
Abstract
Background
We performed a network meta-analysis of randomized controlled trials (RCTs) to indirectly compare the efficacy of different targeted agents with fulvestrant for patients with hormone-receptor-positive (HR+) and human epidermal growth factor receptor type 2-negative (HER2–) advanced breast cancer (ABC) following progression on prior endocrine therapy.
Methods
The titles/abstracts were searched from the PubMed, EMBASE, and the Cochrane Library databases for RCTs to evaluate the efficacy of palbociclib plus fulvestrant vs alternative targeted therapies plus fulvestrant for postmenopausal HR+/HER2– ABC following progression on prior endocrine therapy. In addition, the primary measured outcome was progression-free survival (PFS) and objective response rate. The surface under the cumulative ranking (SUCRA) value of each treatment was calculated to achieve the best ranking for each treatment.
Results
A total of 11 studies, including 4,178 patients in the network meta-analysis, were included and analyzed. In terms of the pooled hazard ratios (HRs) for PFS, palbociclib plus fulvestrant was superior to other target agents plus fulvestrant (HR=0.62, 95% credible interval [CrI]: 0.40–0.96; HR=0.62, 95% CrI: 0.47–0.96; for pictilisib plus fulvestrant and buparlisib plus fulvestrant, respectively). Ribociclib plus fulvestrant has no difference in abemaciclib plus fulvestrant and palbociclib plus fulvestrant (HR =1.02, 95% CrI =0.72–1.45; HR =1.22, 95% CrI =0.84–1.78). In terms of objective response rate, compared with placebo plus fulvestrant, abemaciclib plus fulvestrant, dovitinib plus fulvestrant, buparlisib plus fulvestrant, and palbociclib plus fulvestrant had a significant difference (odds ratio [OR] =2.84, 95% CrI =1.91– 4.31; OR =3.62, 95% CrI =1.21–12.48; OR =1.80, 95% CrI =1.25–2.60; and OR =2.52, 95% CrI =1.43– 4.72, respectively).
Conclusion
According to the present study, palbociclib plus fulvestrant may be the optimal treatment for HR+/HER2– postmenopausal women with ABC after disease progression following endocrine therapy.
Introduction
Breast cancer is the most common malignant disease in women and its incidence increases in postmenopausal individuals.Citation1 Among the postmenopausal patients with advanced breast cancer (ABC; locally advanced or metastatic), the majority are hormone receptor positive (HR+) and human epidermal growth factor receptor type 2 negative (HER2–).Citation2–Citation4 At present, endocrine therapy plays a crucial part in HR+/HER2– ABC. There are three types of commonly used endocrine therapy drugs: selec tive estrogen-receptor modulators, aromatase inhibitors (AIs), and selective estrogen-receptor downregulators.Citation5 Previous meta-analysis have demonstrated that AIs are more effective than tamoxifen in postmenopausal women with ABC in terms of objective response rate (ORR) and complete response (CR).Citation6 However, therapeutic options for patients who failed after tamoxifen or AI treatment are unclear. Fulvestrant is a selective estrogen-receptor downregulator different from other endocrine agents. It binds with 100-fold greater affinity than tamoxifen, and in terms of inhibiting estrogen signaling, it is more effective than tamoxifen and AIs.Citation7–Citation9 These evidence suggested that it could be a better platform for combination with other targeted pathways. The Phase III EFECT trial showed that fulvestrant loading dose (loading dose is 500 mg on day 0, 250 mg on days 14 and 28, and 250 mg every 28 days thereafter) was as effective as exemestane for postmenopausal women with ABC who have experienced progression or recurrence during treatment with a nonsteroidal AIs.Citation10 The CONFIRM and FINDER2 trials demonstrated that fulvestrant 500 mg has efficacy superior to fulvestrant 250 mg in treatment for estrogen-receptor positive (ER+) ABC with progression after previous endocrine therapy.Citation11–Citation13 Therefore, for patients who experience disease progression after tamoxifen or AI therapy, fulvestrant could be a second-line therapeutic option.Citation14 Fulvestrant monotherapy was used to treat HR+ABC patients with good tolerance but limited efficacy.Citation11,Citation15 With the application of fulvestrant in HR+/HER2– ABC patients, numerous new targeted agents in combination with fulvestrant are in clinical development, providing therapeutic options for patients with endocrine resistance. For instance, the combination of palbociclib and fulvestrant was associated with greater median progression-free survival (PFS) compared with fulvestrant plus placebo (9.5 vs 4.6 months; hazard ratio [HR] =0.46, 95% CI =0.36–0.59, P<0.0001) for patients with metastatic breast cancer who had progressed on previous endocrine therapy.Citation15 Furthermore, the Food and Drug Administration approved palbociclib for use in combination with fulvestrant for the treatment of women with HR+/HER2– advanced or metastatic breast cancer with disease progression following endocrine therapy.Citation16 Undeniably, previous network meta-analysisCitation17 has compared the efficacy of endocrine-based therapies following progression on nonsteroidal AI in patients with postmenopausal HR+/HER2– metastatic breast cancer. The result strongly demonstrated that in this circumstance, patients who received palbociclib plus fulvestrant, everolimus plus AI, or everolimus plus fulvestrant prolonged PFS compared with those who received fulvestrant or AI alone.
So far, there has been no direct comparison between palbociclib plus fulvestrant vs other targeted therapies plus fulvestrant for patients with HR+ ABC following progression or recurrence on prior endocrine therapy. Thus, a summary of these trials is needed. The purpose of the present study was to perform a network meta-analysis of the existing literature to indirectly compare the efficacy of different targeted agents with fulvestrant as a second-line therapy for HR+/HER2– ABC.
Materials and methods
Literature and search strategy
The network meta-analysis was designed, and the trial was reported, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension to network meta-analysis.Citation18
We searched the titles/abstracts from the following databases inception to June 5, 2018: PubMed, EMBASE, and the Cochrane Library. We used the Medical Subject Headings/Emtree terms combined with keywords properly adjusted for the different databases in all the search strategies. Detailed information on the search strategies of different databases is provided in Supplementary materials. The network meta-analysis was only restricted to articles of randomized controlled trials (RCTs) published in the English language. For a more comprehensive search strategy and to identify more relevant literature, we manually searched the reference lists of multiple articles, including published meta-analysis and reviews.
Selection criteria
Included participants were HR+/HER2– women with ABC who have progressed or recurrence after previous endocrine therapy or targeted therapy. The type of intervention was fulvestrant plus any of the following treatments: palbociclib, abemaciclib, buparlisib, dovitinib, ribociclib, vandetanib, and everolimus, pictilisib, bortezomib, selumetinib, and placebo. Eligible studies were RCTs that assessed the effectiveness of fulvestrant plus any targeted therapy. The main outcomes were PFS and ORR. Studies involving loading dose of fulvestrant (loading dose is 500 mg on day 0, 250 mg on days 14 and 28, and 250 mg every 28 days) were excluded. We also excluded these studies of fulvestrant plus targeted therapy used as adjuvant treatment. If several articles were based on the same trial, then only the most informative study and/or the primary publication of the results was included in the present network meta-analysis.
Two investigators (TT Zhang and FB Feng), working independently, scanned all titles and abstracts, excluding obviously unmatched articles, and the remaining full texts were read for further identification. For any discrepancies between authors, a third author provided arbitration (Y Yao).
Data extraction and quality assessments
Two authors (CX Zang and WG Zhao) independently extracted the data from eligible studies by using a predefined and standard data form based on Excel spreadsheet. Data were extracted on an intention-to-treat basis. For crossover trials, only first period data were extracted. The information of studies that met the inclusion criteria was extracted as follows: first author’s name, year of publication, pathway inhibited, disease stage, characteristics of trial participants (median age, postmenopausal status, HR status, prior endocrine therapy, Eastern Cooperative Oncology Group performance status, median follow-up), type of treatment (type, dose, duration, and frequency), and primary outcomes. The primary outcomes in the present study were PFS and ORR. After extracting all the information, the two authors crosschecked the extracted information to guarantee accuracy of the information.
The quality of studies was evaluated by two authors (Y Yao and WG Zhao) by using the Cochrane Collaboration’s tool for assessing risk of bias evaluating six domainsCitation19: 1) selection bias, 2) performance bias, 3) detection bias, 4) attrition bias, 5) reporting bias, and 6) other bias. The studies were judged as unclear, high risk, or low risk of bias. Two authors independently extracted the data and assessed risk of bias, and any discrepancies between the two authors were resolved by consensus through discussion.
Statistical methods
The HR was ultimately utilized for pooling effect sizes because the outcome was time-to-event outcomes. We mainly derived the digitized HR and the corresponding of 95% CI from publications. If the HR is not given in the publications directly, the Engauge Digitizer 4.1 (http://digitizer.sourceforge.net/) is used to extract the survival information from the Kaplan–Meier curve.Citation20 Additionally, the odds ratio (OR) was utilized for pooling effect sizes for ORR. If only the percentage of ORR is reported in the article, we need to convert it to decimal to carry out four rounds of five entries.
To ensure that all data were normally distributed, we used the log HR for analysis and a Bayesian approach to evaluate efficacy, according to Welton et al.Citation21 It applies to ORR as well. Furthermore, the model parameter was conducted using the Markov chain Monte Carlo technique with WinBUGS version 1.4.3 (MRC Biostatistics Unit, Cambridge, UK). The WinBUGS sampler was run with three chains using randomly different chosen initial values for 10,000 iterations after a burn-in of 5,000. According to the Deviance Information Criteria (DIC) value, we selected a fixed model or random model. The smaller the DIC value, the more suitable the model.
The summary treatment effect size (HR or OR), as a point estimate, was considered as the median of the posterior distribution, and a 95% credible interval (CrI), which derived from the 2.5 and 97.5 percentiles, was presented. We judged whether it was meaningful or not according to whether the 95% CrI was included. In addition, we adopted the surface under the cumulative ranking (SUCRA) value to rank all treatments. Finally, we used these SUCRAs to determine which is the best treatment. The SUCRA is closer to 100, indicating that it is in the first place. If a loop connecting three arms existed, a node-splitting approach was adopted to assess the inconsistency among direct and indirect evidence.
The risk of bias in individual studies was assessed by Review Manager, version 5.3 (The Nordic Cochrane Centre: The Cochrane Collaboration, Copenhagen, Norway). A network of different interventions was plotted, and the SUCRA was calculated by STATA, version 13.0 (Stata Corporation, College Station, TX, USA).
Results
Overview of the literature search
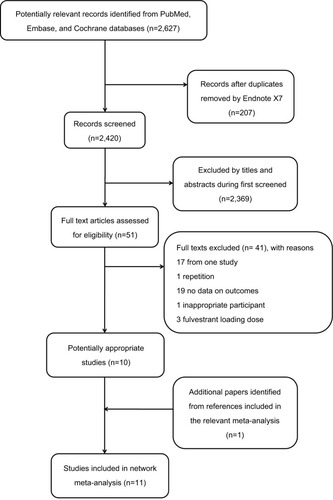
A total of 2,627 articles were identified, among which 207 records were duplicates. After screening the titles and abstracts, 2,369 studies were discarded because they obviously did not meet the predefined inclusion criteria. By reviewing the full text, we further excluded 41 publications for the following reasons: 17 papers were derived from one study, 1 paper was repetitive, 19 papers did not report relevant outcomes on data, 3 papers used the loading dose of fulvestrant, and 1 paper had no appropriate participants. Furthermore, we obtained an eligible paper by tracking relevant references manually. Ultimately, 11 eligible papers were included in the present study.Citation15,Citation22–Citation31 The details of the study selection and the results are shown in .
Figure 1 Flowchart for search results and selection details.
Characteristics of included studies
All trials were multicenter and only had two groups. The 11 papers included 11 trials and comprised 4,178 patients with advanced or locally advanced or metastatic breast cancer. The majority of trials are compared with placebo plus fulvestrant; however, oneCitation30 of the trials is compared with fulvestrant alone. The publication time of the included studies ranged from 2014 to 2018. The median ages were between 56 and 69 years across all studies. The percentage of ER+/progesterone-receptor positive patients ranged from 10% to 100%. Moreover, regarding the percentage of postmenopausal status, only two papers reported the specific percentage, which ranged from 79% to 83.2%, and the remaining papers did not report the specific percentage. In previous endocrine therapy, the included participants had received AIs and/or tamoxifen therapy. The median PFS is from 2.69 to 20.3 months. The characteristics of the eligible studies are summarized in . Detailed information is shown in Supplementary materials.
Table 1 Characteristics of the 11 studies included in the network meta-analysis
The assessment of the risk of bias
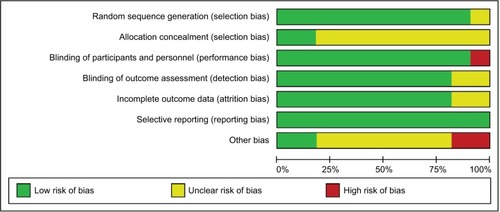
The risk of bias of individual studies included in the present network meta-analysis is presented in . In general, the included studies were high quality in methodological. The majority of studies had reported random sequence generation. In addition to one study, the remaining studies did not explicitly propose specific ways to allocate concealment. Eight trials were funded by pharmaceutical companies. All included studies did not report selectively.
Figure 2 Cochrane risk of bias tool assessment (green: low risk of bias; red: high risk of bias; and yellow: unclear risk of bias).
Network meta-analysis
The evidence network of eligible comparisons is shown in , of which the network of PFS is shown in , and the network of ORR is shown in . The combination of fulvestrant plus placebo was the most frequently investigated regimen (11 comparisons). This regimen was respectively compared with abemaciclib plus fulvestrant, dovitinib plus fulvestrant, everolimus plus fulvestrant, buparlisib plus fulvestrant, pictilisib plus fulvestrant, palbociclib plus fulvestrant, vandetanib plus fulvestrant, ribocilib plus fulvestrant, bortezomib plus fulvestrant, and selumetinib plus fulvestrant. As is demonstrated in , there is no closed loop. Therefore, consistency check is not performed.
Figure 3 Network of eligible comparisons for network meta-analysis for PFS (A) and ORR (B).
Abbreviations: FP, placebo+fulvestrant; ORR, objective response rate; PFS, progression-free survival.
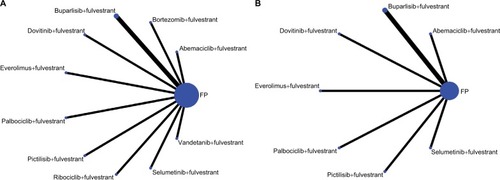
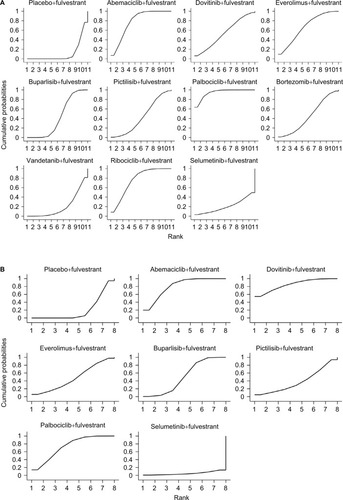
Figure 4 The SUCRA for PFS (A) and ORR (B). The SUCRA value of interventions is closer to 100, indicating that it is always in the first place, and if it is close to 0, it is always at the end.
Abbreviations: ORR, objective response rate; PFS, progression-free survival; SUCRA, surface under the cumulative ranking.
PFS was reported as a primary outcome in all 11 studies. The network meta-analysis results were based on a fixed-effect model because there was no significant difference of the DIC between the fixed-effects model (DIC =1.954) and the random-effects model (DIC =2.779). Among which, compared with placebo plus fulvestrant, palbociclib plus fulvestrant, ribociclib plus fulvestrant, abemaciclib plus fulvestrant, everomilus plus fulvestrant, and buparlisib plus fulvestrant had a significant advantage (HR =0.46, 95% CrI =0.36–0.59; HR =0.56, 95% CrI =0.43–0.74; HR =0.55, 95% CrI =0.45–0.68; HR =0.61, 95% CrI =0.40–0.93; and HR =0.74, 95% CrI =0.66–0.84, respectively). Palbociclib plus fulvestrant was superior to other target agents plus fulvestrant (HR =0.62, 95% CrI =0.40–0.96; HR =0.62, 95% CrI =0.47–0.96 for pictilisib plus fulvestrant and buparlisib plus fulvestrant, respectively). Burparlisib plus fulvestrant and vandetanib plus fulvestrant were inferior to abemaciclib plus fulvestrant (HR =1.34, 95% CrI =1.06–1.71 and HR =1.69, 95% CrI =1.10–2.62, respectively). Ribociclib plus fulvestrant has no difference in abemaciclib plus fulvestrant and palbociclib plus fulvestrant (HR =1.02, 95% CrI =0.72–1.45; HR =1.22, 95% CrI =0.84–1.78). ORR was reported as a primary outcome in all eight studies. The network meta-analysis results were based on fixed-effect model (DIC =101.099) rather than random-fixed model (DIC =101.299). Abemaciclib plus fulvestrant, dovitinib plus fulvestrant, buparlisib plus fulvestrant, and palbociclib plus fulvestrant had a significant difference (OR =2.84, 95% CrI =1.91–4.31; OR =3.62, 95% CrI =1.21–12.48; OR =1.80, 95% CrI =1.25–2.60; and OR =2.52, 95% CrI =1.43–4.72, respectively) when compared with placebo plus fulvestrant. Selumetinib plus fulvestrant was inferior to abemaciclib plus fulvestrant, dovitinib plus fulvestrant, and palbociclib plus fulvestrant (OR =0.08, 95% CrI =0.00–0.80; OR =0.06, 95% CrI =0.00–0.77; and OR =0.08, 95% CrI =0.00–0.92, respectively). More network meta-analysis results of PFS and ORR are summarized in .
Table 2 Network meta-analysis of 11 targeted therapies plus fulvestrant for PFS and ORR
The SUCRAs for the outcomes of PFS in the network meta-analysis are shown in . Moreover, the size of SUCRA value determined which treatment is the best. Palbociclib plus fulvestrant had the biggest SUCRA (SUCRA =94.2%), suggesting that this regimen may be the optimal treatment in terms of PFS. The second highest percentage of treatment was the combination of abemaciclib and fulvestrant (SUCRA =78.1%), followed by ribociclib plus fulvestrant (SUCRA =75.3%), everolimus plus fulvestrant (SUCRA =66.3%), and dovitinib plus fulvestrant (SUCRA =53.4%). The SUCRAs for the outcomes of ORR in the network meta-analysis are shown in . In terms of ORR, dovitinib plus fulvestrant may be the optimal treatment because it has the biggest SUCRA (SUCRA =84.7%). The ranks of second and third are abemaciclib and fulvestrant (SUCRA =80.6%) and palbociclib plus fulvestrant (SUCRA =73.0%).
Discussion
The use of endocrine therapy for the treatment of HR+/HER2– postmenopausal women with ABC has been well established. Clinically, resistance to endocrine therapies is also common in HR+/HER2− disease, and most patients inevitably face disease progression.Citation32 However, for postmenopausal women with HR+/HER2– ABC who previously failed after prior endocrine therapy, the optimal sequence of endocrine treatment remains unclear. Here, we performed a network meta-analysis on the efficacy of the available studies involving different targeted therapy with fulvestrant as a second-line therapy for HR+/HER2– ABC.
According to our network meta-analysis, we derived the following findings in the present analysis: the combination of palbociclib plus fulvestrant significantly improved PFS when compared with fulvestrant plus placebo and abemaciclib plus fulvestrant also improved PFS when compared with fulvestrant plus placebo, but to a lesser degree. However, palbociclib plus fulvestrant had not significantly prolonged PFS comparing with abemaciclib plus fulvestrant. As far as we are concerned, dovitinib plus fulvestrant was more effective than other targeted therapies plus fulvestrant in terms of ORR.
In this case, the combination of endocrine therapy and targeted agents (eg, palbociclib, abemaciclib) to block cell signaling pathways that interact with the ER increased clinical benefits compared with single endocrine therapy.Citation15,Citation31,Citation33 Furthermore, a previous report indicated that estrogen activity and cyclin-dependent kinase (CDK) 4/6/retinoblastoma protein pathway activity are closely related.Citation34 Palbociclib, a selective CDK4/6 inhibitor, preferentially inhibited the proliferation of ER+ cancer cells in preclinical studies.Citation35 A Phase III randomized trial indicated that the combination of palbociclib and fulvestrant could be considered as an option for patients with HR+/HER2– ABC who have progressed on prior endocrine therapy.Citation15 Moreover, in a previous network meta-analysis, we found that the combination of palbociclib plus fulvestrant was associated with longer PFS than single endocrine therapies, such as anastrozole, letrozole, exemestane, and megestrol acetate.Citation36 Following failure on previous endocrine therapy, many patients are offered chemotherapy as a second-line therapeutic option.Citation3 However, the combination of palbociclib plus fulvestrant also improved PFS relative to all other chemotherapy treatments.Citation37 Furthermore, endocrine therapy has a lower toxicity than chemotherapy. But due to the same signal pathway of palbociclib and abemeciclib, they may be no significant difference in prolonging PFS..
In addition, dovitinib plus fulvestrant is more effective than other targeted therapis plus fulvestrant. Dovitinib belongs to a small molecule inhibitor of fibroblast growth factor receptor 1 (FGFR1), FGFR2, and FGFR3.Citation38 The abnormal regulation of FGF and FGFR signals is associated with oncogenesis activity,Citation39 increases the risk of developing breast cancer,Citation40–Citation42 and is related to the resistance to endocrine therapy.Citation43 In addition to inhibiting cell proliferation, dovitinib also showed antineoplastic activity in FGFR-amplified xenograft models.Citation44 This difference in signal transduction pathway may be responsible for the difference between dovitinib and palbociclib on the basis of ORR.
Previous meta-analysis showed that fulvestrant plus targeted therapies showed ORR and PFS benefit in patients with ABC.Citation45 However, different doses of fulvestrant on the effects of combined therapy were not considered in that study, and as a result, there may be greater heterogeneity. In the present study, we only included trials on high dose of fulvestrant, which ruled out the effect of different doses of fulvestrant on results. Furthermore, in terms of PFS and ORR, we ranked different targeted agents plus fulvestrant to determine the optimal treatment. To our knowledge, there are currently no head-to-head trials evaluating the efficacy of different targeted therapies in combination with fulvestrant in patients who experienced disease progression on prior endocrine therapy. The present network meta-analysis indirectly compared different targeted therapies in combination with fulvestrant. Thus, the present study could provide the higher level of evidence for physicians and patients. The network meta-analysis provided an insight into the use of fulvestrant combined with different targeted agents for patients with HR+/HER2– ABC following failure on prior endocrine therapy. However, there are also several limitations in the present study. First, for all treatment comparisons in the present network meta-analysis, no direct evidence was available and thus, it was impossible to evaluate incoherence (ie, the extent of disagreement between direct and indirect evidence). Second, adverse events of targeted agents varied across trials. The assessment of adverse events is relative to the acceptability of patients, and unfortunately, the collected data did not facilitate an evaluation of the adverse events; thus, the toxicity of the targeted agents was ultimately not evaluated. Third, only a limited number of regimens (n=11) and trials (n=11) were included, and the combination of palbociclib plus fulvestrant has only been reported in one study, thereby weakening the validity of the present analysis.
Conclusion
The present study showed that palbociclib plus fulvestrant may be the optimal treatment for HR+/HER2–postmenopausal women with ABC after disease progression following endocrine therapy. However, direct comparisons are still needed to examine differences among different targeted agents plus fulvestrant.
Acknowledgments
The authors would like to acknowledge Dr Shengjie Dong and all the members of Department of Oncology of Weifang Traditional Chinese Hospital.
This study was supported by grants from the National Natural Science Foundation of China (numbers 81473513 and 81673799).
Author contributions
Changgang Sun, Tingting Zhang, and Fubin Feng were involved in the concept and design of the study. Tingting Zhang drafted the manuscript. All authors were involved in acquisition, analysis, and interpretation of the data, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- Stat Fact Sheets SEFemale breast cancer2017 Available from: seer.cancer.gov/statfacts/html/Breast/Assessed January 16, 2018
- CardosoFCostaANortonLESO-ESMO 2nd international consensus guidelines for advanced breast cancer (ABC2)Ann Oncol201425101871188825234545
- MigliaccioIMalorniLHartCDGuarducciCDi LeoAEndocrine therapy considerations in postmenopausal patients with hormone receptor positive, human epidermal growth factor receptor type 2 negative advanced breast cancersBMC Med2015134625857348
- JoyAAGhoshMFernandesRClemonsMJSystemic treatment approaches in her2-negative advanced breast cancer-guidance on the guidelinesCurr Oncol201522Suppl 1S29S4225848337
- FanWChangJFuPEndocrine therapy resistance in breast cancer: current status, possible mechanisms and overcoming strategiesFuture Med Chem20157121511151926306654
- XuHBLiuYJLiLAromatase inhibitor versus tamoxifen in postmenopausal woman with advanced breast cancer: a literature-based meta-analysisClin Breast Cancer201111424625121737354
- HowellARobertsonJFQuaresma AlbanoJFulvestrant, formerly ICI 182,780, is as effective as anastrozole in postmenopausal women with advanced breast cancer progressing after prior endocrine treatmentJ Clin Oncol200220163396340312177099
- OsborneCKPippenJJonesSEDouble-blind, randomized trial comparing the efficacy and tolerability of fulvestrant versus anastrozole in postmenopausal women with advanced breast cancer progressing on prior endocrine therapy: results of a North American trialJ Clin Oncol200220163386339512177098
- HowellARobertsonJFAbramPComparison of fulvestrant versus tamoxifen for the treatment of advanced breast cancer in postmenopausal women previously untreated with endocrine therapy: a multinational, double-blind, randomized trialJ Clin Oncol20042291605161315117982
- ChiaSGradisharWMauriacLDouble-blind, randomized placebo controlled trial of fulvestrant compared with exemestane after prior nonsteroidal aromatase inhibitor therapy in postmenopausal women with hormone receptor-positive, advanced breast cancer: results from EFECTJ Clin Oncol200826101664167018316794
- di LeoAJerusalemGPetruzelkaLResults of the CONFIRM phase III trial comparing fulvestrant 250 mg with fulvestrant 500 mg in postmenopausal women with estrogen receptor-positive advanced breast cancerJ Clin Oncol201028304594460020855825
- Di LeoAJerusalemGPetruzelkaLFinal overall survival: fulvestrant 500 mg vs 250 mg in the randomized CONFIRM trialJ Natl Cancer Inst20141061djt33724317176
- PritchardKIRolskiJPapaiZResults of a phase II study comparing three dosing regimens of fulvestrant in postmenopausal women with advanced breast cancer (FINDER2)Breast Cancer Res Treat2010123245346120632084
- CopeSOuwensMJJansenJPSchmidPProgression-free survival with fulvestrant 500 mg and alternative endocrine therapies as second-line treatment for advanced breast cancer: a network meta-analysis with parametric survival modelsValue Health201316240341723538193
- CristofanilliMTurnerNCBondarenkoIFulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trialLancet Oncol201617442543926947331
- WalkerAJWedamSAmiri-KordestaniLFDA approval of pal-bociclib in combination with fulvestrant for the treatment of hormone receptor-positive, HER2-negative metastatic breast cancerClin Cancer Res201622204968497227407089
- AyyagariRTangDPatterson-LombaOProgression-free survival with endocrine-based therapies following progression on non-steroidal aromatase inhibitor among postmenopausal women with hormone receptor positive, human epidermal growth factor receptor-2 negative metastatic breast cancer: a network meta-analysisCurr Med Res Opin20183491645165229781326
- HuttonBSalantiGCaldwellDMThe PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanationsAnn Intern Med20151621177778426030634
- HigginsJPAltmanDGGotzschePCCochrane Bias Methods Group; Cochrane Statistical Methods GroupThe Cochrane Collaboration’s tool for assessing risk of bias in randomised trialsBMJ2011343d592822008217
- ZhouZRZhangTSLiBExtracting and transforming of appropriate data of meta-analysis in survival curveChin J Evid Based Cardiovasc Med20146243247
- WeltonNJSuttonAJCooperNJAbramsKRAdesAEEvidence synthesis for decision making in healthcareChichester (UK)John Wiley & Sons, Inc2012
- SlamonDJNevenPChiaSPhase III randomized study of ribociclib and fulvestrant in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: MONA-LEESA-3J Clin Oncol201836242465247229860922
- SledgeGWJrToiMNevenPMONARCH 2: abemaciclib in combination with fulvestrant in women with HR+/HER2–advanced breast cancer who had progressed while receiving endocrine therapyJ Clin Oncol201735252875288428580882
- Di LeoAJohnstonSLeeKSBuparlisib plus fulvestrant in postmenopausal women with hormone-receptor-positive, HER2-negative, advanced breast cancer progressing on or after mTOR inhibition (BELLE-3): a randomised, double-blind, placebo-controlled, phase 3 trialLancet Oncol20181918710029223745
- BaselgaJImSAIwataHBuparlisib plus fulvestrant versus placebo plus fulvestrant in postmenopausal, hormone receptor-positive, HER2-negative, advanced breast cancer (BELLE-2): a randomised, double-blind, placebo-controlled, phase 3 trialLancet Oncol201718790491628576675
- ZamanKWinterhalderRMamotCFulvestrant with or without selumetinib, a MEK 1/2 inhibitor, in breast cancer progressing after aromatase inhibitor therapy: a multicentre randomised placebo-controlled double-blind phase II trial, SAKK 21/08Eur J Cancer201551101212122025892646
- MusolinoACamponeMNevenPPhase II, randomized, placebo-controlled study of dovitinib in combination with fulvestrant in postmenopausal patients with HR+, HER2– breast cancer that had progressed during or after prior endocrine therapyBreast Cancer Res20171911828183331
- KropIEMayerIAGanjuVPictilisib for oestrogen receptor-positive, aromatase inhibitor-resistant, advanced or metastatic breast cancer (FERGI): a randomised, double-blind, placebo-controlled, phase 2 trialLancet Oncol201617681182127155741
- ClemonsMJCochraneBPondGRRandomised, phase II, placebo-controlled, trial of fulvestrant plus vandetanib in postmenopausal women with bone only or bone predominant, hormone-receptor-positive metastatic breast cancer (MBC): the OCOG ZAMBONEY studyBreast Cancer Res Treat2014146115316224924416
- AdelsonKRamaswamyBSparanoJARandomized phase II trial of fulvestrant alone or in combination with bortezomib in hormone receptor-positive metastatic breast cancer resistant to aromatase inhibitors: a New York Cancer Consortium trialNPJ Breast Cancer201621603728721390
- KornblumNZhaoFManolaJRandomized Phase II trial of fulvestrant plus everolimus or placebo in postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative metastatic breast cancer resistant to aromatase inhibitor therapy: results of PrE0102J Clin Oncol201836161556156329664714
- WilsonSChiaSKTreatment algorithms for hormone receptor-positive advanced breast cancer: applying the results from recent clinical trials into daily practice-insights, limitations, and moving forwardAm Soc Clin Oncol Educ Book201333e20e27
- KwapiszDCyclin-dependent kinase 4/6 inhibitors in breast cancer: palbociclib, ribociclib, and abemaciclibBreast Cancer Res Treat20171661415428741274
- ButtAJMcNeilCMMusgroveEASutherlandRLDownstream targets of growth factor and oestrogen signalling and endocrine resistance: the potential roles of c-Myc, cyclin D1 and cyclin EEndocr Relat Cancer200512Suppl 1S47S5916113099
- FinnRSDeringJConklinDPD 0332991, a selective cyclin D kinase 4/6 inhibitor, preferentially inhibits proliferation of luminal estrogen receptor-positive human breast cancer cell lines in vitroBreast Cancer Res2009115R7719874578
- ChirilaCMitraDColosiaAComparison of palbociclib in combination with letrozole or fulvestrant with endocrine therapies for advanced/metastatic breast cancer: network meta-analysisJ Cell Biochem201733814571466
- WilsonFRVaruAMitraDCameronCIyerSSystematic review and network meta-analysis comparing palbociclib with chemotherapy agents for the treatment of postmenopausal women with HR-positive and HER2-negative advanced/metastatic breast cancerBreast Cancer Res Treat2017166116717728752187
- Lopes de MenezesDEPengJGarrettENCHIR-258: a potent inhibitor of FLT3 kinase in experimental tumor xenograft models of human acute myelogenous leukemiaClin Cancer Res200511145281529116033847
- HeinzleCSutterlütyHGruschMGrasl-KrauppBBergerWMarianBTargeting fibroblast-growth-factor-receptor-dependent signaling for cancer therapyExpert Opin Ther Targets201115782984621375471
- EastonDFPooleyKADunningAMGenome-wide association study identifies novel breast cancer susceptibility lociNature200744771481087109317529967
- Ruiz-NarváezEAHaddadSALunettaKLGene-based analysis of the fibroblast growth factor receptor signaling pathway in relation to breast cancer in African American women: the AMBER consortiumBreast Cancer Res Treat2016155235536326743380
- AndréFCortésJRationale for targeting fibroblast growth factor receptor signaling in breast cancerBreast Cancer Res Treat201515011825677745
- RugoHVidulaNMaCImproving response to hormone therapy in breast cancer: new targets, new therapeutic optionsAm Soc Clin Oncol Educ Book201635e40e5427249746
- AndréFBachelotTCamponeMTargeting FGFR with dovitinib (TKI258): preclinical and clinical data in breast cancerClin Cancer Res201319133693370223658459
- LinWZXuQNWangHBLiXYFulvestrant plus targeted agents versus fulvestrant alone for treatment of hormone-receptor positive advanced breast cancer progressed on previous endocrine therapy: a meta-analysis of randomized controlled trialsBreast Cancer201724334535228324247