the incidence, treatment and prognostic factors of extragonadal choriocarcinoma in males.
Materials and methods
Two cohorts were identified from the Surveillance, Epidemiology, and End Results (SEER) Program by histology, tumor site and sex. One cohort of 115 patients was created using the SEER nine registries (1973–2014) to estimate the incidence. The other cohort of 197 patients was created using the SEER 18 registries (1973–2013) to estimate the patient demographics and survival.
Results
The median age at diagnosis was 30 years. The most common primary tumor location was the mediastinum followed by the retroperitoneum and the brain. Approximately 23% of patients underwent beam radiation therapy, whereas 63.5% underwent surgery. The estimated one- and 5-year cause-specific survival rates were 49% and 35%, respectively. The multivariate analysis showed that the age at diagnosis, ie, a younger age of 0–19 years old, and the primary tumor site, ie, the brain, were the independent prognostic factors and were correlated with a favorable prognosis. The median survival time of patients was 186 months, 13 months and 4 months in the 0–19, 20–49 and 50+ years of age, respectively.
Conclusion
Extragonadal choriocarcinoma in males is a rare malignancy with a poor prognosis. A young age at diagnosis and primary tumor site in the brain were the independent prognostic factors.
Introduction
Choriocarcinoma is a highly malignant neoplasm that most commonly occurs in females and is related to a gestational event. In males, choriocarcinoma is generally considered a nonseminomatous germ cell tumor, which represents less than 5% of all germ cell tumors in males.Citation1 Choriocarcinoma in males commonly develops in the gonads (ie, testes). In some cases, extragonadal choriocarcinoma occurs in midline locations, such as the mediastinum, retroperitoneum and pineal gland, with rare cases reported in the parenchymal organs, such as the lungs, gastrointestinal tract and breast.Citation2–Citation7 Although the burden of extragonadal germ cell tumors has been previously described in population-based studies, extragonadal choriocarcinoma in males has not been specified.Citation8,Citation9
Several hypotheses have been proposed by pathologists to explain the etiology of extragonadal choriocarcinoma: 1) the tumor arises from retained primordial germ cells that migrate abnormally during embryogenesis; 2) metastasis occurs from a gonadal choriocarcinoma that regressed spontaneously; and 3) development is a consequence of multidirectional tumor differentiation from a common stem cell in malignant epithelium. Recently, novel somatic and germline mutations have been reported to correlate with extragonadal germ cell tumors; however, strict pathological distinctions for the development of choriocarcinoma seem to be very difficult for pathologists to apply.Citation10–Citation12 The etiology suggests that prognostic factors of extragonadal choriocarcinoma should not be implied from the extragonadal germ cell cancer or testicular choriocarcinoma, despite the 5-year relative survival rate of 71% and 68% for extragonadal germ cell cancer in Europe and in the USA, respectively, and the testicular choriocarcinoma 5-year survival rate of less than 80% in the USA.Citation9,Citation13,Citation14 Based on previous case reports, the prognostic factors of extragonadal choriocarcinoma in males was not fully understood.
The Surveillance, Epidemiology, and End Results (SEER) database of the National Cancer Institute provides data on cancers in 18 geographical areas of the USA and covers ~26% of the population. We performed this population-based study to explore the incidence and prognostic factors of extragonadal choriocarcinoma in males and aimed to provide a more accurate estimate of the incidence and survival rate of this very rare disease.
Materials and methods
The SEER Program
Two cohorts of patients were created using the SEER program (www.seer.cancer.gov) SEER*Stat Database. One cohort to estimate the incidence was created using the SEER 9 Registries Research Data, November 2016 Submission (1973–2014)<Katrina/Rita Population Adjustment>. The other cohort to estimate the patient demographics and survival was created using SEER 18 Registries Research Data+Hurricane Katrina Impacted Louisiana Cases, November 2015 Submission (1973–2013 varying).
The selection of patients was based on 1) ICD for Oncology (ICD-O) codes of 9100/2: Choriocarcinoma in situ, NOS, 9100/3: Choriocarcinoma, NOS, 9101/2: Choriocarcinoma combined with other germ cell elements, in situ, 9101/3: Choriocarcinoma combined with other germ cell elements; 2) sex is male; 3) site is not “Testis – male”. Finally, one cohort of 115 eligible patients was enrolled to estimate the incidence and the other cohort of 197 eligible patients was enrolled to estimate the patient demographics and survival in this study.
Statistical analysis
Incidence rates were analyzed with SEER*Stat Software version 8.3.5 (Surveillance Research Program, National Cancer Institute, seer.cancer.gov/seerstat). Trends in incidence rates were analyzed with the Joinpoint Regression Program (version 4.5.0.1; Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute) using the Joinpoint regression model and permutation tests for identifying changes in trends.Citation15 Statistical analysis was performed with SPSS Statistical Package version 24.0 (SPSS Inc, Chicago, IL, USA). Rates were per 100,000 and age was adjusted to the 2000 US standard population. Percent change was calculated using 1 year for each end point. The tumor stage was classified by SEER summary stage 1977 (1995–2000). Marital status was divided into two groups: married and others, which included never married, widowed, divorced, separated, unmarried or domestic partner, and unknown. The age at diagnosis between two groups was compared using a t-test. Rates of surgery and beam radiation treatment between groups were compared using chi-squared test. The 1-, 3- and 5-year cause-specific survival (CSS) rates were estimated by the life table method, and median survival rates were estimated by Kaplan–Meier analyses and then compared statistically using the log-rank test. The prognostic factors were determined by univariate regression analysis, where HRs with 95% CIs were calculated to estimate the risk of death. A multivariable analysis was further performed to find independent prognostic factors using the Cox proportional hazards. P<0.05 was considered statistically significant.
Ethical approval
The ethical approval and informed consent statements are not applicable for this type of research. The data accessed from the SEER database are freely available.
Results
Incidence
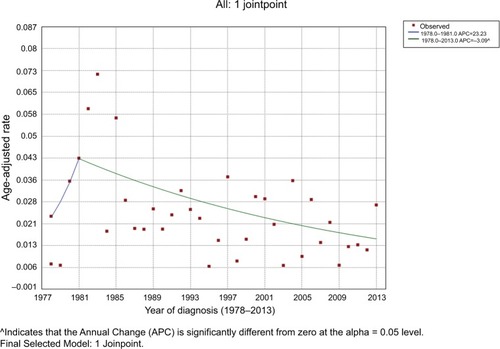
Between 1973 and 2014, a total of 115 male patients exhibiting extragonadal choriocarcinoma were identified in the SEER nine registries. The overall incidence rate for extragonadal choriocarcinoma in males during that period based on the SEER data was 0.022 per 100,000 people (95% CI: 0.018 to 0.026). In 1977 and 2014, the frequency was zero, which cannot be processed by Joinpoint trend analysis; therefore, we calculated the age-adjusted rates from 1978 to 2013 instead. The incidence of extragonadal choriocarcinoma in males changed from 0.0072 per 100,000 people in 1978 to 0.0430 in 1981, with an annual percent change (APC) of 23.23 and then dropped to 0.0272 in 2013 with an APC of –3.09 (95% CI=–4.9 to –1.3, P<0.05), demonstrating no significant change from 1981 to 2013 ().
Figure 1 The incidence of extragonadal choriocarcinoma in male from 1978 to 2013.
Notes: Annual age-adjusted rates of extragonadal choriocarcinoma in male by year (1973–2013). The incidence is presented as the number of patients per 100,000 age-adjusted for the 2000 US standard population.
Patient demographics
From 1973 to 2013, 197 cases of extragonadal choriocarcinoma in males were identified in the SEER database. Patient demographics and clinical characteristics of the study population are summarized in . The median age of diagnosis was 30 years with a range of 0–84 years and percentile of 21–46 years. The most common primary tumor location was the mediastinum, with 44.8% of cases occurring in this location (n=30), followed by the retroperitoneum and the brain. Other tumor sites included the liver (n=2), intrahepatic bile duct (n=1), nasal cavity (n=1), subcutaneous connective tissue (n=2), adrenal gland (n=1) and abdomen (n=1).
Table 1 Demographics and clinical characteristics
Treatment
The ratio of patients who received beam radiation therapy was 22.8% for the whole cohort but was lower in older patients and European-Americans, and the ratio receiving surgery was 63.5% overall, which has decreased over the last decades. Among the tumors located at different sites, brain tumor patients were more prone to receive beam radiation, and mediastinum tumor patients were less likely to receive surgery. The treatment characteristics of the cohort are shown in .
Table 2 Treatment characteristics of choriocarcinoma out of testicle in males
Survival
The median follow-up time was 9 months (with a range of 0–427 months). The median survival time of the cohort was 11 months (95% CI: 5.7 to 16.3 months), whereas the estimated 1-, 3- and 5-year overall survival rates were 46%, 33% and 31%, respectively. The estimated 1-, 3- and 5-year CSS rates were 49%, 37% and 35%, respectively.
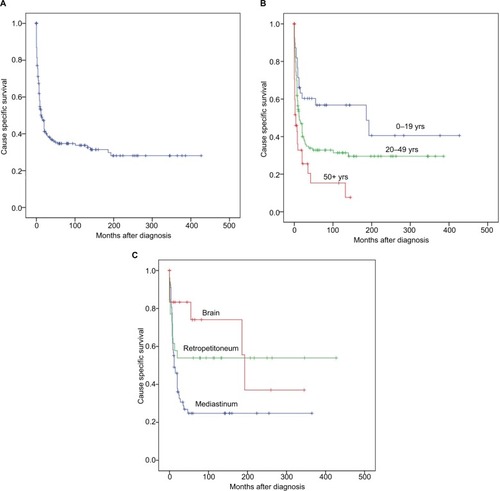
The multivariate analysis showed that the age at diagnosis and primary site were the independent prognostic factors (). First, age at diagnosis was related to prognosis in the univariate CSS analysis. Compared with older patients, younger patients were significantly correlated with a favorable prognosis of survival. The median survival time () was 186 months for the 0- to 19-year-old patients; 13 months in the 20- to 49-year-old patients; and only 4 months in patients aged 50+ years. The multivariate analysis showed that age at diagnosis was an independent prognostic factor. In addition, the brain as the primary site was related to a favorable prognosis in both univariate and multivariate analyses. The median survival time was 193 months for brain tumors and 12 months for mediastinum tumors.
Table 3 Univariate and multivariate survival analyses for evaluating the prognostic factor of choriocarcinoma out of testis in males
Figure 2 Plots of cause-specific survival (CSS) duration.
Notes: (A) CSS for the cohort of extragonadal choriocarcinoma in male. (B) CSS by age of diagnosis. Patients were separated into three groups by age of diagnosis. Five-year CSS was 57%, 33% and 15% for those diagnosed among 0–19 years, 20–49 years and 50+ years (P<0.05), respectively. (C) CSS by primary site. Selected patients were separated into three groups by the primary site of tumor. Five-year CSS was 25%, 54%, and 71% for patients of mediastinum, retroperitoneum, and brain tumors.
The variables of diagnosis year and marital status were related to prognosis in our univariate analysis but were not identified as independent prognostic factors in our multivariate analysis. For year of diagnosis, the survival rate tended to increase along decades, and the median survival times were 5, 10, 13 and 20 months in 1973–1982, 1983–1992, 1993–2002 and 2003–2013, respectively. For marital status, we found married patients were related to an unfavorable prognosis in the univariate analysis, but the multivariate analysis excluded it as an independent prognostic factor. To elucidate the reason, we compared the age at diagnosis in married patients with the other marital categories using the t-test. The results showed a significantly younger age at diagnosis in married patients than the other marital categories (28.0±16.5 years vs 44.9±15.0 years, P=0.000).
Other variables, such as ethnicity and therapeutic treatment (ie, surgery vs beam radiation), were not prognostic factors in the multivariate analysis. First, ethnicity was not correlated to prognosis, despite a worse prognosis for African-American patients when compared with European-American patients or others. Second, surgery and beam radiation treatments were not correlated to prognosis. In fact, the number of surgeries dropped from 77.4% in 1973–1999 to 51.0% in 2000–2013, P=0.000. However, the percentage of beam radiation cases was similar at 19.4% and 26.0% in the previous and current centuries, respectively (P=0.270).
Discussion
In the present study, we took advantage of the large data set from the SEER Program to investigate the incidence and prognostic factors in the largest series of extragonadal choriocarcinoma in males reported to date. The retrospective study showed that the rates of beam radiation and surgery cases were 22.8% and 63.5%, respectively, and the 5-year CSS rate was 35%. The age at diagnosis and primary site were the independent prognostic factors.
Despite the multiple hypotheses of tumor development, choriocarcinoma is a rare neoplasm, and to the best of our knowledge, the incidence of extragonadal choriocarcinoma in males was first reported in a population-based cohort. Most importantly, according to data collected by Jiang et al,Citation16,Citation17 gestational choriocarcinoma affected 1–9.2 in 40,000 pregnancies and 1 in 40 hydatidiform moles, and the inci dence ratio of gestational choriocarcinoma to nongestational choriocarcinoma was 79:1, with a male-to-female ratio of 13:33 among patients with nongestational choriocarcinoma. Moreover, nongestational choriocarcinoma in males has been reported at variable anatomical sites with the most occurring in the testes. A total of 106 cases of male choriocarcinoma were reviewed between 1995 and 2006 by Yokoi et al, and the testes were the most common primary tumor site accounting for 33% (35/106).Citation18 However, testicular choriocarcinoma represents only less than 1% of all germ cell tumors.Citation2,Citation19 Interestingly, extragonadal germ cell tumors occur more frequently in the Korean population than in western countries, and the authors considered genetic and dietary factors as possible explanations for the difference.Citation20 The extragonadal germ cell tumor rate among males in the USA is 1.82 times higher than that in Europe, and the authors think that miscoding of registries could be a likely explanation.Citation8,Citation9 However, choriocarcinoma was not specified in these studies and was merely described in case reports. For example, the primary mediastinal choriocarcinoma was first described by Arendt in 1931, and only 43 subsequent reports were found by 2014.Citation3 Zhu et al’s literature review of primary pulmonary choriocarcinoma in males reflected only 29 cases reported by 2016.Citation5 In our study, the incidence of extragonadal choriocarcinoma in males estimated by SEER data was 0.022/100,000 people, and the incidence decreased from 1981.
Extragonadal choriocarcinoma occurs more frequently in younger male patients rather than in older male patients, and furthermore, younger age is a prognostic factor. On the one hand, although there are potentially different mechanisms of development between testicular and extragonadal choriocarcinoma, we found a similar age in peak incidence between the two. The highest incidence of testicular cancer in the USA is between 20 and 34 years old, and the majority of new testicular choriocarcinoma cases develop between 25 and 30 years of age.Citation14 In our study, the peak incidence of extragonadal choriocarcinoma in males was 20–29 years old, and the majority was younger than 50 years. These findings are in agreement with a literature review involving 41 cases of primary mediastinal choriocarcinoma, which is usually diagnosed in young patients aged between 20 and 30 years old.Citation3 However, 26 cases of primary choriocarcinoma of the bladder and 53 cases of primary gastric choriocarcinoma reported in the literature showed that the majority of patients were diagnosed at 50+ years of age, and Serno et al found that the median age of male primary pulmonary choriocarcinoma was 60 years.Citation6,Citation21,Citation22 Therefore, we speculate that choriocarcinoma at midline locations mainly occurs in young patients, while choriocarcinoma of parenchymal organs tends to affect older patients. On the other hand, our data show that patients who are younger than 20 years have a favorable prognosis. Similarly, Jiang et al analyzed 13 cases of male primary choriocarcinoma reported from the medical center and 100 cases from the scientific literature, and discovered that patients not older than 34 years had significantly longer survival rates.Citation17 In fact, the International Federation of Gynecology and Obstetrics 2000 prognostic scoring system was widely used to estimate the prognosis for gestational trophoblastic neoplasia, and age is a prognostic factor.Citation23 A recent study found that age, ethnicity and tumor stage were independent predictors of mortality of gestational choriocarcinoma.Citation24 Therefore, the findings imply that age is a critical prognostic factor for choriocarcinoma.
Taken together, the tumorigenesis and prognosis of younger patients seem different from those of older patients, and these findings indicate that more detailed research should be undertaken in the context of pathology and molecular genetics.
In our study, the most common sites of extragonadal choriocarcinoma in males were the mediastinum, retroperitoneum and brain, among which the brain is the primary site directly correlated to a favorable prognosis. Interestingly, the incidence in anatomical locations of extragonadal choriocarcinoma was slightly different from the case series. Yokoi et al described the largest series of 106 cases of male choriocarcinoma reported during 1995–2006, and in addition to testes, the mediastinum, pineal body, gastrointestinal tract, lungs and retroperitoneum were the most common sites; similar results were described by Jiang et al in 2014.Citation17,Citation18 Publication bias was inevitable because a literature review of previously published case reports formed the majority of data in both studies. However, the present population-based study provides an overall view of the extragonadal choriocarcinoma in males. Additionally, although choriocarcinoma of the brain was correlated to a favorable prognosis compared with that of the mediastinum, it could be fatal in more than half the patients. A previous study that included intracranial choriocarcinoma in men and women found that the 1-year survival rate was 61.2%, and the prognosis of male patients was better than that of females.Citation25 Choriocarcinoma is the rarest and most malignant of primary intracranial germ cell tumors, accounting for ~3%–5% of all intracranial GCTs, and germ cell tumors comprised 3%–11% of all intracranial neoplasms in children and 1% of all primary intracranial neoplasms in adults.Citation26,Citation27 The most common sites of intracranial choriocarcinoma are the pineal and suprasellar regions. Characteristic clinical features include tumor hemorrhage, extraneural and cerebrospinal fluid metastasis, and fetal problems of intracranial choriocarcinoma; these features contribute to its poor prognosis.Citation25
The treatment for primary choriocarcinoma has remained unclear without any standard strategies, and no clinical trial has been reported because of the rarity of this disease; therefore, clinicians often provide patients with surgery, chemotherapy and radiotherapy as choices for treatment.Citation28 Surprisingly, our study did not find that beam radiation or surgery could prolong survival, and further analysis showed that neither radiotherapy nor surgery could prolong survival in a subgroup of intracranial tumors. However, a previous literature review based on 66 reported cases in 1975–2004 revealed that surgery, radiotherapy and chemotherapy were independent prognostic factors in primary intracranial choriocarcinoma/germ-cell tumors with high levels of human chorionic gonadotropin (HCG), although the case selection bias and different treat ment protocols should not be overlooked.Citation25 We believe that the treatment efficacy can be omitted in our study because of the limited number of cases. Therefore, we conclude that the best management is based on multidisciplinary therapy, and multicenter clinical trials should be encouraged.
The limitations of this current study include the following: 1) the lack of central verification of pathology diagnosis; 2) the unavailability of information of treatment such as chemotherapy and surgical margin in the SEER database, which may be a critical prognostic factor; 3) the lack of information of biomarkers, such as HCG; 4) and the relatively small sample size, which may still not be enough to fully illustrate the incidence, treatment and prognosis of this rare tumor.
Conclusion
The present study suggests that extragonadal choriocarcinoma in males is a rare malignancy with a poor prognosis. However, a young age at diagnosis and the brain as the primary tumor site were the independent prognostic factors.
Acknowledgments
This work was not supported by any organization. This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- SchmollHJExtragonadal germ cell tumorsAnn Oncol200213Suppl 426527212401700
- ChengLLyuBRothLMPerspectives on testicular germ cell neoplasmsHum Pathol201759102527569298
- ZhangSGaoHWangXAPrimary choriocarcinoma in mediastinum with multiple lung metastases in a male patient: a case report and a review of the literatureThorac Cancer20145546346726767039
- JiangLWuJTPengXPrimary choriocarcinoma of the colon: a case report and review of the literatureWorld J Surg Oncol2013112323356395
- ZhuRJiaCYanJLuoYHuoZPrimary pulmonary choriocarcinoma in a male that was successfully diagnosed and treated: A case report and review of the literatureMedicine20169552e569328033262
- MonnMFJaquaKRBihrleRChengLPrimary Choriocarcinoma of the Bladder: A Case Report and Review of LiteratureClin Genitourin Cancer201715218819127793609
- ZhuYLiuMLiJBreast carcinoma with choriocarcinomatous features: a case report and review of the literatureWorld J Surg Oncol20141223925073898
- StangATrabertBWentzensenNBurden of extragonadal germ cell tumours in Europe and the United StatesEur J Cancer20124871116111722425262
- TramaAMalloneSNicolaiNBurden of testicular, paratesticular and extragonadal germ cell tumours in EuropeEur J Cancer201248215916922142457
- IkuraYInoueTTsukudaHYamamotoTUedaMKobayashiYPrimary choriocarcinoma and human chorionic gonadotrophin-producing giant cell carcinoma of the lung: are they independent entities?Histopathology2000361172510632747
- WangLYamaguchiSBursteinMDNovel somatic and germline mutations in intracranial germ cell tumoursNature2014511750824124524896186
- CheungANZhangHJXueWCSiuMKPathogenesis of choriocarcinoma: clinical, genetic and stem cell perspectivesFuture Oncol20095221723119284380
- StangATrabertBWentzensenNGonadal and extragonadal germ cell tumours in the United States, 1973-2007Int J Androl201235461662522320869
- ReilleyMJPagliaroLCTesticular choriocarcinoma: a rare variant that requires a unique treatment approachCurr Oncol Rep2015172225645112
- KimHJFayMPFeuerEJMidthuneDNPermutation tests for joinpoint regression with applications to cancer ratesStat Med200019333535110649300
- LurainJRGestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform moleAm J Obstet Gynecol2010203653153920728069
- JiangFXiangYFengFZRenTCuiZMWanXRClinical analysis of 13 males with primary choriocarcinoma and review of the literatureOnco Targets Ther201471135114125018640
- YokoiKTanakaNFurukawaKMale choriocarcinoma with metastasis to the jejunum: a case report and review of the literatureJ Nippon Med Sch200875211612118475033
- HumphreyPAChoriocarcinoma of the testisJ Urol2014192393493524949806
- ParkDSChungMKChungJIHistologic type, staging, and distribution of germ cell tumors in Korean adultsUrol Oncol200826659059418367106
- KobayashiAHasebeTEndoYPrimary gastric choriocarcinoma: two case reports and a pooled analysis of 53 casesGastric Cancer20058317818516086121
- SernoJZeppernickFJäkelJPrimary pulmonary choriocarcinoma: case report and review of the literatureGynecol Obstet Invest201274217117622738859
- NganHYBenderHBenedetJLGestational trophoblastic neoplasia, FIGO 2000 staging and classificationInt J Gynaecol Obstet200383Suppl 117517714763174
- TarneyCMTianCCraigERRelative effects of age, race, and stage on mortality in gestational choriocarcinomaInt J Gynecol Cancer201828233834529232272
- ShinodaJSakaiNYanoHHattoriTOhkumaASakaguchiHPrognostic factors and therapeutic problems of primary intracranial choriocarcinoma/germ-cell tumors with high levels of HCGJ Neurooncol2004661–222524015015791
- KyritsisAPManagement of primary intracranial germ cell tumorsJ Neurooncol201096214314919588227
- HoffmanHJOtsuboHHendrickEBIntracranial germ-cell tumors in childrenJ Neurosurg19917445455511848284
- KregeSBeyerJSouchonREuropean consensus conference on diagnosis and treatment of germ cell cancer: a report of the second meeting of the European Germ Cell Cancer Consensus group (EGCCCG): part IEur Urol200853347849618191324