
Abstract
Purpose
The purpose of this study was to evaluate the combined measurement of serum CEA, TPA, and CA 15-3, using an individual reference limit (IRL), for predicting distant metastases in asymptomatic women following a diagnosis of primary breast cancer.
Methods
A total of 231 patients were followed up for a mean of 5.5±1.6 years. An IRL for defining critical changes (CCs) in marker levels was used as a warning signal of pending distant metastases.
Results
Sensitivity, specificity, and accuracy of the combined CEA–TPA–CA 15-3 marker panel for predicting patient outcome were 95.2%, 97.8%, and 97.9%, respectively. In all, 19 (8.3%) patients relapsed with a mean lead time to radiological evidence of metastases of 11.7±13.8 months.
Conclusion
We concluded that the combined measurement of CA 15-3, CEA, and TPA using an IRL for determining the CC in markers levels is an accurate strategy for predicting outcome during postoperative monitoring of asymptomatic breast cancer patients. Whether the early prediction of metastasis and subsequent administration of therapy impacts on patient outcome should now be the objective of a prospective clinical trial. The marker panel described here could serve as the basis for such a trial.
Introduction
Although the serial measurement of circulating markers during postoperative monitoring of asymptomatic breast cancer patients can result in the early detection of metastatic disease,Citation1 the practice is opposed by most American and European expert panels.Citation2–Citation5 The main reason for this opposition is the absence of high-level evidence demonstrating that measurement of serum markers in this setting has clinical utility, ie, enhances patient outcome or leads to a better quality of life. Despite most published guidelines recommending against the use of markers in the postoperative surveillance of asymptomatic women, many centers continue to perform these tests, especially CA 15-3 and CEA.Citation6–Citation8 Less frequently measured markers during surveillance include TPA, TPS, and the soluble form of HER2.Citation1
Early work showed that measurement of single markers had limited sensitivity and specificity in detecting early metastatic disease following curative surgery for breast cancer.Citation9–Citation11 More recent data, however, using multiple markers have shown increased accuracy for detecting early metastases.Citation12–Citation14 To further enhance the accuracy for detection of metastases, we investigated an individual reference limit (IRL) as a cutoff point for a panel of three markers, ie, CEA, TPA, and CA 15-3.Citation15 In this preliminary study, after a mean follow-up of 3.7 years, the sensitivity of the marker panel for detecting metastases was 93% and the specificity was 97.6%.Citation15 The aim of the present study was to confirm these preliminary findings using a greater number of patients and longer follow-up.
Materials and methods
Marker measurement and patient follow-up
From September 2009 to January 2017, 231 consecutively women who had undergone mastectomy for breast cancer and who were disease free were intensively monitored for 5.5±1.6 years (mean ± sd; range, 1–7.4 years) with serial serum determination of the marker panel, CA 15-3, CEA, and TPA. Mean age of the patients was 62 years (mean ± sd, 9 years; range, 36–84 years). No patient received neo-adjuvant treatment. To date, 19 patients have relapsed. Clinical data relating to 11 survivors from these 19 relapsed patients were updated in December 30, 2017. During follow-up, the marker panel was measured every 3 months. All marker determinations were performed as previously reported.Citation15 In addition to the serial marker determinations, physical and radiological examinations were performed every 6 months. Laboratory data and instrumental examinations were carried out by personnel blinded to the clinical status of the patients.
Determination of the IRL for assessing critical change (CC) in marker levels
Since factors such as the presence of concurrent benign disease and woman’s age may affect marker levels, we used an IRL for determining the CC signaling the emergence of early metastases. For each disease-free patient, the IRL was calculated using the mean marker concentration ± sd of the 5 five consecutive monthly determinations. The IRL was computed as mean ± 2 sd for CEA and CA 15-3 and mean ±3 sd for TPA. The use of 3 rather than 2 sd for TPA was due to the higher analytical and biological variability of TPA compared to CEA and CA 15-3.Citation16 When the sd of the 5 consecutive monthly determinations was less than 20% of the mean value, the 20% of the mean value was used as sd. To minimize the impact of possible new benign disease or progression of existing disease altering markers levels, the IRL was recalculated every 3 years. Two consecutive values of any of the three markers giving levels higher than the IRL were considered a CC and thus regarded as suspicious of relapse (). In this situation, a complete instrumental workup was immediately carried out to establish if recurrence(s) was present.
Table 1 Formula for calculation of the IRL and definition of CC of a serum tumor marker panel
Radiological examinations
Both at the start and end of the study, all patients underwent skeletal X-ray, bone scintigraphy (BS), liver echography (LE), and abdomen and thoracic computed tomography (AT-CT).Citation17–Citation19 During follow-up, BS, LE, and AT-CT examinations were carried out in patients suspected of a pending relapse as indicated by clinical symptoms and/or increasing marker level. Patients with positive radiological examinations were investigated as follows: hotspots on the BS with an equivocal interpretation were confirmed by computed tomography (CT) and/or magnetic resonance imaging (MRI); thoracic lesions equivocal by CT were clarified by bronchoscopy and/or cyto/histologic examination; equivocal LE lesions were further investigated by CT or fine needle aspiration cytology; soft tissue involvement was confirmed by cytology and/or histology; and pleural or peritoneal involvement was confirmed by cytology or imaging. In cases where the diagnostic workup was negative or unclear, a full diagnostic clinical and radiological assessment was carried out every 6 months up to 18 months until the uncertainty was resolved. If the diagnostic assessment was found to be negative, the marker warning signal was considered false and such patients returned to standard follow-up with the marker panel. Consistent with current guidelines, yearly mammographic screening was carried out in all patients. All patients provided consent to be postoperatively monitored with the instrumental and laboratory examinations described.
Determination of lead time (LT)
In relapsed patients, the marker LT was defined as the time from the second of the two consecutive increments of the first CC to definitive radiological and/or cytohistological diagnosis of metastatic disease. Relapses were categorized as follows: 1) relapses in patients without any ongoing adjuvant (AV) treatment (n=10); 2) relapses in patients who were under prolonged AV hormone therapy (n=2); and 3) relapses in patients who were under prolonged AV treatment that was changed at the time of the CC (n=8). The AV treatment for patients in the last subgroup before and after CC was hormone therapy followed by chemotherapy (CH) in three patients, CH followed by hormone therapy in one patient, a different regimen of CH administered to one patient, and first-line hormone therapy followed by second-line hormone therapy in three patients.
Statistical analyses
Categorical data were described by frequency (absolute and relative), whereas continuous data were expressed by mean and sd. To evaluate the normality of the LT distribution, the Kolmogorov–Smirnov test was carried out and the comparison between groups (with and without AV treatment, current and previous methodology) was performed by Student’s t-test (two tailed). Data relating to the marker tests were expressed as percentage of sensitivity and specificity. Sensitivity was computed in relapsed patients as positive results at the test CC (true positives)/the total number of true relapses (true positives plus false negatives). Specificity was computed as the number of negative results in the absence of a CC in marker levels (true negatives) divided by the number of true negatives plus false positives. Accuracy was computed as the number of true-negative results plus true-positive results divided by the total number of results. A positive test (CC) was defined as true- or false-positive test, and a negative test (CC) was defined as true- or false-negative test according to whether it was or was not confirmed by a prolonged clinical-imaging course, respectively. The rate of false “warning signals” per year of follow-up per 100 patients was defined as the ratio between the total number of false warning signals and the number of years a patient was at risk. Finally, a comparison between specificity (first 3 years against the successive 3 years IRL determination) was carried out by the two-proportion z-test. Significance was fixed at 0.05. All analyzes, descriptive and inferential, were performed by SPSS v.24 technology.
Results
Non-relapsed patients
After a mean follow-up of 64.9 months (±19.6 months, sd), 212 (91.7%) of the 231 patients were apparently free of distant metastases. In total, 4,763 measurements of CEA–TPA–CA 15-3 were carried out in 212 patients. The AV treatments received by these women and the characteristics of their tumors are summarized in . The specificity of CEA, TPA, CA 15-3, CEA–CA 15-3, and CEA–TPA–CA 15-3 combination for predicting absence of metastasis was 99.5%, 98.6%, 99.7%, 99.2%, and 97.8%, respectively (). The rates of false warning signals per year of follow-up per 100 patients were 1.8, 5.1, 1.1, 2.9, and 8 for CEA, TPA, CA 15-3, CEA–CA 15-3, and CEA–TPA–CA 15-3 combinations, respectively ().
Table 2 Principal characteristics of the 212 studied patients
Table 3 Serum determinations higher than IRL and false warning signals for CEA, TPA, CA 15-3, and CEA–TPA–CA 15-3 combination in the 231 studied patients with a mean follow-up of 64.9 months (range: 12–89 months)
Relapsed patients
Of the 231 patients studied, 21 relapses occurred in 19 (8.3%) patients. The AV treatments received by these women and the characteristics of their tumors are summarized in . In the eight relapsed patients with stage IA, the molecular biological subtype was luminal A (one), non-luminal (one), luminal B (two), ER+ with not determined HER2 (three), and no biological parameters determined (one). Furthermore, the disease-free interval (DFI) was relatively long (167±96 months, mean ± sd). lists the DFI, sensitivity, and LT of the marker panel. One of the 19 relapsed patients with skeletal involvement was falsely negative, while for all the remaining 20 relapses, the IRL-CC was the warning signal. No patient had clinical symptoms at the radiological diagnosis of metastases. Two patients relapsed twice. In both of these cases, the first relapse involved liver lesions that were surgically removed. After being apparently disease free for 3 years, one of these patients developed bone involvement, while the other recurred with cerebellum metastasis after 2 years being apparently disease free.
Table 4 Principal characteristics of the 19 relapsed patients
Table 5 IRL: DFI, sensitivity (S), and LT of CEA, TPA, and CA 15-3 in the early detection of breast cancer distant metastases
The metastases sites in the other 16 patients were: bone in 5, lung in 2, liver in 2, soft tissues in 5, bone and soft tissues in 1, and bone, lung, and soft tissues in 1 patient. In patients relapsing during AV therapy, sensitivity ranged from 27.3% for CEA or TPA to 90.9% for the CEA–TPA–CA 15-3 combination. The addition of TPA to the CEA–CA 15-3 panel increased the sensitivity from 63.6% to 90.9%. In patients relapsing without AV therapy, sensitivity ranged from 40% for CA 15-3 to 100% for CEA–TPA–CA 15-3. The addition of TPA to the CEA–CA 15-3 panel increased the sensitivity from 80% to 100%. A CC for CEA, TPA, CA 15-3, the CEA–CA 15-3 combination, and the CEA–TPA–CA 15-3 combination occurred in 8, 8, 8, 15, and 20 of the 21 relapses. Therefore, in 20 (95.2%) of the 21 relapses, the warning signal from the three markers was the alarm sign for a radiological assessment for possible metastatic disease. Sensitivity ranged from 27.3% for CEA or TPA to 95.2% for CEA–TPA–CA 15-3. The addition of TPA to the CEA–CA 15-3 panel increased the sensitivity from 71.4% to 95.2% ( and ). For all 21 relapses, the mean ± sd LT was 13.7±15.1 months for the CEA–CA 15-3 combination and 11.7±13.8 months for the CEA–TPA–CA 15-3 combination. In patients relapsing in the absence of AV therapy, the mean ± sd LT was 7±6.4 months, 8.8±8.5 months, and 8.5±8.2 months for CEA, TPA, and CA 15-3, and it was 7.2±7.1 months and 7.9±7.1 months for CEA–CA 15-3 and CEA–TPA–CA 15-3, respectively. The difference was significant for CEA and CEA–CA 15-3 association (P=0.027 and P=0.041, respectively).
In patients who relapsed while receiving AV therapy, the mean ± sd LT was 28.7±27 months, 2.7±2.1 months, and 15.5±11.1 months for CEA, TPA, and CA 15-3, whereas it was 21.1±18.8 months and 15.6±17.8 months for CEA–CA 15-3 and CEA–TPA–CA 15-3, respectively. In two patients, after having obtained their informed consent, hormone therapy was started at the time of the warning signal from the CEA–TPA–CA 15-3 combination, with negative radiological examinations. When both these relapses were added to the group of eleven relapses in patients receiving postoperative AV treatment (), the mean ± sd LT became 15.9±16.1 months (vs 5.2±5.4 months, P=0.052 for relapses without postoperative AV therapy).
Table 6 IRL: sensitivity (S) and LT of CEA–CA 15-3 and CEA–TPA–CA 15-3 associations in the early detection of breast cancer distant metastases
Survival of patients with metastasis
As of December 2017, 11 (58%) of the 19 relapsed patients were alive. In seven of the eight patients who died, metastatic disease was the cause of death. In all 19 patients, the mean survival time from treatment of metastatic disease to death was 52.1±37 months (range, 7–131 months; median, 38 months) and the 5-year survival rate was 54.5% (6 of 11 evaluable patients). Two of these 19 patients who underwent prolonged AV treatment before radiological signs of metastases exhibited high IRLs for the marker panel. In three patients, AV therapy was started soon after surgical removal of metastases (contra-lateral axillary lymph nodes [one] or liver [two]). In five patients, the survival time was 45, 60, 60, 90, and 115 months while the mean survival was 74±28 months (range, 45–115 months; median, 60 months).
Description of two cases of early treatment with long-term survival and without clinical symptoms related to the relapse
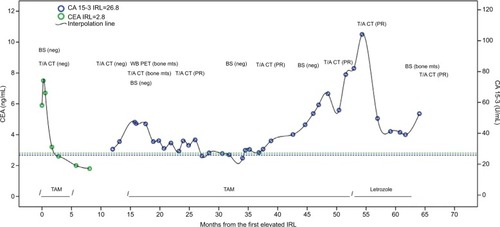
Patient 1 was diagnosed with T1N1M0 in March 2012. Following primary surgery (quadrantectomy), she received six cycles of cyclophosphamide, methotrexate, 5-fluorouracil CH, followed by 7 years of hormone therapy (tamoxifen for 5 years plus vorozole for 2 years). At the time of the CEA CC, she had stopped AV treatment for about 3 years and was asymptomatic. The complete workup failed to detect metastasis. With her consent, she again began to take tamoxifen while a concomitant intense radiological monitoring was performed. During the 7 months of adjuvant tamoxifen, a progressive decrease in CEA values to normal range occurred. No radiological evidence of relapse occurred during this time. Subsequently, the patients stopped taking tamoxifen but continued with regular measurement of the marker panel and instrumental examinations. At the end of March 2013, although asymptomatic, an increase in CA 15-3 suggested a pending relapse. About 4 months after the CA 15-3 warning signal, whole-body positron-emission tomography (8-5-13) and whole-body CT (9-4-13) confirmed a secondary bone involvement at L4 and the patient was given tamoxifen.
Following tamoxifen administration, CA 15-3 levels initially decreased to lower than the CA 15-3 IRL with a partial response at thoracic/abdominal CT. Thereafter, levels fluctuated for about 1 year and then increased up to October 2016 when tamoxifen was replaced with letrozole. Following letrozole administration, CA 15-3 values again decreased although they stayed higher than the CA 15-3 IRL. During the interval from August 2013 to October 2017, the patient was asymptomatic and radiological monitoring was consistent with the partial response ().
Figure 1 Serum CEA and CA 15-3 behavior during postoperative follow-up of patient 1.
Abbreviations: BS, bone scintigraphy; CT, computed tomography; IRL, individual reference limit; mts, metastases; neg, negative; PET: positron emission tomography; PR, partial response; SD, stable disease; T/A, thoracic/abdominal; TAM, tamoxifen; WB, whole body.
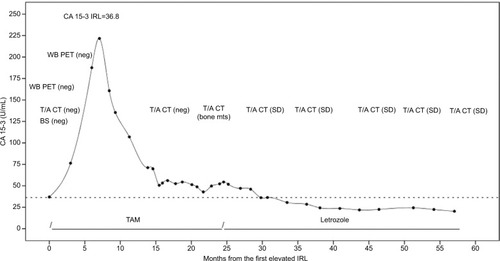
The second patient, who had T1N0M0 postoperative staging, underwent primary surgery (radical mastectomy modified according to Scanlon’s technique) on February 1991 when she was 48 years. She received AV tamoxifen for 4 years. In January 2013, concomitant TPA and CA 15-3 CC were the warning signal of a pending relapse. At this time, she was asymptomatic and not receiving any systemic treatment. A complete workup however, failed to identify metastatic disease. As with the previous patient, these patients following consent began taking tamoxifen, ie, from April 2013 until November 2014. After commencing tamoxifen, TPA and CA 15-3 levels first progressively decreased and then fluctuated with levels marginally higher than the IRL. In November 2014, a further workup with whole-body CT showed diffuse bone metastasis. At that time, tamoxifen was replaced with letrozole, which led to levels of TPA and CA 15-3 lower than the IRL for these markers. During April 2013 to October 2017, the patient was asymptomatic. In addition, radiological monitoring from November 2014 to October 2017 documented stable disease ().
Figure 2 Serum CA 15-3 behavior during postoperative follow-up of patient 2.
Abbreviations: BS, bone scintigraphy; CT, computed tomography; IRL, individual reference limit; mts, metastases; neg, negative; PET: positron emission tomography; SD, stable disease; T/A, thoracic/abdominal; TAM, tamoxifen; WB, whole body.
Discussion
One of the main arguments against the routine use of markers in the postoperative management of asymptomatic women following a diagnosis of breast cancer is the limited efficiency of single markers for detecting early recurrences.Citation2 Although single markers have limited accuracy in detecting recurrences,Citation2 we show here that the combined measurement of CA 15-3, CEA, and TPA and the use of an IRL for defining a CC in marker levels predicted patient outcome with a sensitivity of 95.2%, specificity of 97.8%, and overall accuracy of 97.9%. Furthermore, combined measurement of the three markers provided an LT of ~1 year. A limitation of our study, however, is that only 19 (8.3%) of the 231 studied patients had evidence of distant metastases.
The key question however, is whether the early detection of recurrences followed by the early administration of systemic therapy has clinical utility. Despite the availability of the markers used in the investigation for over 20 years, it is unsatisfactory that we still lack evidence as to whether their measurement in asymptomatic women following a diagnosis of breast cancer is clinically useful. Clearly, this question needs to be urgently addressed in a prospective randomized trial. Should such a trial be carried out, the three markers with their IRLs described in this investigation might be considered for use in the test arm of the study.
Before concluding, we should state that two randomized prospective trials carried out the in 1980s and early 1990sCitation20,Citation21 compared an intensive follow-up regime with a minimalist strategy for the postoperative surveillance of breast cancer patients. Both these trials indicated that physical examinations and mammography carried out timely did not significantly affect overall survival (OS) obtained using imaging and routine laboratory examinations. However, the relevance of these old studies to the modern management of breast cancer patients is questionable because the determination of any of the abovementioned markers was not included.Citation1 Furthermore, as to early recurrence detection, the older instruments were less accurate than the modern ones. Perhaps, the most significant clinical change since these studies were performed is the increased number of new drugs tailored for subgroups of patients with recurrent breast cancers, particularly ER-+ and HER2-+ cancers.Citation22–Citation26 Clearly, these deficiencies need to be addressed with a trial incorporating the measurement of serum markers and administration of modern treatments.
Conclusion
We have shown that the combined measurement of serial levels of CA 15-3, CEA, and TPA predicts patient outcome following curative surgery for breast cancer with high accuracy and provides an LT of ~1 year for the detection emerging metastasis. Therefore, a prospective randomized multicenter clinical trial comparing patients recruited to an intensive postoperative follow-up with CEA–TPA–CA 15-3 tumor marker panel as described here vs no follow-up should be carried out. This is to evaluate 1) whether a significant favorable impact on median survival from diagnosis of metastases and OS occurs in the intensive CEA–TPA–CA 15-3 follow-up arm vs no follow-up and 2) whether within the intensive CEA-TPA-CA 15-3 follow-up arm in ER+ patients, a hormone salvage treatment started following the CC before radiological documentation significantly prolonged the just mentioned end points compared to patients starting hormone salvage therapy after metastases have been radiologically documented.
Ethics and consent statement
The research and consent process were approved by the Council of the Department of Internal Medicine at Pisa University. All the studied patients gave verbal informed consent, witnessed in the presence of a family member, and were free to remove themselves from the trial at any time.
Disclosure
The authors report no conflicts of interest in this work.
References
- DuffyMJMcDermottEWCrownJBlood-based biomarkers in breast cancer: from proteins to circulating tumor cells to circulating tumor DNATumour Biol2018405101042831877616
- No authors listedClinical practice guidelines for the use of tumor markers in breast and colorectal cancerJ Clin Oncol199614284328778874347
- BastRCRavdinPHayesDFAmerican Society of Clinical Oncology Tumor Markers Expert Panel2000 Update of recommendations for the use of tumor markers in breast and colorectal cancer: clinical practice guidelines of the American Society of Clinical OncologyJ Clin Oncol20011961865187811251019
- HarrisLFritscheHMennelRAmerican Society of Clinical OncologyAmerican Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancerJ Clin Oncol200725335287531217954709
- SenkusEKyriakidesSOhnoSESMO Guidelines CommitteePrimary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-upAnn Oncol201526Suppl 5v8v3026314782
- RamseySDHenryNLGralowJRTumor marker usage and medical care costs among older early-stage breast cancer survivorsJ Clin Oncol201533214915525332254
- KeatingNLLandrumMBGuadagnoliEWinerEPAyanianJZSurveillance testing among survivors of early-stage breast cancerJ Clin Oncol20072591074108117369571
- HahnEEHaysRDKahnKLLitwinMSGanzPAUse of imaging and biomarker tests for posttreatment care of early-stage breast cancer survivorsCancer2013119244316432424105101
- DnistrianAMSchwartzMKGreenbergEJSmithCASchwartzDCCA 15-3 and carcinoembryonic antigen in the clinical evaluation of breast cancerClin Chim Acta19912002–381931777973
- GuadagniFFerroniPCarliniSA re-evaluation of carcinoembryonic antigen (CEA) as a serum marker for breast cancer: a prospective longitudinal studyClin Cancer Res2001782357236211489813
- MarianiLMiceliRMichilinSGionMSerial determination of CEA and CA 15.3 in breast cancer follow-up: an assessment of their diagnostic accuracy for the detection of tumour recurrencesBiomarkers200914213013619330591
- MolinaRZanónGFilellaXUse of serial carcinoembryonic antigen and CA 15.3 assays in detecting relapses in breast cancer patientsBreast Cancer Res Treat199536141487579505
- StieberPNagelDBlankenburgIDiagnostic efficacy of CA 15-3 and CEA in the early detection of metastatic breast cancer – a retrospective analysis of kinetics on 743 breast cancer patientsClin Chim Acta201544822823126160053
- di GioiaDBlankenburgINagelDHeinemannVStieberPTumor markers in the early detection of tumor recurrence in breast cancer patients: CA 125, CYFRA 21-1, HER2 shed antigen, LDH and CRP in combination with CEA and CA 15-3Clin Chim Acta20164611727451906
- NicoliniAFerrariPFulceriFCarpiARossiGAn individual reference limit for ‘early’ diagnosis of metastatic breast cancer during postoperative follow-upBiomark Med20159430731725808435
- NicoliniATartarelliGCarpiAIntensive post-operative follow-up of breast cancer patients with tumour markers: CEA, TPA or CA15.3 vs MCA and MCA-CA15.3 vs CEA-TPA-CA15.3 panel in the early detection of distant metastasesBMC Cancer2006626917116247
- NicoliniAFerrariPSagripantiACarpiAThe role of tumour markers in predicting skeletal metastases in breast cancer patients with equivocal bone scintigraphyBr J Cancer1999799–101443144710188888
- NicoliniACarpiAFerrariPThe role of tumour markers in improving the accuracy of conventional chest X-ray and liver echography in the post-operative detection of thoracic and liver metastases from breast cancerBr J Cancer200083111412141711076646
- HojoTMasudaNMizutaniTIntensive vs. standard postoperative surveillance in high-risk breast cancer patients (INSPIRE): Japan Clinical Oncology Group Study JCOG1204Jpn J Clin Oncol2015451098398626246481
- No authors listedImpact of follow-up testing on survival and health-related quality of life in breast cancer patients. A multicenter randomised controlled trial. The Givio InvestigatorsJAMA1994271158715928182811
- Rosselli del TurcoMPalliDCariddiACiattoSPaciniPDistanteVIntensive diagnostic follow-up after treatment of primary breast cancer. A randomized trial. National Research Council Project on Breast Cancer follow-upJAMA199427120159315977848404
- HarbeckNGnantMBreast cancerLancet2017389100741134115027865536
- KaklamaniVGGradisharWJEndocrine therapy in the current management of postmenopausal estrogen receptor-positive metastatic breast cancerOncologist201722550751728314835
- GingrasIGebhartGde AzambujaEPiccart-GebhartMHER2-positive breast cancer is lost in translation: time for patient-centered researchNat Rev Clin Oncol2017141166968128762384
- NixonNAHannoufMBVermaSA review of the value of human epidermal growth factor receptor 2 (HER2)-targeted therapies in breast cancerEur J Cancer201889728129241083
- de GrootAFKuijpersCJKroepJRCDK4/6 inhibition in early and metastatic breast cancer: a reviewCancer Treat Rev20176013013828961554