
Abstract
Purpose
Acute myeloid leukemia patients are commonly treated with cytarabine (Ara-C) and anthracyclines but the sustained remission rate is not very promising. We explored the role of drug-metabolizing enzymes and transporters in the therapeutic response.
Patients and methods
Bone marrow and peripheral blood samples of 90 newly diagnosed acute myeloid leukemia patients treated with standard 3+7 regimen were analyzed through real-time PCR for expression of human equilibrative nucleoside transporter 1, deoxycytidine kinase, cytidine deaminase (CDA), deoxycytidine monophosphate deaminase (dCMPD) and topoisomerase IIα (Topo-IIa). The expression of these markers was studied in relationship with good (persistent remission) and poor therapeutic response (relapse/resistance).
Results
High Topo-IIa expression in peripheral blood was associated with good response (P=0.006). Relapse was higher among low expressors of Topo-IIa in peripheral blood (OR: 26.25). Bone marrow Topo-IIa expression followed a similar trend but did not reach statistical significance. In contrast, patients with high bone marrow dCMPD expression had poor response (OR: 3; P=0.043). One-year disease-free survival (DFS) was better among those with high bone marrow Topo-IIa (P=0.04) or CDA (P=0.03) expression. High bone marrow Topo-IIa expression also had better DFS at 6 months (P=0.04) and at 12 months (P=0.04).
Conclusion
High expression of Topo-IIa in peripheral blood is a favorable indicator of persistent remission, good therapeutic response and DFS. High dCMPD and low CDA expression in bone marrow is associated with poor therapeutic outcome.
Introduction
Acute myeloid leukemia (AML) is mainly treated with chemotherapy regimen comprising of cytarabine and anthracyclines.Citation1 Treatment of AML is often complicated by resistance to conventional chemotherapy, which reflects the survival of tumor cells despite exposure to cytotoxic chemotherapeutic agents.Citation2,Citation3 This has been a major problem in effective cancer treatment.Citation4 Therapeutic response depends on availability of drug at the target tissue where it inflicts damage to the malignant cells. Therefore, sensitivity and resistance to a drug could be influenced by the expression of drug transporters, drug metabolizing enzymes, and thus availability of sufficient drug at target receptors.
Human equilibrative nucleoside transporter 1 (hENT1) or solute carrier family 29 member 1 is a transmembrane glycoprotein present in cell and mitochondrial membranes. It is primarily involved in importing nucleosides for salvage pathway of purine and pyrimidine nucleosides. Cytotoxic nucleoside analogs, such as cytarabine (Ara-C), also utilize this transporter to enter cells.Citation5 Thus, efficiency of Ara-C influx can determine the intracellular drug level and thereby response to chemotherapy.Citation6
Deoxycytidine kinase (dCK) is the rate-limiting enzyme of salvage pathway that phosphorylates nucleoside analogs, including Ara-C and gemcitabine to respective monophosphates. These monophosphates are phosphorylated by various kinases to diphosphates and triphosphates, which are in turn utilized for DNA synthesis. These Ara-C nucleotides inhibit DNA replication and transcription by inhibiting DNA and RNA polymerases.Citation7 Ara-C is converted to its inactive metabolite Arauridine through cytidine deaminase (CDA) while Ara-CMP is converted to an inactive metabolite, Ara-UMP by deoxycytidine monophosphate deaminase (dCMPD).Citation8 Both in vitro and in vivo studies have shown that changes in the cellular levels of dCK, CDA and dCMPD are associated with changes in intracellular drug concentrations. Thus, the efficacy of a specific dose of Ara-C may also vary depending upon expression of these enzymes as they may alter the availability of drug at the target.Citation9–Citation12
Topoisomerases, such as topoisomerase IIα (Topo-IIa), are enzymes required for relieving DNA supercoils during replication, transcription and chromosome condensation.Citation13 Topo-IIa expression starts increasing during S phase of cell cycle and continues to increase in G2 and M phases, thus being highly expressed in rapidly dividing cells. Some anticancer drugs such as anthracyclines, etoposide and mitoxantrone act by targeting Topo-IIa and preventing it from religating nicks in DNA, thus introducing strand breaks.Citation14,Citation15 Topo-IIa expression has been found to correlate with clinical outcome in various malignancies, but the findings of various studies are contradictory, where high Topo-IIa expression is correlated with a favorable outcome in some studies,Citation16–Citation19 while having an adverse outcome in others.Citation20–Citation23 For example, in acute lymphoblastic leukemia (children n=65), an increased Topo-IIa expression correlated with daunorubicin resistance as part of the FRALLE-93 protocol.Citation20 Thus, it is imperative that the chemotherapy outcome should be studied in relation to molecular markers given above to draw a holistic picture. Hence, this study was designed to comprehensively analyze the role of hENT1, dCK, CDA, dCMPD and Topo-IIa gene expression in response to standard 3+7 AML chemotherapy regimen.
Materials and methods
Patient induction, sample collection and real-time/quantitative PCR
A total of 90 patients diagnosed with AML were recruited at National Institute of Blood Disease & Bone Marrow Transplantation (NIBD&BMT) Karachi, during September 2011 to March 2017. All patients, who received cytarabine 200 mg/m2/day for 7 days and daunorubicin 45 mg/m2/day for 3 days, were included. Complete remission (CR) was defined as blast cells <5% in bone marrow and no blast cells in peripheral blood. Patients remained under observation and were assessed for CR documentation during the days 21–28 after the first cycle of induction chemotherapy.
The study was approved by the Ethical Review Board at NIBD&BMT in accordance with the Declaration of Helsinki. All patients provided written informed consent to participate in this research. Any participant under the age of 18 had parental or legal guardian written informed consent confirmed.
Patient bone marrow and peripheral blood samples were collected separately and were used to study the expression of hENT1, dCK, CDA, dCMPD and Topo II. Detailed information about sample collection and storage, RNA extraction, reverse transcription reaction and quantitative real-time PCR (qPCR) were previously reported.Citation24 Briefly, we enriched the leukemia blasts with the Ficoll gradient method.Citation24 The peripheral blood mononuclear cells layer yielded cells overwhelmingly populated by blast cells. Other mononuclear cells could be seen only sporadically, as confirmed by morphology and flow cytometry. Primers and probes used are: for hENT1 forward 5′-TGTTTCCAGCCGTGACT-3′, reverse 5′-CAGGCCACATGAATACAG-3′ and probe 5′-/56-FAM/CA GCA CCT G/ZEN/G GAA CGTTAC TT/3IABkFQ/-3′; for dCK forward 5′-TGCAGGGAAGTCAACATT-3′, reverse 5′-TCCCAC-CATTTTTCTGAG-3′ and probe 5′-/56-FAM/TA AAC AAT T/ZEN/G TGT GAA GATTGG GAA G/3IABkFQ/-3′; for CDA forward 5′-GGAGGCCAAGAAGTCAG-3′, reverse 5′-GACGGCCTTCTGGATAG-3′ and probe 5′-/56-FAM/CA ACA TAG A/ZEN/A AAT GCC TGCTAC CC/3IABkFQ/-3′; for dCMPD forward 5′-AATGGGTGCAGTGATGAC-3′, reverse 5′-CTTAGCGCATTCATTACAAG-3′ and probe 5′-/56-FAM/AT CAT GAA C/ZEN/A AAA ATT CGACCG AT/3IABkFQ/-3′; for Topo-IIa forward 5′-AGTC-GCTTTCAGGGTTCTTGAG-3′, reverse 5′-TTTCATTTA-CAGGCTGCAATGG-3′ and probe 5′-/56-FAM/CC CTT CAC G/ZEN/A CCG TCA CCATGG A/3IABkFQ/-3′, and for GAPDH forward 5′-GAAGGTGAAGGTCGGAGTCA-3′, reverse 5′-GAAGATGGTGATGGGATTTC-3′, and probe 5′-(FAM)/56-JOEN/CC GAC TCT T/ZEN/G CCC TTCGAA C/3IABkFQ/(TAMRA)-3′.Citation25,Citation26
Statistical analyses
Statistical analyses were done using SPSS version 19.0 (IBM Corporation, Armonk, NY, USA). Data are presented as frequencies and percentages, or median and interquartile ranges where applicable. Chi-squared tests were used to analyze the differences between the groups. Spearman’s correlations (rs) were computed to determine the relationships between different gene expressions. The Kaplan–Meier survival analysis (log-rank test) was carried out to explore the survival according to gene expression. Only a P<0.05 was considered significant.
Results
Baseline characteristics
Ninety AML patients were analyzed in this study. Baseline data, such as age, gender and ethnic distribution, AML subtype, myeloperoxidase status, mutations, translocations and karyotyping are given in , which shows that CR was achieved by 56 patients while 34 were resistant to chemotherapy. A relapse was reported in 19 patients who had achieved CR. Thus, 37 patients who achieved remission and did not relapse during the study period (persistent remission) were labeled as good responders to therapy (41%), whereas all those patients who showed either little or no remission after chemotherapy or relapsed later were grouped together as poor responders (n=53; 59%). One-year disease-free survival (DFS) and overall survival (OS) status was calculated. Since gene expression data were not normally distributed, median and IQRs are provided according to various groups, as shown in .
Table 1 Baseline characteristics of the study population (n=90)
Chi-squared and Fisher exact tests
Grouping variables were dichotomized for meaningful analysis, ie, gender (male and female), AML classification (APML being good prognostic, all others being poor prognostic), myeloperoxidase status (negative, positive), remission status (relapse, persistent remission), final therapeutic response (poor, good) and survival status (dead, alive). Nonparametric variables were compared by chi-squared or Fisher’s exact test (). AML other than APML had a higher relapse rate (P=0.012), poor final therapeutic response (P<0.001) and a trend of higher mortality (P=0.05). In addition, patients with relapse and poor therapeutic outcome (resistant + relapsed) had higher mortality (P<0.001 for both groups). FLT3-positive patients had a poor therapeutic outcome when compared with FLT3-negative patients (P=0.03).
Table 2 Comparison between groups according to baseline characteristics
Since the gene expression data were not normally distributed, we stratified it as either low or high expression. If the relative gene expression was up to one-fold, the patients were labeled low expressers, and if more than one, high expressers. Chi-squared or Fisher’s exact test was done to compare low or high expression between relapse vs remission, poor vs good therapeutic response and dead vs alive (survival) groups (). Among good responders, a trend of high hENT1 expression (bone marrow, P=0.07; peripheral blood, P=0.05) but lower marrow dCMPD expression (P=0.043) was observed when compared with poor responders. Although bone marrow Topo-IIa showed a trend of being higher among good responders, it did not reach significance. However, such significance for Topo-IIa expression was achieved in peripheral blood samples of good responders (P=0.006). Subgroup analysis showed that peripheral blood Topo-IIa expression was higher in persistent remission vs relapse group (P=0.001).
Table 3 Comparison between groups according to gene expression
No significant difference was found in the gene expression of dCK and CDA among these clinical outcome groups.
OR was computed, which showed that patients with low Topo-IIa expression in peripheral blood relapsed more often (OR: 26.25) and had poorer therapeutic response (OR: 11.8) than those with higher expression. Patients with lower dCMPD expression in bone marrow were likely to have good response (OR: 3.1).
Nonparametric correlation – Spearman’s Rho (rs)
Correlation was computed among the expression of genes in bone marrow and peripheral blood (). A positive correlation was observed between the expression in bone marrow and peripheral blood for each gene. There was a positive correlation between dCK and dCMPD as well as hENT1 in respective bone marrow and peripheral blood samples. Both bone marrow and peripheral blood dCK expression positively correlated with dCK/CDA ratio in both bone marrow and peripheral blood. CDA expression positively correlated with hENT1 and Topo-IIa expression in respective sample types. dCMPD expression positively correlated with hENT1 and Topo-IIa expression in respective sample types. In addition, Topo-IIa correlated positively with dCK/CDA ratio.
Table 4 Spearman correlation matrix
OS
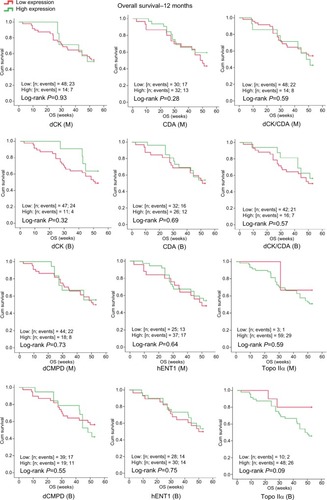
OS was calculated for 6 and 12 months by Kaplan–Meier analysis and is presented in . Better OS at 12 months was noted for APML (P=0.031), whereas poor OS at 6 and 12 months was seen in those with FLT3 mutation when compared with those without it (P=0.003 and P=0.001, respectively). A trend of higher Topo-IIa expression in peripheral blood with better DFS was observed (P=0.09). No significant differences were observed for higher and lower expression of other genes regarding 6- or 12-month OS.
Figure 1 Kaplan–Meier curves showing OS in relationship to dCK, CDA, dCK/CDA, dCMPD, hENT1 and Topo-IIα expression in bone marrow (M) and peripheral blood (B).
Abbreviations: CDA, cytidine deaminase; Cum, cumulative; dCK, deoxycytidine kinase; dCMPD, deoxycytidine monophosphate deaminase; hENT1, human equilibrative nucleoside transporter 1; OS, overall survival; Topo-IIα, topoisomerase IIα.
DFS
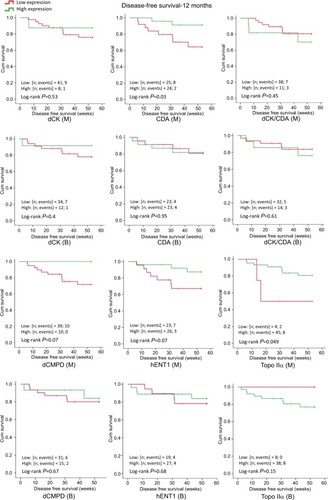
shows better 12-month DFS among high CDA expressors (P=0.032) in bone marrow. Better DFS was found with high bone marrow Topo-IIa expression at both 6 (0.04) and 12 months (P=0.04). A trend of high Topo-IIa expression in peripheral blood with better DFS was also observed (P=0.08).
Figure 2 Kaplan–Meier curves showing DFS in relationship to dCK, CDA, dCK/CDA, dCMPD, hENT1 and Topo-IIα expression in bone marrow (M) and peripheral blood (B).
Abbreviations: CDA, cytidine deaminase; Cum, cumulative; dCK, deoxycytidine kinase; dCMPD, deoxycytidine monophosphate deaminase; DFS, disease free survival; hENT1, human equilibrative nucleoside transporter 1; Topo-IIα, topoisomerase IIα.
Discussion
We observed that high Topo-IIa expression is strongly associated with a better CR rate in AML patients treated with standard dose 3+7 induction chemotherapy comprising Ara-C and daunorubicin, and thus translates into low relapse and better DFS, whereas high dCPMD expression was associated with poor chemotherapy response. In agreement with other studies, we observed that patients with APML and absent FLT3 mutation had better therapeutic response and survival.
Although WHO and European Leukemia Net classifications have included many factors determining the clinical outcome in terms of response and survival, the picture is far from complete. Remission rates remain poor and many patients do not survive, pointing to the possibility of incompletely treated disease with chemotherapy. Multiple mechanisms can potentially be attributed to a partial or absent response to chemotherapy. These may include alterations in influx and efflux of the chemotherapeutic drugs, activation and inactivation of the drugs, drug target availability and ultimately the efficiency of apoptotic machinery. These factors are not yet part of any AML therapeutic guideline partly due to conflicting data. The current study is an attempt to clarify the role of these mechanisms in association with therapeutic outcome in AML patients treated with Ara-C and daunorubicin.
Expression of Ara-C transporter hENT1 and metabolizing enzymes dCK, CDA and dCMPD
Ara-C is transported inside the cell by hENT1Citation5 and increased retention of Ara-C in leukemic cells has been associated with longer duration of CR in patients with AML.Citation27 Low and high expression of hENT1 have been reported as a predictor of Ara-C resistance in AMLCitation10,Citation28 and sensitivity in acute lymphocytic leukemia,Citation9 respectively. Some solid organ tumors have shown interesting results. For example, some degree of hENT1 protein expression has been found associated with increased OS and DFS in pancreatic cancer treated with gemcitabine (a pyrimidine nucleoside analog) when compared with no hENT1 expression.Citation29–Citation31 It has also been shown in vitro that hENT1 expression positively correlated with IC50 of gemcitabine, suggesting a direct role of hENT1 expression in cancer cell sensitivity in a non-small-cell lung cancer cell line exposed to gemcitabine.Citation32 Greenhalf et alCitation31 inferred that pancreatic cancer patients with no hENT1 expression should not be treated with gemcitabine. Similarly, higher expression of hENT1 has been found associated with prolonged survival or better therapeutic response in patients with advanced biliary tract cancer who were treated with gemcitabine.Citation33
In a recent study of hematological malignancy, high-risk Myelodysplastic syndrome patients treated with decitabine (another pyrimidine analog) also suggested a similar outcome.Citation34 We observed that in AML patients treated with the standard 3+7 regimen, a trend of higher hENT1 expression was seen among good responders, although it did not reach statistical significance (bone marrow, P=0.07; peripheral blood, P=0.05). This inability to reach statistical significance could be partly explained based on sample size, because another study with a higher sample size reported a shorter DFS among hENT1-deficient AML patients (n=123) treated with Ara-C dosage similar to our study.Citation28
Once Ara-C is inside the cells, dCK, a cytoplasmic enzyme, activates Ara-C by phosphorylating it, which is then incorporated in the newly synthesized DNA, while CDA inactivates it. Abraham et alCitation35 have described Ara-C resistance index, which is denoted as ΔCt (DCK × ENT1)/ΔCt CDA. They found that resistance index values were significantly higher in resistant patients compared with sensitive patients. In contrast, we have observed that dCK and CDA expression was not associated with response to chemotherapy; however, we had a smaller sample size but more rigorous method of gene expression calculation (ΔΔCt), which might explain the difference. Regarding the inactivators of Ara-C, we have shown that expression of bone marrow dCMPD was significantly higher in poor therapeutic response, with OR=3 (). Paradoxically, a higher CDA expression in bone marrow (instead of anticipated lower expression) was found significantly associated with better DFS. At present, the significance of this isolated finding is unclear. This could be a chance finding because no other subgroup analysis could support this observation. Hence, it needs to be explored further.
In contrast, Achiwa et alCitation32 did not find any correlation of dCK expression with IC50 of gemcitabine in a non-small-cell lung cancer line. Similarly, many studies have shown no significant association of the gene expression of dCK, CDA and hENT1 with clinical outcome or survival in AML (n=123 and 42)Citation28,Citation36 as well as a variety of other cancers such as myelodysplastic syndrome (n=98)Citation34 and biliary tract cancer (n=28).Citation33 Our study shows a similar trend of dCK or CDA expression with regard to patient survival or chemotherapy outcome.
We observed that bone marrow and peripheral blood hENT1 expression correlated with each other and with dCK, CDA, dCMPD and Topo-IIa positively in respective bone marrow and peripheral blood samples (). These observations might indicate a synchronized regulation of expression of these genes suggesting differential transcriptomic regulation.
Role of anthracycline target Topo-IIa
The expression of Top IIα, being a target molecule for anthracyclines, seems imperative in assessing the response to anthracycline-based chemotherapy. In our study, AML patients were treated with daunorubicin 45 mg/day as part of the standard regimen described above. We observed that higher peripheral blood Topo-IIa expression was associated with persistent remission as compared with resistance (P=0.047) or relapse (P<0.001) (Mann–Whitney U-test, data not provided). In addition, patients with higher peripheral blood Topo-IIa expression had significantly better DFS at 6 and 12 months. There was no effect of Topo-IIa expression on OS. Patients with low Topo-IIa expression in peripheral blood had higher odds to develop relapse (OR >26) and poor therapeutic response (OR >11). Thus, availability of Topo-IIa is important for a better therapeutic response. Topo-IIa expression in peripheral blood was found positively and strongly correlated with hENT1 expression. This correlation may be explained by a possible upregulation of Topo-IIa in response to the drug entering the cell, although the transporter for daunorubicin entry is not well characterized. Some studies have shown, in agreement with our findings that higher Topo-IIa expression could predict better outcome in breast cancer patients treated with anthracyclines. In one study, patients were treated with five cycles of 5-flurouracil, epirubicin, cyclophosphamide, which included an anthracycline called epirubicin 75–100 mg/m2.Citation18 In another study, it was reported that Topo-IIa expression in Her2/neu expressing breast cancer positively influenced response to anthracycline-based chemotherapy.Citation17 A systematic review of breast cancer patients receiving anthracycline-based chemotherapy has also supported this observation.Citation16 As described earlier, Topo-IIa expression increases during S, G2 and M phases of the cell cycle, and is thus highly expressed in rapidly dividing cells.Citation14,Citation15 Chemotherapy may kill the cancer cells and lead to senescence of normal tissue.Citation37 Thus, it can be hypothesized that if Topo-IIa is highly expressed it may not only provide a better drug target in malignant cells but also help in subsequent DNA repair in normal tissue damaged by chemotherapy.
However, high expression may be a double-edged sword, as it may dilute the therapeutic effect of anthracyclines by providing abundant topoisomerase function to evade the drug action. Currently, little is known about this intricate balance and much seems to depend on pathology, tissue involved and anthracycline dosing, among other factors. For example, in contrast to our results, in small cell lung cancer patients (n=93) receiving doxorubicin and etoposide, high Topo-IIa expression was associated with poor therapeutic outcome and low OS.Citation21 Similarly, another study conducted on Hodgkin’s lymphoma patients receiving anthracycline (doxorubicin or epirubicin; n=238) reported that high expression of Topo-IIa was associated with adverse prognosis, whereas low expression had no effect.Citation38 In patients with colorectal carcinoma (n=228), Topo-IIa overexpression was found associated with advanced tumor stage and resistant disease.Citation23
However, some studies could not find any significant association of Topo-IIa expression with outcome or survival among AML (n=123, semiquantitative RT-PCR)Citation28 and breast cancer (n=232) treated with anthracyclines.Citation39
Similarly, in some studies of AML, Topo-IIa expression was not found associated with clinical outcome at all.Citation28,Citation40 Conflicting results may be due to the use of techniques with different sensitivities. Immunohistochemistry was the technique used in most of these studies to assess Topo-IIa expression, but more sensitive techniques are now available.
The prognostic role of MPO has remained controversial.Citation41 There could be multiple reasons for that. For example, it is important to only consider studies with similar criteria for MPO positivity while exploring its role related to therapeutic outcome. An interesting observation of our study was the association of MPO positivity with poor therapeutic response.
Others have reported that MPO positivity is a favorable prognostic factor, though the effect size is small.Citation41 A recent study suggests that MPO status may, in fact, be a reflection of DNA methylation status in blast cells, and thus could be an indirect marker that should be interpreted with caution.Citation42 Thus, the MPO controversy needs further exploration in depth.
The main strength of our study included adoption of a uniform treatment and follow-up protocol as well as inclusion of both bone marrow and peripheral blood. Our study also had limitations. It was a single-center study and may not be representative of the entire population of AML patients. We recommend that this study should be replicated with a larger sample size and inclusion of other hematological malignancies to validate our results regarding gene expression.
Conclusion
AML patients with APML subtype had better CR rate and better OS. FLT3 mutation is a known bad prognostic marker. All patients positive for this mutation could not achieve CR and all were resistant to chemotherapy. A higher hENT1 expression tended to be associated with better CR rate in these patients. However, this observation may be confirmed by use of a larger sample size. CDA and dCK expression did not correlate with CR rate. Higher dCPMD expression was associated with poor chemotherapy response. A high Topo-IIa expression is strongly associated with better CR rate in AML patients treated with standard dose 3+7 induction chemotherapy comprising Ara-C and daunorubicin, and thus translates into low relapse and better DFS.
Acknowledgments
The authors acknowledge Alfaisal University, Riyadh, Saudi Arabia, for the financial support through grant IRG-302111603131 for partial support of this project. They also thank Dr Peter M. B. Cahusac, Associate Professor of Pharmacology and Biostatistics, Alfaisal University, for his kind support in reviewing the article for English language.
Supplementary material
Table S1 Gene expression profile, grouped by various factors
Author contributions
All authors met authorship criteria and made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- DöhnerHEsteyEHAmadoriSDiagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNetBlood2010115345347419880497
- LerchEEspeliVZuccaEPrognosis of acute myeloid leukemia in the general population: data from southern SwitzerlandTumori200995330331019688968
- BahlASharmaARainaVLong-term outcomes for patients with acute myeloid leukemia: a single-center experience from AIIMS, IndiaAsia Pac J Clin Oncol201511324225225639656
- ShtilAASignal transduction pathways and transcriptional mechanisms as targets for prevention of emergence of multidrug resistance in human cancer cellsCurr Drug Targets200121577711465539
- ZhangJVisserFKingKMBaldwinSAYoungJDCassCEThe role of nucleoside transporters in cancer chemotherapy with nucleoside drugsCancer Metastasis Rev20072618511017345146
- MataJFScrideliCAQueirozRPCytosine arabinoside-metabolizing enzyme genes are underexpressed in children with MLL gene-rearranged acute lymphoblastic leukemiaBraz J Med Biol Res200639111417142317146554
- HazraSOrtSKonradMLavieAStructural and kinetic characterization of human deoxycytidine kinase variants able to phosphorylate 5-substituted deoxycytidine and thymidine analoguesBiochemistry201049316784679020614893
- ChabnerBAAmreinPCDrukerBJAntineoplastic Agents Texbook of Goodman & Gilman’s The Pharmacological Basis of Therapeutics11th edBruntonLLLazoJSParkerKLNew YorkThe McGraw-Hill Companies Inc200613151403
- StamRWden BoerMLMeijerinkJPDifferential mRNA expression of Ara-C-metabolizing enzymes explains Ara-C sensitivity in MLL gene-rearranged infant acute lymphoblastic leukemiaBlood200310141270127612406912
- KannoSHiuraTOhtakeTCharacterization of resistance to cytosine arabinoside (Ara-C) in NALM-6 human B leukemia cellsClin Chim Acta20073771–214414917097625
- LambaJKCrewsKPoundsSPharmacogenetics of deoxycytidine kinase: identification and characterization of novel genetic variantsJ Pharmacol Exp Ther2007323393594517855478
- RatheSKLargaespadaDADeoxycytidine kinase is downregulated in Ara-C-resistant acute myeloid leukemia murine cell linesLeukemia20102481513151520508618
- PommierYLeoEZhangHMarchandCDNA topoisomerases and their poisoning by anticancer and antibacterial drugsChem Biol201017542143320534341
- PogorelčnikBPerdihASolmajerTRecent developments of DNA poisons–human DNA topoisomerase IIα inhibitors–as anticancer agentsCurr Pharm Des201319132474248823363399
- BowerJJKaracaGFZhouYSimpsonDACordeiro-StoneMKaufmannWKTopoisomerase II alpha maintains genomic stability through decatenation G(2) checkpoint signalingOncogene201029344787479920562910
- MiyoshiYKurosumiMKurebayashiJPredictive factors for anthracycline-based chemotherapy for human breast cancerBreast Cancer201017210310919657712
- WangJXuBYuanPTOP2A amplification in breast cancer is a predictive marker of anthracycline-based neoadjuvant chemotherapy efficacyBreast Cancer Res Treat2012135253153722864769
- MukherjeeAShehataMMoseleyPRakhaEEllisIChanSTopo2α protein expression predicts response to anthracycline combination neo-adjuvant chemotherapy in locally advanced primary breast cancerBr J Cancer2010103121794180021063406
- NikolényiASükösdFKaizerLTumor topoisomerase II alpha status and response to anthracycline-based neoadjuvant chemotherapy in breast cancerOncology2011803–426927721734419
- GrandgirardNLy-SunnaramBFerrantDImpact of Topoisomerase II alpha and spermine on the clinical outcome of children with acute lymphoblastic leukemiaLeuk Res200428547948615068901
- DingemansAMWitloxMAStallaertRAvan der ValkPPostmusPEGiacconeGExpression of DNA topoisomerase II alpha and topoisomerase IIbeta genes predicts survival and response to chemotherapy in patients with small cell lung cancerClin Cancer Res1999582048205810473085
- MaternaVPlegerJHoffmannULageHRNA expression of MDR1/P-glycoprotein, DNA-topoisomerase I, and MRP2 in ovarian carcinoma patients: correlation with chemotherapeutic responseGynecol Oncol200494115216015262134
- CosseJPMichielsCTumour hypoxia affects the responsiveness of cancer cells to chemotherapy and promotes cancer progressionAnticancer Agents Med Chem20088779079718855580
- KulsoomBShamsiTSAfsarNAMemonZAhmedNHasnainSNBax, Bcl-2, and Bax/Bcl-2 as prognostic markers in acute myeloid leukemia: are we ready for Bcl-2-directed therapy?Cancer Manag Res20181040341629535553
- BurgerHFoekensJALookMPRNA expression of breast cancer resistance protein, lung resistance-related protein, multidrug resistance-associated proteins 1 and 2, and multidrug resistance gene 1 in breast cancer: correlation with chemotherapeutic responseClin Cancer Res20039282783612576456
- SuzukiKKazuiTYoshidaMDrug-induced apoptosis and p53, BCL-2 and BAX expression in breast cancer tissues in vivo and in fibroblast cells in vitroJpn J Clin Oncol199929732333110470656
- RustumYMPreislerHDCorrelation between leukemic cell retention of 1-beta-D-arabinofuranosylcytosine 5′-triphosphate and response to therapyCancer Res19793914249282940
- GalmariniCMThomasXCalvoFIn vivo mechanisms of resistance to cytarabine in acute myeloid leukaemiaBr J Haematol2002117486086812060121
- SpratlinJSanghaRGlubrechtDThe absence of human equilibrative nucleoside transporter 1 is associated with reduced survival in patients with gemcitabine-treated pancreas adenocarcinomaClin Cancer Res200410206956696115501974
- FarrellJJElsalehHGarciaMHuman equilibrative nucleoside transporter 1 levels predict response to gemcitabine in patients with pancreatic cancerGastroenterology2009136118719518992248
- GreenhalfWGhanehPNeoptolemosJPPancreatic cancer hENT1 expression and survival from gemcitabine in patients from the ESPAC-3 trialJ Natl Cancer Inst20141061djt34724301456
- AchiwaHOguriTSatoSMaedaHNiimiTUedaRDeterminants of sensitivity and resistance to gemcitabine: the roles of human equilibrative nucleoside transporter 1 and deoxycytidine kinase in non-small cell lung cancerCancer Sci200495975375715471562
- MurataAAmanoRYamadaNPrognostic predictive values of gemcitabine sensitivity-related gene products for unresectable or recurrent biliary tract cancer treated with gemcitabine aloneWorld J Surg Oncol20131111723710668
- WuLShiWLiXHigh expression of the human equilibrative nucleoside transporter 1 gene predicts a good response to decitabine in patients with myelodysplastic syndromeJ Transl Med201614667426944860
- AbrahamAVaratharajanSKarathedathSRNA expression of genes involved in cytarabine metabolism and transport predicts cytarabine response in acute myeloid leukemiaPharmacogenomics201516887789026083014
- VeugerMJHondersMWWillemzeRBargeRMDeoxycytidine kinase expression and activity in patients with resistant versus sensitive acute myeloid leukemiaEur J Haematol200269317117812406011
- JordanCTGuzmanMLNobleMCancer stem cellsN Engl J Med20062135512531261
- Doussis-AnagnostopoulouIAVassilakopoulosTPThymaraITopoisomerase II alpha expression as an independent prognostic factor in Hodgkin’s lymphomaClin Cancer Res20081461759176618347177
- ArriolaEMorenoAVarelaMPredictive value of HER-2 and Topoisomerase II alpha in response to primary doxorubicin in breast cancerEur J Cancer200642172954296016935488
- GieselerFGlasmacherAKämpfeDTopoisomerase II activities in AML blasts and their correlation with cellular sensitivity to anthracyclines and epipodophyllotoxinesLeukemia199610Suppl 3S46S49
- KimYYoonSKimSJKimJSCheongJWMinYHMyeloperoxidase expression in acute myeloid leukemia helps identifying patients to benefit from transplantYonsei Med J201253353053622476996
- ItonagaHImanishiDWongYFExpression of myeloperoxidase in acute myeloid leukemia blasts mirrors the distinct DNA methylation pattern involving the downregulation of DNA methyltransferase DNMT3BLeukemia20142871459146624457336