
Abstract
Background
Ewing’s sarcoma (ES) is a highly aggressive and metastatic neoplasm occurring mainly in children and young adults. The standard treatment of localized ES requires a combination of surgery, chemotherapy, and radiotherapy. Although the 5-year survival rate for local ES has improved, the survival rate and prognosis are still very poor for metastatic or recurrent ES patients. The aim of this study was to investigate the efficacy and safety of apatinib, a specific vascular endothelial growth factor receptor 2 inhibitor, in ES patients.
Methods
This retrospective analysis involved eleven patients with ES not amenable to curative treatment. All patients suffered poor responses to two cycles of chemotherapy (vincristine, doxorubicin, and cyclophosphamide). Apatinib 500 mg (or 250 mg) was given daily. Tumor responses were assessed according to the Response Evaluation Criteria in Solid Tumors 1.1. Survival analysis was performed by the Kaplan–Meier test. The safety profile was also recorded.
Results
The mean age of the patients was 18 (range, 10–31) years. The 12-month overall survival and progression-free survival rates were 90% and 72%, respectively. Four patients achieved partial response, and four patients achieved stable disease, with objective response rate of 40%. The median follow-up in our study was 16 months (range, 3–26 months). The most common adverse events included hand–foot skin reaction (n=5; 45%), oral ulcers (n=4; 36%), and gastrointestinal discomfort (n=4; 36%).
Conclusion
Apatinib may provide as second- or first-line treatment options for ES patients, particularly in chemoresistant cases. Further studies with more cases and longer follow-up will be necessary to determine the clinical efficacy and safety of apatinib in ES patients.
Introduction
Ewing sarcoma family tumors (ESFTs) are a group of aggressive neoplasms of the bone and soft tissue, characterized histologically by small, round, blue cells. ESFTs mainly occur in adolescents and young adults, between ages 10 and 20 years, as primitive neuroectodermal tumor. Specifically, they are malignant small-cell tumors of the thoracopulmonary region and classic Ewing sarcomas of the bone and soft tissue.Citation1,Citation2 Ewing’s sarcoma (ES) is characterized by chromosomal translocation involving the Ewing sarcoma breakpoint region 1 (EWSR1) gene, and 85% of cases are associated with translocations of EWSR1 on chromosome 22 to chromosome 11.Citation2,Citation3
Nearly 27% of ES patients are found to have metastatic lesions at diagnosis, and the remaining patients have localized cancer.Citation4 A multidisciplinary approach including risk-adapted chemotherapy and local therapy (surgery and radiation therapy) has significantly increased the survival of patients with localized disease.Citation5 However, the prognosis of advanced ES patients is still grave, with 5-year survival rates of only 20%–30%.Citation6,Citation7 According to the Clinical Practice Guideline of the National Comprehensive Cancer Network, the first-line treatment with systemic therapy is recommended, including vincristine, doxorubicin, cyclophosphamide, ifosfamide, and etoposide. Nevertheless, the second-line therapy of ES depends on previous completion of adjuvant therapy and first-line treatment, as well as patient’s tolerance.
Several second-line chemotherapy regimens have been recommended for refractory or recurrent ES,Citation8,Citation9 cancers that are typically refractory to conventional chemotherapy and irradiation.Citation10 In addition, there are still no randomized studies comparing different regimens for the second-line chemotherapy treatments. Moreover, the best second-line regimens have not been identified, and further investigation will be required to identify them.
Apatinib is a novel receptor tyrosine kinase inhibitor that selectively competes for the vascular endothelial growth factor receptor 2 (VEGFR-2) ATP-binding site, blocking downstream signaling, and inhibiting tumor angiogenesis.Citation11,Citation12 Apatinib has been reported to improve progression-free survival (PFS), and consequently overall survival (OS), in patients with advanced gastric cancer.Citation13 It is thought to be a potentially useful agent to expand the therapeutic options in various sarcomas, including angiosarcoma, malignant fibrous histiocytoma, and myxoid/round cell liposarcoma.Citation14,Citation15
To our best knowledge, there are no prior reports on the effects of apatinib on ES, and therefore, the aim of this study was to investigate the efficacy and safety of apatinib, a specific VEGFR-2 inhibitor, in patients with these cancers. We conducted a retrospective cohort study to investigate the association of antiangiogenesis-related adverse events (AEs) with clinical outcomes in ES patients and to report the data from a total of eleven of these patients treated with apatinib. Our report describes the usage, safety, and efficacy of apatinib in ES patients, who were being treated in the Department of Orthopedics at West China Hospital.
Patients and methods
Eligibility criteria
The study was conducted retrospectively on patients treated between February 1, 2016, and January 1, 2018. The inclusion criteria included 1) histologically proven ES, 2) initial treatment in the Department of Orthopedics of West China Hospital, 3) tumors that were not amenable to curative treatment (with unresectable lesions or distant metastasis), 4) measur able lesions according to Response Evaluation Criteria for Solid Tumors (RECIST),Citation16 5) an Eastern Cooperative Oncology Group performance status 0 or 1, and 6) chemotherapy rejection or at least two prior cycles of chemotherapy, including VAC (vincristine, doxorubicin, and cyclophosphamide) or VAIE (vincristine, doxorubicin, and cyclophosphamide alternating with ifosfamide and etoposide).
Treatment methods
Because these patients had not responded to conventional chemotherapy, apatinib was administered at a dose of 500 mg once daily. For patients younger than 10 years, we used 250 mg once daily.Citation17 One treatment cycle was 28 days long. One dose reduction (to 250 mg) or interruptions of therapy for drug-related toxicity was allowed. Dose-limiting toxicity was defined as possibly or definitely drug-related grades 3–4 toxic responses. This study was performed according to the principles embodied in the Declaration of Helsinki and the Institutional Review Board of Sichuan University West China Hospital. Written informed consent was obtained from all patients when they began treatment for apatinib. The study protocol followed all appropriate guidelines according to the Declaration of Helsinki.
Evaluation of efficacy and safety
In this retrospective study, we were mainly concerned with documenting the objective response rate (ORR), including complete response and partial response (PR) cases, as well as the PFS for each apatinib protocol according to RECIST 1.1. Moreover, OS and toxicities encountered in the study were also recorded. Treatment efficacy was evaluated by computed tomography (CT) or magnetic resonance imaging. The safety evaluation was based on the frequency and severity of events assessed according to the Common Terminology Criteria for Adverse Events.Citation18 Kaplan–Meier survival curves were used for PFS estimation. Data analyses were performed using SPSS 20.0 software (IBM Corporation, Armonk, NY, USA).
Results
Patients’ characteristics
From February 1, 2016, to January 1, 2018, eleven consecutive advanced ES patients were enrolled. All pathologic diagnoses were confirmed at West China Hospital. Patients’ clinical characteristics at entry to the study are summarized in . One patient was lost to follow-up, and one patient stopped using apatinib because of toxicity. Median followup time was 15.8 months (range, 3.0–26.0 months). Before treatment with apatinib, first line of prior chemotherapy was administrated for at least two cycles. Seven patients (63.6%) had metastasis at initial presentation (including lung, spine, and bone metastasis).
Table 1 Patients’ characteristics
Treatment methods
Among eleven patients, five (45.4%) patients received chemotherapy, local surgery, and then apatinib. Another five (45.4%) patients received apatinib and chemotherapy in combination, and stable disease (SD) was achieved. The last one (9.2%) patient received only apatinib, because chemotherapy was rejected after a lung metastasis was found at the initial diagnosis ().
Table 2 Different treatment combinations and response
All eleven patients were evaluated by physicians in our clinic on a monthly basis and with at least chest CT and imaging of tumor lesions at other sites.
Efficacy
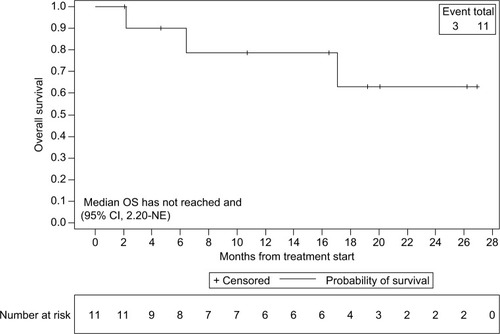
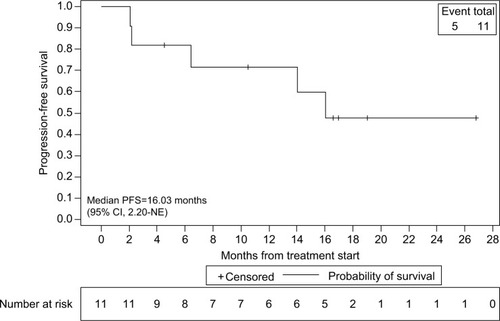
By the last scheduled visit (), one patient was lost to follow-up and one patient died of lung metastasis. The median PFS was 16.0 months (95% CI). Four (40%) of ten patients had PRs (), and four (40%) had SD (). Two (20%) patients developed progressive disease (PD). The 6- and 12-month OS rates were 90.0% and 78.8%, respectively. Moreover, the 6- and 12-month PFS rates were 81.8% and 71.6%, respectively ( and ). The ORR was 40% (4/10) for ES.
Table 3 Clinical characteristics of eleven Ewing sarcoma patients treated with apatinib
Table 4 Patients’ clinical evaluations
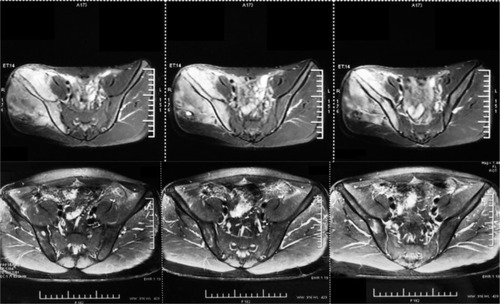
Figure 1 The patient with PR showing response to the treatment with apatinib.
Figure 2 Kaplan–Meier estimates of PFS for all patients.
Figure 3 Kaplan–Meier estimates of OS for all patients.
Abbreviation: OS, overall survival.
Abbreviation: PFS, progression-free survival.
Note: MRIs of the pelvis are shown before and after treatment.
Abbreviations: MRI, magnetic resonance imaging; PR, partial response.
Safety and toxicity
The treatment was interrupted in one (10%) patient because of hand–foot syndrome. Two patients (15- and 19-year-old males) died of lung metastasis because of respiratory failure. Toxicities encountered in the study are listed in . Most adverse reactions were mild (grades 1–2) and easily controlled. However, some more serious adverse reactions occurred and were of variable severity. The only grade 3 reaction was hand–foot syndrome.
Table 5 Adverse events
Discussion
ES is aggressive with high metastatic tendency and can develop resistance to conventional chemotherapy.Citation19 The mechanisms by which ES become resistant to chemotherapy are varied and can involve inherent resistance of the cancer stem cells, drug metabolizing enzymes, modulation of cellular signal transduction pathways, and tumor heterogeneity.Citation19
Several phase I and II clinical trials have reported investigational therapies for ES, including insulin growth factor-receptor antibody, mammalian target of rapamycin inhibition, poly ADP-ribose polymerase inhibition, telomerase inhibition, Akt, nuclear factor κB, BRAF, and vascular endothelial growth factor (VEGF).Citation20–Citation22 Owing to obvious side effects and translation failure of these observations into clinical strategies, multiple parallel pathways and cellular processes will need further investigation.
Among these possible therapeutic targets, VEGF has been highlighted in ES cell lines. Inhibition or blockade of VEGF can result in the suppression of ES tumor growth.Citation23 There also appears to be an association of VEGF expression with poor prognosis of ES patients.Citation24–Citation28 VEGF has an important role in tumor angiogenesis and vasculogenesis. Although there are many subtypes of VEGF, VEGFR-2 is the key mediator of the recognized VEGF-induced phenotypes.Citation29 Apatinib, a specific VEGFR-2 inhibitor, was licensed by the China Food and Drug Administration for the treatment of advanced/metastatic gastric cancer and adenocarcinomas of the gastroesophageal junction in 2014. Its anticancer effects have been reported in a broad range of malignancies such as osteosarcoma, rhabdomyosarcoma, synovial sarcoma, and alveolar soft part sarcoma.Citation17,Citation30
Previous studies have evaluated the response of advanced bone and soft tissue sarcomas to apatinib. Zhu et alCitation30 reported an ORR of 33.3% when apatinib was administered as a second-line or further-line treatment. Xie et al reported, as a second-line or further-line treatment, the ORR was 40.9% (9/22) for osteosarcoma, 70%(7/10) for ES, 100% (3/3 cases) for chondrosarcoma, and 71.4% (15/21) for soft tissue sarcoma.Citation17 Thus, apatinib was a third-line treatment option for one ES patient in our study, with the result encouraging as a PR. In fact, apatinib has been reported as a first-line treatment for off-label use.Citation31,Citation32 Therefore, we attempted to use apatinib as a second- or first-line treatment option for ES patients, particularly in cases resistant to chemotherapy and five of the ten ES patients took apatinib together with chemotherapy. Apatinib also was administered as a first-line treatment option for advanced ES patients in this study. Median follow-up in our study was 16.0 months, and one patient (10%) achieved a PD, two (20%) achieved SD, and two (20%) achieved PR. For four patients (40%) used apatinib as second-line treatment, one (10%) achieved a PD, two (20%) achieved a SD, and one (10%) developed a PR. In our study, the ORR with apatinib was 40% (4/10) in ES. Although Xie et al reported that their objective ORR was 70% (7/10) for ES patients, and our ORR rate was 40% (4/10), their patients met endpoints in a short period. We have achieved 12-month OS and PFS rates of 90.0% and 71.6%, respectively. As most patients are still assessed as having PR or SD, the duration of response of patients could not be evaluated. Apatinib was administered at a dose of 500 mg/day for adolescents and adults and 250 mg/dayCitation30 for patients younger than 10 years, dosing that is lower than that used in the previous trials. Therefore, our ORR may have been limited by the lower drugs doses.
For the AEs, the most common toxicities are fatigue, hypertension, and hand–foot skin reaction (HFS).Citation30 Importantly, only one patient had to stop using apatinib as a result of toxicity (HFS). Four patients had oral ulcers and weight loss. Five of our patients had treatment-related gastrointestinal discomfort, and one patient had delayed wound healing. None of our patients had hypertension. Interestingly, previous studies reported that patients with grade 3/4 toxicities had a longer PFS than those without grade 3/4 toxicities, especially for patients with hypertension and HFS.Citation33 Similar results were found in our study.
We recognize that our study has some limitations. First, as a retrospective study, most patients had combined chemotherapy. Therefore, it is not strictly correct to draw comparisons with the used of apatinib and other drugs. Second, the inclusion criteria utilized were not as rigorous as those employed in formal prospective trials. Third, because only eleven ES patients were enrolled in our study, we had insufficient numbers to permit subset analyses and limited statistical power. Fourth, the dose of 250 mg apatinib adopted in this study for some patients was not widely recommended.
Conclusion
This study provides preliminary evidence of efficacy of apatinib in patients with advanced ES. Apatinib may prove to be a second-line or even a first-line treatment option for advanced ES patients, particularly in cases resistant to chemotherapy. Further studies with more patients and longer follow-up times will be necessary to fully determine the clinical efficacy of apatinib in ES. Indeed, it is likely that formal multicenter randomized clinical trials will be required to fully establish the effects of apatinib on ES patients.
Ethical statement
To preserve patient confidentiality and privacy, patient data have been deidentified before analysis. This retrospective study was performed based on the data from anonymized patients who received apatinib treatment between February 2016 and January 2018. Because of the nature of retrospective design and patient anonymization, the ethical board of Sichuan University West China Hospital approved the retrospective study and also determined that informed consent was not required.
Acknowledgments
This work was supported, in part, by National Natural Science Foundation of China (81702664). This abstract was selected for online publication presenting interim findings only, at the 2018 ASCO Annual Meeting, taking place on June 1–5, 2018, at the McCormick Place Convention Center in Chicago, Illi-nois (Abstract Submission ID: 211471; Password: 210783). The abstract was released by ASCO on May 16, 2018, at 5:00 PM EDT on meetinglibrary.asco.org.
Disclosure
The authors report no conflicts of interest in this work.
References
- RosenGWollnerNTanCProceedings: disease-free survival in children with Ewing’s sarcoma treated with radiation therapy and adjuvant four-drug sequential chemotherapyCancer19743323843934812758
- BurchillSAMolecular abnormalities in Ewing’s sarcomaExpert Rev Anticancer Ther20088101675168718925858
- JiangYLudwigJJankuFTargeted therapies for advanced Ewing sarcoma family of tumorsCancer Treat Rev201541539140025869102
- EsiashviliNGoodmanMMarcusRBChanges in incidence and survival of Ewing sarcoma patients over the past 3 decades: Surveillance Epidemiology and End Results dataJ Pediatr Hematol Oncol200830642543018525458
- KrasinMJDavidoffAMRodriguez-GalindoCDefinitive surgery and multiagent systemic therapy for patients with localized Ewing sarcoma family of tumors: local outcome and prognostic factorsCancer2005104236737315948159
- CotterillSJAhrensSPaulussenMPrognostic factors in Ewing’s tumor of bone: analysis of 975 patients from the European Intergroup Cooperative Ewing’s Sarcoma Study GroupJ Clin Oncol200018173108311410963639
- van MaldegemAMBensonCRutkowskiPEtoposide and carbo- or cisplatin combination therapy in refractory or relapsed Ewing sarcoma: a large retrospective studyPediatr Blood Cancer2015621404425251256
- FoxEPatelSWathenJKPhase II study of sequential gemcitabine followed by docetaxel for recurrent Ewing sarcoma, osteosarcoma, or unresectable or locally recurrent chondrosarcoma: results of Sarcoma Alliance for Research Through Collaboration Study 003Oncologist201217332122363068
- RaciborskaABilskaKDrabkoKVincristine, irinotecan, and temozolomide in patients with relapsed and refractory Ewing sarcomaPediatr Blood Cancer201360101621162523776128
- ArpaciEYetisyigitTSekerMPrognostic factors and clinical outcome of patients with Ewing’s sarcoma family of tumors in adults: multicentric study of the Anatolian Society of Medical OncologyMed Oncol201330146923345116
- LiJZhaoXChenLSafety and pharmacokinetics of novel selective vascular endothelial growth factor receptor-2 inhibitor YN968D1 in patients with advanced malignanciesBMC Cancer20101052920923544
- DingJChenXGaoZMetabolism and pharmacokinetics of novel selective vascular endothelial growth factor receptor-2 inhibitor apatinib in humansDrug Metab Dispos20134161195121023509226
- LiJQinSXuJRandomized, double-blind, placebo-controlled phase III trial of apatinib in patients with chemotherapy-refractory advanced or metastatic adenocarcinoma of the stomach or gastroesophageal junctionJ Clin Oncol201634131448145426884585
- JiGHongLYangPSuccessful treatment of angiosarcoma of the scalp with apatinib: a case reportOnco Targets Ther201694989499227563253
- JiGHongLYangPSuccessful treatment of advanced malignant fibrous histiocytoma of the right forearm with apatinib: a case reportOnco Targets Ther201694989499227563253
- TaylorPTHaverstickDRe: new guidelines to evaluate the response to treatment in solid tumors (ovarian cancer)J Natl Cancer Inst200597215115657346
- XieLGuoWWangYYanTJiTXuJApatinib for advanced sarcoma: results from multiple institutions’ off-label use in ChinaBMC Cancer201818139629625604
- de RojasTBautistaFJMaderoLMorenoLThe first step to integrating adapted common terminology criteria for adverse events for childrenJ Clin Oncol201634182196219727114600
- AhmedAAZiaHWagnerLTherapy resistance mechanisms in Ewing’s sarcoma family tumorsCancer Chemother Pharmacol201473465766324469502
- VornicovaOBar-SelaGInvestigational therapies for Ewing sarcoma: a search without a clear findingExpert Opin Investig Drugs2016256679686
- ArnaldezFIHelmanLJNew strategies in Ewing sarcoma: lost in translation?Clin Cancer Res201420123050305624756371
- NaingALorussoPFuSInsulin growth factor-receptor (IGF-1R) antibody cixutumumab combined with the mTOR inhibitor temsirolimus in patients with refractory Ewing’s sarcoma family tumorsClin Cancer Res20121892625263122465830
- YudohKKanamoriMOhmoriKYasudaTAokiMKimuraTConcentration of vascular endothelial growth factor in the tumour tissue as a prognostic factor of soft tissue sarcomasBr J Cancer200184121610161511401313
- YudohKKanamoriMOhmoriKYasudaTAokiMKimuraTConcentration of vascular endothelial growth factor in the tumour tissue as a prognostic factor of soft tissue sarcomasBr J Cancer200184121610161511401313
- DalalSBerryAMCullinaneCJVascular endothelial growth factor: a therapeutic target for tumors of the Ewing’s sarcoma familyClin Cancer Res20051162364237815788688
- ZhouZBolontradeMFReddyKSuppression of Ewing’s sarcoma tumor growth, tumor vessel formation, and vasculogenesis following anti vascular endothelial growth factor receptor-2 therapyClin Cancer Res200713164867487317699866
- AhmedAAShermanAKPawelBRExpression of therapeutic targets in Ewing sarcoma family tumorsHum Pathol20124371077108322196127
- KreuterMPaulussenMBoeckelerJClinical significance of vascular endothelial growth factor-A expression in Ewing’s sarcomaEur J Cancer200642121904191116824746
- AutieroMWaltenbergerJCommuniDRole of PlGF in the intra- and intermolecular cross talk between the VEGF receptors Flt1 and Flk1Nat Med20039793694312796773
- ZhuBLiJXieQDiaoLGaiLYangWEfficacy and safety of apatinib monotherapy in advanced bone and soft tissue sarcoma: an observational studyCancer Biol Ther201819319820429261005
- WangYBiMZhangHGaoZZhouHChangSApatinib in gastric carcinoma: a case report of partial response for first-line treatment in advanced diseaseAsia Pac J Clin Oncol2017135e528e53028028915
- DongMBiJLiuXWangBWangJSignificant partial response of metastatic intra-abdominal and pelvic round cell liposarcoma to a small-molecule VEGFR-2 tyrosine kinase inhibitor apatinib: a case reportMedicine20169531e436827495042
- LiJWangLEfficacy and safety of apatinib treatment for advanced esophageal squamous cell carcinomaOnco Targets Ther2017103965396928860804