
Abstract
Objective
Our study assessed the clinical utility and prognostic value of pretreatment hematological parameters and calculated coefficients including the platelet to lymphocyte ratio (PLR), neutrophil to lymphocyte ratio (NLR), and monocyte to lymphocyte ratio (MLR) in patients with cervical adenocarcinoma (CA).
Materials and methods
Among 738 cervical cancer patients with International Federation of Gynecology and Obstetrics (FIGO) stages IA–IV treated at our institution, 96 (13%) presented with CA histology. The blood samples, collected within 10 days before treatment, were analyzed using a Sysmex XN-2000 system. The statistical tests included Mann–Whitney U-tests, log-rank tests, and Cox regression models. The cutoff points for the calculated hematological coefficients (NLR, PLR, and MLR) were determined using the MedCalc statistical program.
Results
The prognostic factor for overall survival (OS) and recurrence-free survival (RFS) in CA was clinical stage according to FIGO classification (FIGO IIB–IV vs I–IIA) (P=0.0001; P=0.002). Among patients with FIGO stage IIB–IV treated with radiotherapy/chemoradiotherapy, an elevated PLR was a negative prognostic factor for OS (P=0.017; HR: 2.96; 95% CI: 2.069–3.853). Among all patients, an elevated pretreatment NLR was a poor prognostic factor for OS (P=0.014; HR: 2.85; 95% CI: 2.011–3.685) and RFS (P=0.049; HR: 4.0; 95% CI: 2.612–5.392). The white blood cell count (WBC) before treatment was significantly higher in patients who died during follow-up (P=0.009).
Conclusion
Elevated NLR values before treatment may be associated with a shorter time of RFS and OS, while PLR index may have prognostic significance for OS in patients with advanced disease (FIGO IIB–IV). Both indexes and WBC may be a cost-effective biomarker that can be used conveniently for stratification of recurrence risk and death.
Introduction
Due to the development of screening programs, the incidence of cervical cancer has decreased worldwide; however, the incidence of cervical adenocarcinoma (CA) has increased, especially in younger age groups. According to the literature, cervical cancer is the fourth most frequently occurring malignancy among women and the second most common malignancy of the female genital tract, with 200,000 deaths and 500,000 new cases worldwide annually.Citation1,Citation2 CA histopathology accounts for 5%–25% of all cervical cancer cases. Data on the influence of histopathology on survival in cancer patients are conflicting; however, most studies confirm adenocarcinoma histopathology as a poor prognostic factor in cervical cancer.Citation3–Citation5 Some authors have identified different molecular profiles between histopathological types and the need for clinical trials to determine the optimal treatment regimen to enhance the outcome of patients with CA.Citation4–Citation7 Cervical cancer is staged according to International Federation of Gynecology and Obstetrics (FIGO) classification. The clinical stage of the disease can be assessed clinically but other parameters are assessed surgically. Therefore, non-invasive pretreatment parameters, which can be used conveniently and cost-effectively, are needed to predict the clinical course of the disease and the likelihood of response to treatment. Serum C-reactive protein (CRP) is not routinely evaluated before treatment, and it has been shown to have a negative prognostic value in patients with other malignancies such as hepatocellular cancerCitation8 and ovarian carcinoma.Citation9 The inflammation process plays an important role in the carcinogenesis and cancer progression and may act as a measure of disease progression. Neutrophils have been shown to secrete vascular endothelial growth factor, IL-18, and matrix metalloproteinases that directly contribute to tumor-related angiogenesis, tumor growth, and metastatic processes.Citation10–Citation12 Systemic nonspecific markers of inflammation such as the platelet to lymphocyte ratio (PLR) and neutrophil to lymphocyte ratio (NLR) have been investigated in different types of malignancies such as non-small-cell lung cancer,Citation13 pancreatic cancer,Citation14 gastric cancer,Citation15,Citation16 renal cell,Citation17 and colorectal cancer.Citation18–Citation20 Several studies have also evaluated the role of systemic inflammation in malignancy in cervical cancer. However, little is known about the prognostic value of the pretreatment levels of inflammatory markers, including white blood cell count (WBC), NLR, and PLR, in patients with CA. To our knowledge, there are no studies on the role of these parameters in this histopathological type of cervical carcinoma. Taking into account that adenocarcinoma often presents with less favorable outcomes,Citation3–Citation5,Citation21 the assessment of easily applicable prognostic factors for possible additional therapies is of particular importance.
The aim of this study was to determine the clinical usefulness and prognostic value of pretreatment hematological parameters including WBC, hemoglobin (Hb), and platelets (PLT) as well as calculated coefficients such as NLR, PLR, and monocyte to lymphocyte ratio (MLR) in patients with CA.
Materials and methods
We retrospectively analyzed data from cervical cancer patients with FIGO stage IA–IV disease who were treated consecutively from November 2003 to January 2008 at the Maria Sklodowska-Curie Institute-Oncology Center in War-saw. The eligibility criteria included patients with cervical cancer with confirmed adenocarcinoma histopathology who were qualified to receive radical treatment. The histopathological features of all tumors were confirmed by our institutional pathologist. Data on all clinical factors and complete blood parameters were collected within 10 days before treatment. Blood samples were evaluated using a Sysmex XN-2000 system. The NLR was defined as the absolute number of neutrophils divided by the absolute number of lymphocytes (G/L), the PLR as the absolute number of PLT by the absolute number of lymphocytes (G/L), and the MLR as the absolute number of monocytes by the absolute number of lymphocytes (G/L) in patients with adenocarcinoma of the uterine cervix. Patients were staged according to FIGO classification and treated according to European Society for Medical Oncology and European Society of Radiotherapy and Oncology (ESTRO) recommendations. Before treatment, patients were staged with clinical examination, computed tomography (CT) or X-ray imaging of the chest, and CT or magnetic resonance (MR) of the abdomen and pelvis. In case of suspected infiltration of the bladder or rectum, histopathological confirmation of cystoscopy or rectoscopy specimens was performed. Patients with early cervical cancer (FIGO stages IA 1–2, IB1, and IIA) were treated with radical hysterectomy and bilateral oophorectomy, including the part of the cardinal and uterosacral ligament at the upper end of the vagina, as well as pelvic lymphadenectomy. In case of enlarged para-aortal lymph nodes, para-aortal lymphadenectomy or biopsy was performed. After surgical treatment, patients were qualified for adjuvant therapy based on risk factors. In case of the presence of at least two intermediate risk factors such as deep stromal invasion, large tumor, or lymphovascular space invasion, the patients were administered external beam irradiation (EBRT) with or without chemotherapy and brachytherapy (BT) as two 7.5-Gray (Gy) fractions prescribed to the vaginal vault. Patients with high-risk factors such as positive lymph nodes (N1), positive margins (R1), or parametrial infiltration were treated with chemoradiotherapy (CCRT). Patients with locally advanced cervical cancer, FIGO stages IB2, IIB–IVA, were also treated with CCRT. The first-line therapy in these patients included CCRT with weekly cisplatin at a dose of 40 mg/m2 of body surface area. Patients qualified to receive CCRT were treated with EBRT to the pelvis, and sometimes, to the para-aortic area, based on the three-dimensional (3D) planning system calculated using a HELAX system, according to the recommendations of Reports 50 and 62 of the International Commission on Radiation Units and Measurements (ICRU) with a 3D conformal technique. Clinical target volumes (CTVs) with a margin of 5 mm in all directions were delineated on the CT scans, and the planning target volumes (PTVs) were defined. Organs at risk (OAR) were also delineated during the planning procedure. Patients were treated with a total dose of 45–46 Gy to the pelvic and/or para-aortal region, and a 60–64 Gy boost in cases of enlarged lymph nodes measuring over 2 cm or resistant tumor in the parametrium. The patients started high-dose rate (HDR) BT in 1–3 weeks after EBRT. BT was performed with an iridium (Ir-192) source from microSelectron® (Nucletron Devices) once a week with 4 fractions of 7.5 Gy for a total dose of 30 Gy prescribed to the high-risk CTV. BT was planned according to the Groupe Européen de Curiethérapie-ESTRO recommendations with wider margins in the uterus and vaginal directions due to the lack of MR-based planning possibilities, according to the ICRU 38 Report. The planning system was based on CT images or radiographs. During the planning procedure, the PTV and OAR were delineated on CT scans. Fletcher, ring applicator, or 2–6 interstitial metal needles and intrauterine catheters were used to perform the HDR-BT.
The patients were followed-up every 3 months for the first 2 years, at 6-month intervals for the next 3, and annually after 5 years. In case of suspected relapse, we obtained histologically evaluated biopsy specimens. Patient follow-up was maintained until death or last observation, with a cutoff date of December 31, 2017.
Nonparametric Mann–Whitney U-tests were used for statistical comparisons of two independent groups. The probabilities of recurrence-free survival (RFS) and overall survival (OS) were assessed using univariate analysis with log-rank tests and multivariate analysis using Cox proportional hazards models. The OS was defined as the time interval between the start of treatment and the last follow-up or death. The RFS was the period between the first day of the treatment and disease recurrence, local or distant. The level of significance was P<0.05. The cutoff points for the calculated hematological coefficients (NLR, PLR, and MLR) were determined using the MedCalc statistical program.
Results
Among 738 patients with cervical cancer treated at our center, we excluded those with squamous cell histopathology (642) and two CA patients treated with palliative intent and included all patients with CA who were qualified to receive radical treatment; thus, a total of 94 patients with CA were included in the final analysis. Their median age was 53 years (range: 20–81 years). Forty-two patients had early-stage disease (FIGO I–IIA) and 52 had advanced disease (FIGO IIB–IVA). Early-stage disease was confirmed in 37 (61%) premenopausal and 57 (35%) postmenopausal patients. During the long-term follow-up (median: 66 months; range: 4.6–171.4 months), disease recurrence was observed in 44 (49%) patients (median age: 54 years), including 15 premenopausal and 29 postmenopausal women. The median time to relapse was 25 months. Forty-eight (51%) patients died. The clinical and pathological features of the patients with CA, the treatment characteristics, and the outcomes are presented in .
Table 1 Patients, treatment, and clinical outcome characteristics
NLR, PLR, and MLR and the ranges of the absolute numbers and median hematological parameters
The median pretreatment NLR was 2.32 (range: 0.7–20.3). The median PLR was 158 (range: 62.6–634). The calculated coefficients of NLR, PLR, and MLR, the ranges of the absolute numbers, and medians of the hematological parameters (Hb, WBC, and PLT) overall according to FIGO and clinical conditions are presented in .
Table 2 Median values and concentration ranges for NLR, PLR, MLR, WBC, Hb, and PLT according to the clinical condition
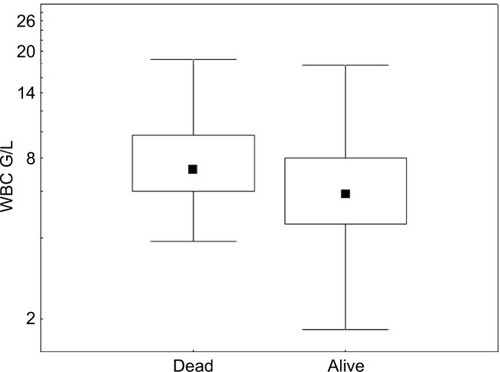
We next evaluated the correlation between the examined parameters and the age of patients, FIGO stage, and clinical status during the follow-up. No statistically significant correlations between age (<50 vs >50 years), FIGO stage, and the values of the studied parameters were observed. In patients with FIGO IIB–IV disease, only a trend of elevated NLR was observed (P=0.06). Of all hematological parameters, pretreatment WBC (P=0.009) was significantly higher in patients who died during follow-up than in patients who survived, as analyzed using the Mann–Whitney U-test (). Higher WBC values were also demonstrated in patients with metastases compared to the nonmetastatic group, however, this relationship was observed to be a trend (P=0.054).
Figure 1 Medians and WBC values according to clinical status (alive vs dead).
Abbreviation: WBC, white blood cell count.
Based on the analysis of receiver operating characteristic (ROC) curves for hematological factors cutoff points for NLR, PLR, and MLR were determined while maintaining the optimal sensitivity and specificity of tests for recurrence and no-recurrence groups. The results are presented in .
Table 3 ROC analysis: NLR, PLR, and MLR test characteristics for remission or recurrence in patients with adenocarcinoma of the cervix
Next, we analyzed the prognostic value of the examined parameters for RFS and OS. The first group comprised of patients treated with surgery and BT, EBRT, or CCRT (n=47); and the second group included patients treated with radiotherapy (RT) alone or CCRT (n=47).
The influence of the examined parameters on RFS in the whole group of patients
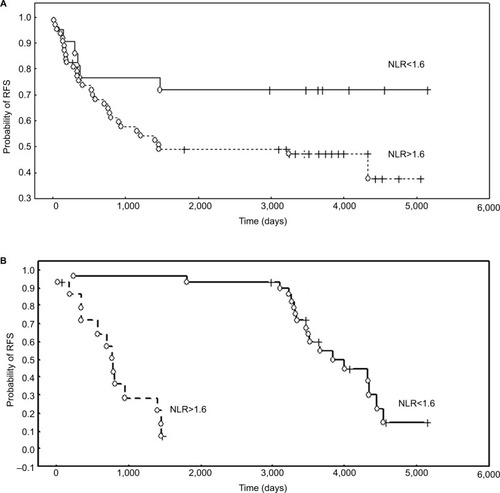
The results of the log-rank univariate analysis demonstrated that disease stage (FIGO IIB–IV) (P=0.002) and conservative treatment modality (patients treated only with RT or CCRT) (P=0.004) were associated with a shorter time to relapse. Among the hematological coefficients, NLR tended to be associated with RFS (P=0.059). However, multivariate Cox analysis demonstrated that the rate of NLR (P=0.021; HR 3.0; 95% CI: 2.063–3.936) was an independent prognostic factor and elevated values were associated with a worse RFS (). In the group of patients treated with surgery and further BT, RT, or CCRT (n=47), the correlation between NLR (P=0.001), PLR (P=0.006), and Hb (P=0.01) with RFS was demonstrated in log-rank tests, while Cox analysis revealed that only elevated NLR (P=0.049; HR: 4.0; 95% CI: 2.612–5.392) was an independent and poor prognostic factor for RFS ().
Figure 2 The probability of RFS according to NLR.
Notes: (A) RFS of CA patients treated with RT/CCRT stratified by NLR. (B) Probability of RFS according to NLR in patients treated with primary surgery and adjuvant RT/CCRT.
Abbreviations: CA, cervical adenocarcinoma; CCRT, chemoradiotherapy; NLR, neutrophil to lymphocyte ratio; RFS, recurrence-free survival; RT, radiotherapy.
The prognostic value of the examined parameters on OS in the whole group of patients
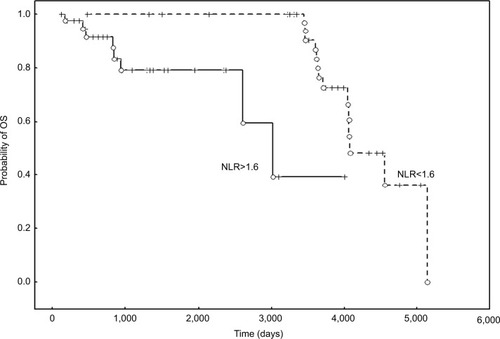
OS was associated with disease stage (FIGO IIB–IV) (P=0.0001) and conservative treatment modality, which is the treatment of choice for this clinical stage. Patients treated with RT or CCRT only (P=0.004) had a shorter OS, which may also be an effect of the disease advancement. Cox multivariate analysis revealed that, among hematological parameters, an elevated NLR was a poor prognostic factor for OS (P=0.014; HR: 2.85; 95% CI: 2.011–3.685) ().
Figure 3 OS of CA patients stratified by NLR.
Abbreviations: CA, cervical adenocarcinoma; NLR, neutrophil to lymphocyte ratio; OS, overall survival.
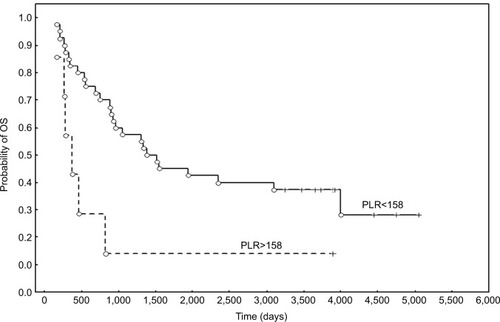
Survival analysis in patient groups divided according to FIGO stage and treatment modality confirmed that elevated values of PLR were correlated with poor prognosis for OS in patients with FIGO stage IIB-IV treated with RT/CCRT (P=0.017; HR: 2.96; 95% CI: 2.069–3.853) ().
Figure 4 The probability of OS according to the PLR in patients with FIGO stage IIB-IV treated with RT/CCRT.
Abbreviations: CCRT, chemoradiotherapy; FIGO, International Federation of Gynecology and Obstetrics; OS, overall survival; PLR, platelet to lymphocyte ratio; RT, radiotherapy.
Discussion
To our knowledge, this is the first study with mature data to investigate the prognostic value of pretreatment NLR, PLR, and other hematological parameters in patients with CA. As this histopathological type generally has a less favorable outcome,Citation21,Citation22 easy and inexpensive identification of high-risk groups is especially important. Therefore, selecting patients with a particularly unfavorable prognosis and encouraging them to consider the use of new forms of treatment is a priority task. This study is a continuation of a material analysis of tumor markers.Citation23 Further analyses were performed to identify low-cost and widely available data on hematological parameters in this group of patients.
The NLR may act as a marker for the evaluation of the systemic balance between pro-tumor inflammation associated with neutrophils and antitumor immune response associated with lymphocytes. An increased NLR may indicate a trend for decreased antitumor immune capacity and increased pro-tumor inflammation.Citation24 In another study,Citation25 a higher NLR was associated with more advanced disease stage in younger patients. More advanced disease stage and elevated pretreatment NLR in patients with CA in our study were significantly associated with poorer RFS and OS. This finding is in accordance with previous studies reporting that the pretreatment NLR is associated with survival in patients with other malignancies as well as cervical cancer, especially those with advanced disease.Citation26,Citation27 Zhang et al demonstrated the poor prognostic influence of NLR on RFS, but not OS, in cervical carcinoma patients treated with surgery. They found that an elevated NLR was associated with lymph node metastases (LNM) and the depth of stromal infiltration.Citation28 In patients with cervical squamous cell carcinoma treated with CCRT, NLR was a highly significant prognostic factor for RFS and OS. Moreover, a low NLR was significantly associated with a complete response to treatment with CCRT.Citation29 In an analysis by Huang et al, a high pretreatment NLR was an adverse prognostic factor for OS and RFS and was also significantly associated with FIGO stage, LNM, and tumor size.Citation30 The prognostic value of pretreatment NLR was confirmed in a study of patients with a wide range of malignancies.Citation31 In a study of cervical cancer treated with RT, Cho et al reported that an increased NLR was associated with a poorer treatment response and more aggressive disease.Citation32
Our results also confirmed that more advanced FIGO stage and elevated NLR were significantly associated with a poorer outcome. Wang et al did not confirm the predictive values of NLR and PLR in cervical cancer patients treated with neoadjuvant chemotherapy and surgery.Citation33 However, our study did not include these patients.
Besides low lymphocyte values, thrombocytosis has also been reported as a marker of host systemic inflammation. Its prognostic value in malignancies has been confirmed.Citation34–Citation37 Pretreatment peripheral PLR has been shown to have prognostic value for LNM and clinical outcome in early cervical cancer treated with surgery.Citation38 According to Nakamura et al, the pretreatment PLR may be an independent predictor of recurrence in cervical cancer patients treated with CCRT.Citation39 The findings of our study demonstrated that pretreatment PLR was significantly correlated with the prognosis of CA patients treated with RT/CCRT. Elevated pretreatment PLR in patients with FIGO stage IIB–IV disease treated with RT/CCRT negatively impacted the OS. Once confirmed in a larger study group, these results have significant potential for wider application in practice. Considering that CA histology has been reported to be a poor prognostic factor for worse response to CCRT, this is a unique information with regard to this group of patients. Therefore, it seems reasonable to consider whether this particular group should not be subjected to complementary treatments such as targeted therapy or the addition of anti-inflammatory agents.
Leukocytes, being at the center of the inflammatory response to tumor formation, have been the subject of evaluation in many studies on colorectal and lung cancers.Citation12,Citation40 The results of our study demonstrated that elevated pretreatment values of WBC in patients with cervical carcinoma were related to a shorter OS. The findings of other study confirmed that WBC may predict survival in these patients. The prognostic value of WBC in cervical cancer has been demonstrated in other studies.Citation25,Citation34,Citation41 The total WBC may be a significant addition to the other established markers of systemic inflammation, including albumin, CRP, lymphocytes counts, neutrophil, prognostic nutritional index, and their combination.Citation26,Citation42,Citation43 The results of our study suggest that inflammatory components such as lymphocytes, PLT, neutrophils, and WBC play a critical role in the development and progression of CA. The specific relationships between these components and poor survival are yet to be elucidated. However, pretreatment lymphocyte and neutrophil numbers indicate the level of systemic inflammation.Citation44–Citation46 Inflammation may change the tumor microenvironment and lead to promotion of angiogenesis and metastasis.Citation25,Citation47,Citation48 Moreover, circulating lymphocytes may secrete cytokines that play a role in preventing proliferation and metastatic process and in cytotoxicity. Lower lymphocyte levels and NLR imbalance may promote progression of malignancy. More advanced cancer stage may significantly affect hematological parameters, unlike smaller tumors. Thus, the NLR reflects the balance between inflammatory and immune responses.Citation19,Citation49 Moreover, more advanced FIGO stage (FIGO IIB-IVA) in patients with CA is a poor prognostic factor for OS; in our study, treatment with RT/CCRT was related to a poor prognosis, probably related to the disease severity. However, we have to consider that this is the treatment of choice for this group of patients, and our study aimed to identify inexpensive markers that can be conveniently used for patient identification. Based on the results of the studies available in the literature, and analyzing the relationship between the value of the assessed parameters and the survival of patients, we can conclude that they may have a prognostic value. We also know that the inflammation process may promote the cancer progression. We assume that an unfavorable prognosis of patients with adenocarcinoma of the cervix is not a result of the increased value of the analyzed parameters. Elevated parameters seem to be a symptom of cancer advancement and evidence that a value of coefficients reflects the fact that after exceeding a limit, the tumor mass is so high that the chances for a favorable treatment outcome are drastically reduced. Future studies are necessary to assess additive, alternative, or more effective treatment regimens.
The strength of our study was the large group of patients with CA and the long follow-up, which presented mature results. To our knowledge, this is the first report on the influence of inflammatory parameters on the outcome of patients with CA. The weakness of our study is its retrospective nature and single institution experience. However, if proven in future clinical studies, WBC, NLR, and PLR might be novel, relatively easily available, and inexpensive prognostic markers that help in guiding therapeutic methods and identifying CA patients with high-risk profiles. A histological type, characterized by a poorer prognosis among patients with cervical cancer and concerning an increasingly younger population, our study identified high-risk patients with CA FIGO IIB– IV and elevated WBC, NLR, and PLR before treatment. If confirmed in larger cohorts, these hematological parameters and ratios may identify patients who may respond to anti-inflammatory treatment.
Conclusion
To our knowledge, this is the largest report of CA patients with mature data. We first demonstrated the prognostic significance of pretreatment PLR, NLR, and WBC values on the survival of patients with CA. Furthermore, the combination of NLR and PLR may enable risk stratification for survival prediction. These parameters can be derived directly from routine blood cell counts, making it an easily available marker for individual risk assessment and stratification of patients with uterine CA, in addition to the clinical stage. Changes in blood NLR and PLR might have utility in tailored therapy, especially in advanced stages that lack reliable markers.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- Bodner-AdlerBKimbergerOSchneidingerCKölblHBodnerKPrognostic significance of pre-treatment serum C-reactive protein level in patients with adenocarcinoma of the uterine cervixAnticancer Res20163694691469627630314
- SmallWBaconMABajajACervical cancer: a global health crisisCancer2017123132404241228464289
- YokoiEMabuchiSTakahashiRImpact of histological subtype on survival in patients with locally advanced cervical cancer that were treated with definitive radiotherapy: adenocarcinoma/adenosquamous carcinoma versus squamous cell carcinomaJ Gynecol Oncol2017282e1928028992
- RosePGAre the differences in treatment outcome for adenocarcinoma of the cervix different enough to change the treatment paradigm?Gynecol Oncol2012125228528622482933
- WilliamsNLWernerTLJarboeEAGaffneyDKAdenocarcinoma of the cervix: should we treat it differently?Curr Oncol Rep20151741725708801
- WrightAAHowittBEMyersAPOncogenic mutations in cervical cancer: genomic differences between adenocarcinomas and squamous cell carcinomas of the cervixCancer2013119213776338324037752
- TorneselloMLBuonaguroLBuonaguroFMMutations of the TP53 gene in adenocarcinoma and squamous cell carcinoma of the cervix: a systematic reviewGynecol Oncol2013128344244823168175
- GomezDFaridSMalikHZPreoperative neutrophil-to-lymphocyte ratio as a prognostic predictor after curative resection for hepatocellular carcinomaWorld J Surg20083281757176218340479
- HeflerLAConcinNHofstetterGSerum C-reactive protein as independent prognostic variable in patients with ovarian cancerClin Cancer Res200814371071418245530
- JablonskaEPuzewskaWGrabowskaZJablonskiJTalarekLVEGF, IL-18 and NO production by neutrophils and their serum levels in patients with oral cavity cancerCytokine2005303939915826815
- ArdiVCKupriyanovaTADeryuginaEIQuigleyJPHuman neutrophils uniquely release TIMP-free MMP-9 to provide a potent catalytic stimulator of angiogenesisProc Natl Acad Sci U S A200710451202622026718077379
- Di CarloEForniGMusianiPNeutrophils in the antitumoral immune responseChem Immunol Allergy20038318220312947985
- YinYWangJWangXPrognostic value of the neutrophil to lymphocyte ratio in lung cancer: A meta-analysisClinics201570752453026222823
- SugiuraTUesakaKKanemotoHMizunoTOkamuraYElevated preoperative neutrophil-to-lymphocyte ratio as a predictor of survival after gastroenterostomy in patients with advanced pancreatic adenocarcinomaAnn Surg Oncol201320134330433723982254
- LeeSOhSYKimSHPrognostic significance of neutrophil lymphocyte ratio and platelet lymphocyte ratio in advanced gastric cancer patients treated with FOLFOX chemotherapyBMC Cancer20131335023876227
- JinHZhangGLiuXBlood neutrophil-lymphocyte ratio predicts survival for stages III-IV gastric cancer treated with neoadjuvant chemotherapyWorld J Surg Oncol20131111223705622
- PichlerMHuttererGCStoeckigtCValidation of the pretreatment neutrophil-lymphocyte ratio as a prognostic factor in a large European cohort of renal cell carcinoma patientsBr J Cancer2013108490190723385728
- JankovaLDentOFChanCChapuisPClarkeSJPreoperative neutrophil/lymphocyte ratio predicts overall survival but does not predict recurrence or cancer-specific survival after curative resection of node-positive colorectal cancerBMC Cancer20131344224079717
- DingPRAnXZhangRXElevated preoperative neutrophil to lymphocyte ratio predicts risk of recurrence following curative resection for stage IIA colon cancerInt J Colorectal Dis201025121427143320821217
- GalonJCostesASanchez-CaboFType, density, and location of immune cells within human colorectal tumors predict clinical outcomeScience200631357951960196417008531
- JungEJByunJMKimYNCervical adenocarcinoma has a poorer prognosis and a higher propensity for distant recurrence than squamous cell carcinomaInt J Gynecol Cancer20172761228123628604449
- GalicVHerzogTJLewinSNPrognostic significance of adenocarcinoma histology in women with cervical cancerGynecol Oncol2012125228729122266551
- KotowiczBKaminskaJFuksiewiczMClinical significance of serum CA-125 and soluble tumor necrosis factor receptor type I in cervical adenocarcinoma patientsInt J Gynecol Cancer201020458859220686378
- MosesKBrandauSHuman neutrophils: Their role in cancer and relation to myeloid-derived suppressor cellsSemin Immunol201628218719627067179
- LeeYYChoiCHKimHJPretreatment neutrophil:lymphocyte ratio as a prognostic factor in cervical carcinomaAnticancer Res20123241555156122493401
- ProctorMJMcMillanDCMorrisonDSFletcherCDHorganPGClarkeSJA derived neutrophil to lymphocyte ratio predicts survival in patients with cancerBr J Cancer2012107469569922828611
- WangLJiaJLinLPredictive value of hematological markers of systemic inflammation for managing cervical cancerOncotarget2017827448244483228148894
- ZhangYWangLLiuYPreoperative neutrophil-lymphocyte ratio before platelet-lymphocyte ratio predicts clinical outcome in patients with cervical cancer treated with initial radical surgeryInt J Gynecol Cancer20142471319132525033256
- MizunumaMYokoyamaYFutagamiMAokiMTakaiYMizunumaHThe pretreatment neutrophil-to-lymphocyte ratio predicts therapeutic response to radiation therapy and concurrent chemoradiation therapy in uterine cervical cancerInt J Clin Oncol201520598999625736530
- HuangQTManQQHuJPrognostic significance of neutrophil-to-lymphocyte ratio in cervical cancer: A systematic review and meta-analysis of observational studiesOncotarget2017810167551676428187430
- TempletonAJMcNamaraMGŠerugaBPrognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysisJ Natl Cancer Inst20141066dju12424875653
- ChoYKimKHYoonHIKimGEKimYBTumor-related leukocytosis is associated with poor radiation response and clinical outcome in uterine cervical cancer patientsAnn Oncol201627112067207427502717
- WangDWuMFengFZPretreatment neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios do not predict survival in patients with cervical cancer treated with neoadjuvant chemotherapy and radical hysterectomyChin Med J201312681464146823595378
- KoseMCelikFKoseSKAriozDTYilmazerMCould the platelet-to-lymphocyte ratio be a novel marker for predicting invasiveness of cervical pathologies?Asian Pac J Cancer Prev201516392392625735383
- SmithRABosonnetLGhanehPThe platelet-lymphocyte ratio improves the predictive value of serum CA19-9 levels in determining patient selection for staging laparoscopy in suspected periampullary cancerSurgery2008143565866618436014
- AcmazGAksoyHUnalDAre neutrophil/lymphocyte and platelet/lymphocyte ratios associated with endometrial precancerous and cancerous lesions in patients with abnormal uterine bleeding?Asian Pac J Cancer Prev20141541689169224641391
- KozasaKMabuchiSKomuraNComparison of clinical utilities of the platelet count and platelet-lymphocyte ratio for predicting survival in patients with cervical cancer: a single institutional study and literature reviewOncotarget2017833553945540428903428
- ChenLZhangFShengXGZhangSQChenYTLiuBWPeripheral platelet/lymphocyte ratio predicts lymph node metastasis and acts as a superior prognostic factor for cervical cancer when combined with neutrophil: LymphocyteMedicine20169532e438127512849
- NakamuraKNishidaTHarumaTPretreatment platelet-lymphocyte ratio is an independent predictor of cervical cancer recurrence following concurrent chemoradiation therapyMol Clin Oncol2015351001100626623040
- SpragueBLTrentham-DietzAKleinBEPhysical activity, white blood cell count, and lung cancer risk in a prospective cohort studyCancer Epidemiol Biomarkers Prev200817102714272218843014
- Tavares-MurtaBMMendonçaMADuarteNLSystemic leukocyte alterations are associated with invasive uterine cervical cancerInt J Gynecol Cancer20102071154115921495217
- HaragaJNakamuraKOmichiCPretreatment prognostic nutritional index is a significant predictor of prognosis in patients with cervical cancer treated with concurrent chemoradiotherapyMol Clin Oncol20165556757427900086
- GelbandHSankaranarayananRGauvreauCLCosts, affordability, and feasibility of an essential package of cancer control interventions in low-income and middle-income countries: key messages from Disease Control Priorities, 3rd editionLancet2016387100332133214426578033
- OnalCGulerOCYildirimBAPrognostic Use of pretreatment hematologic parameters in patients receiving definitive chemoradiotherapy for cervical cancerInt J Gynecol Cancer20162661169117527206286
- WangYYBaiZLHeJLPrognostic value of neutrophil-related factors in locally advanced cervical squamous cell carcinoma patients treated with cisplatin-based concurrent chemoradiotherapyDis Markers2016201619
- ZhengRRHuangMJinCCervical cancer systemic inflammation score: a novel predictor of prognosisOncotarget2016712152301524226885692
- MantovaniAAllavenaPSicaABalkwillFCancer-related inflammationNature2008454720343644418650914
- BalkwillFMantovaniAInflammation and cancer: back to Virchow?Lancet2001357925553954511229684
- ParamanathanASaxenaAMorrisDLA systematic review and meta-analysis on the impact of pre-operative neutrophil lymphocyte ratio on long term outcomes after curative intent resection of solid tumoursSurg Oncol2014231313924378193