
Abstract
Background
Sorafenib is the first regimen listed in the treatment algorithm for hepatocellular carcinoma (HCC) worldwide. This study aimed to assess the efficacy of sorafenib treatment for advanced HCC in a clinical practice using a nationwide population study.
Methods
All patients registered with a diagnosis of primary HCC and identified as having been prescribed sorafenib between August 2012 and December 2015 were selected from a national database and retrospectively reviewed. Outcomes related to prescription of sorafenib for these patients were further assessed.
Results
A total of 9,738 patients were enrolled and analyzed. As a result, 32.33% of patients had an initial treatment response and were eligible for the prescribed second term (240 tablets/ term) of sorafenib and 8.91% of patients received more than three terms of sorafenib. Meanwhile, the duration of sorafenib usage beyond 6 months was noted in 15.49% of patients, including 10.59% of patients with a period of usage between 6 and 12 months and 4.9% of patients with more than 12 months usage. Survival analysis showed that patients who received locoregional therapy plus sorafenib had significantly better survival rates than those who underwent only sorafenib treatment. Certain patients who underwent hepatectomy (n=12) or liver transplantation (n=13) were subsequently free of HCC.
Conclusion
The disease control rate of sorafenib in advanced HCC patients in this study seemed similarly poorer as what has been previously reported by clinical trials. The combination of sorafenib and additional treatments could perhaps provide survival benefits and possibly cure disease in combination with surgical management.
Introduction
Despite ongoing developments in diagnostic techniques and therapeutic strategies, the overall prognosis for patients with hepatocellular carcinoma (HCC) remains dismal. The major concern regarding poor outcomes is attributed to late detection leading to patients becoming ineligible for potentially curative treatments, as more than approximately two-thirds of patients are diagnosed in the advanced stages of HCC.Citation1 In fact, no systemic therapy has been shown to confer a survival advantage in patients with advanced HCC prior to the availability of sorafenib.Citation2,Citation3 Using the well-known sorafenib Hepatocellular Carcinoma Assessment Randomized Protocol (SHARP) study, sorafenib was first shown to be an efficacious therapeutic option and well tolerated in patients with advanced HCC.Citation4
Sorafenib is a multikinase inhibitor with both antiproliferative and antiangiogenic effects and has been shown to induce apoptosis in a wide range of tumor models.Citation5,Citation6 Moreover, the molecular pathogenesis of HCC with regard to Raf-1 and vascular endothelial growth factor signaling pathways could be inhibited by sorafenib, which provides the rationale for indication in this setting.Citation7–Citation9 Subsequently, Cheng et al conducted a further study that showed a similar result showing sorafenib to be an appropriate option for the treatment of advanced HCC in the Asia-Pacific region.Citation10 As a result, sorafenib was approved for the treatment of unresectable HCC worldwide and listed in the Barcelona Clinic Liver Cancer (BCLC) staging system and the Asian Pacific Association for the Study of the Liver (APASL) as the treatment guideline for HCC.Citation11–Citation13
To further understand the adoption of sorafenib and associated survival rates of individuals with advanced HCC in clinical practices, this study conducted a nationwide population-based evaluation over time, examining this newly approved drug in HCC. The study is characterized by a Taiwan National Health Insurance (NHI) program that covers nearly the entire national population and reimburses the cost of sorafenib to indicated-patients with advanced HCC. This NHI program consists of detailed healthcare information related to claims data and is believed to be the most comprehensive and reliable database for assessing the real practice in terms of treatment outcomes of sorafenib in patients with advanced HCC.
Materials and methods
Sorafenib prescription
The Taiwan NHI program covers nearly the entire population of the country, and the database consists of comprehensive information related to healthcare data. Sorafenib has been both fully covered and reimbursed by NHI since August 2012 for patients under certain indications that are generally based on the treatment algorithm for HCC proposed by APASL and BCLC. Therefore, patients with BCLC advanced stage HCC including macroscopic vascular invasion and/or extrahepatic metastasis that were not amenable to either surgical resection or locoregional therapy were eligible for sorafenib prescription. In addition, patients were also required to have a liver functional reserve of Child–Pugh class A. Physicians apply to the NHI for all patients who met the aforementioned conditions and NHI reviews patients’ clinical data and approves the use of sorafenib. The NHI is allowed to prescribe 800 mg (200 mg/tablet) of a defined daily dose (DDD) for 2 months in every qualifying patient. The application has to be renewed every 2 months or run out of sorafenib, in which patients who had imaging evidence showing no disease progression were eligible for another term of sorafenib usage.
Patient population
All patients registered with primary HCC in the Registry for Catastrophic Illness Patient Database who were identified as having been prescribed sorafenib from the NHI claim database since August 2012 were enrolled in the study. This study was thoroughly reviewed and endorsed by the internal review board of Chang Gung Memorial Hospital at Linkou (approved no. 201800970B0) and informed consent from patients was waived. In addition, the study complied with the ethical standards of the Declaration of Helsinki in terms of data linkage studies. All personal identification information on files was replaced by surrogate identification numbers to ensure patient privacy.
Statistical analyses
Outcome measures included time to discontinuation of sorafenib (TDS) and overall survival (OS). TDS was defined as the time between the date of the first sorafenib prescription and the date of last sorafenib prescription. OS was measured from the date of the first sorafenib prescription to the date of death or the end of this study. Statistical analyses were performed using SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA). Student’s t-test was used for continuous data, and categorical variables were compared using the chi-squared or Fisher’s exact tests, as appropriate. Survival curves in terms of TDS and OS were delineated using the Kaplan–Meier method and analyzed by means of the log-rank test. All statistical tests were two-sided, and a P-value of ≤0.05 was considered statistical significance.
Results
Patient characteristics
Overall, a total of 9,738 patients (7,664 men and 2,074 women) who were registered in the NHI database having been prescribed sorafenib for HCC between August 2012 and December 2015 were retrospectively analyzed. The baseline patient demographics are summarized in . More than half of the patients (57.35%) were registered as carrying chronic hepatitis B virus and 35.57% of patients were positive for hepatitis C virus. Apart from the year of 2012, more than 2,500 patients ranged from 2,592 to 2,754 HCC patients were treated with sorafenib each year.
Table 1 Clinical characteristics of patients with hepatocellular carcinoma treated with sorafenib
Prescription of sorafenib
Only 34.89% of patients were administered sorafenib within 3 months of HCC diagnosis, and sorafenib was administered more than 1 year after HCC was detected in the majority of patients (46.81%). Overall, 67.67% of patients were given no more than 2 months of DDD (240 tablets), which represented ~32.33% of patients that had an initial treatment response and/or good tolerance and were eligible for prescribed second term of sorafenib. Eventually, 8.91% of patients received more than three terms of sorafenib applications (≥720 tablets). With regard to the duration of treatment, most patients (46.77%) had no more than 2 months of sorafenib usage. Meanwhile, duration of treatment beyond 6 months was noted in 15.49% of patients, including 10.59% of patients who had a period of between 6 and 12 months and 4.9% of patients who had more than 12 months treatment ().
Additional therapy after sorafenib treatment
Apart from sorafenib, 4,200 patients (43.13%) received additional therapy including 22.02% of patients who received transarterial chemoembolization (TACE), 3.66% of patients who received radiofrequency ablation (RFA), and 29.34% of patients who received external beam radiotherapy. The median period between starting sorafenib and additional locoregional therapy were 5.5 months (25–75 percentile, 2.2–10.2), 7.4 months (3.0–15.3), and 1.4 months (0.5–4.7) for TACE, RFA, and radiotherapy, respectively. Eventually, 90 patients (0.92%) underwent hepatectomy, and 18 patients (0.18%) underwent liver transplantation following sorafenib treatment. The median period between starting sorafenib and surgical intervention was 4.6 months (25–75 percentile, 2.2–8.3) for hepatectomy and 5.5 months (1.6–8.0) for liver transplantation. Overall, 72.58% of patients died, 14.14% were alive with sorafenib usage and 13.28% were alive without sorafenib prescription at the end of the study period. Of those patients without ongoing sorafenib prescription, 541 patients (5.6%) remained under the combination of locoregional therapies and the remaining patients had no reimbursed record of therapy at least in the NHI database.
summarizes patients who had undergone surgical managements including hepatectomy (n=90) and liver transplantation (n=18) following sorafenib treatment. The majority of patients had received locoregional therapy in addition to sorafenib therapy prior to surgical treatments, and more than 80% of patients had total dosage of sorafenib prescription less than 720 tablets.
Table 2 Clinical characteristics of patients who had undergone surgical managements after sorafenib treatment
Outcomes and survival analysis
During the follow-up period, the median TDS of entire cohort was 2.5 months (range from 0.2 to 40.7 months).
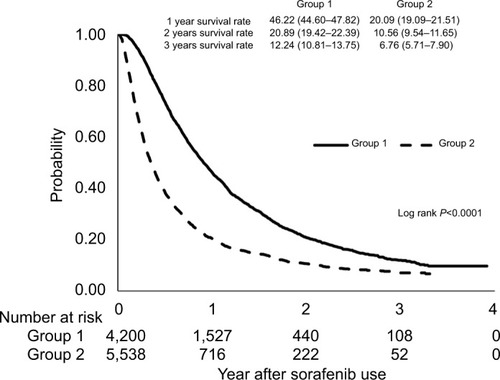
The analysis of sorafenib prescription in terms of the TDS curve showed that only 5% were still on sorafenib at 3 years (). The median time of OS was 5.4 months (range from 1.0 to 46.8 months). The OS of the entire cohort at 1-year and 3-year time points were 32.08% (95% CI =31.06–33.10) and 9.14% (95% CI =8.28–10.06), respectively (). Meanwhile, the OS of patients who had received additional locoregional therapy were significantly better than those of patients who had only given sorafenib treatment. The 1 and 3 years OS were 46.22% (95% CI =44.60–47.82) and 12.24% (95% CI =10.81–13.75) in patients with additional locoregional therapy compared with 20.29% (95% CI =19.09–21.51) and 6.76% (95% CI =5.71–7.90) of 1 and 3 years OS among patients treated with sorafenib only (, P<0.0001).
Figure 1 Kaplan–Meier plots of time to discontinuation of sorafenib for all patients.
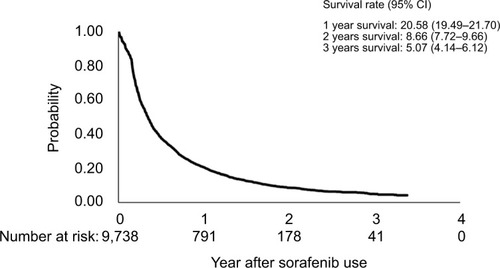
Figure 2 Kaplan–Meier plots of overall survival for all patients.
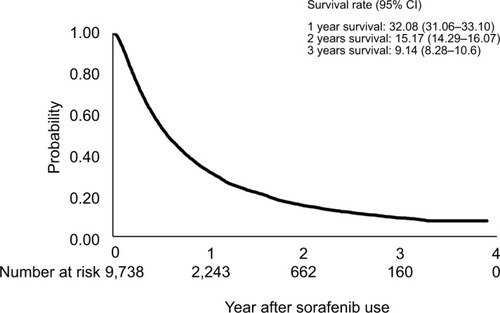
Figure 3 Comparison of Kaplan–Meier cumulative overall survival curves based on additional locoregional therapy. Group 1, patients had received sorafenib and additional locoregional therapy. Group 2, patients had only sorafenib treatment (P<0.0001).
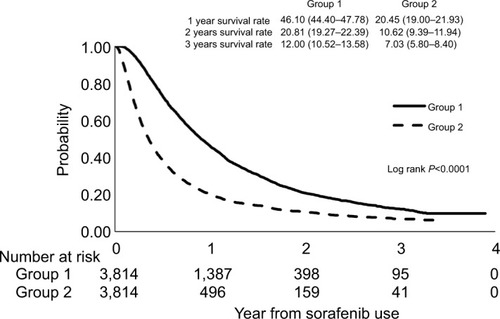
Moreover, a propensity score matching model was used for comparison between the two groups. Variables including age, sex, and comorbidities were matched on the basis of propensity score model, and patients selected from the two groups were further compared for outcome analysis. The outcome of patients who had received additional locoregional therapy were also significantly better than those of patients who had only given sorafenib treatment. The 1 and 3 years OS in the group of patients with additional locoregional therapy was 46.10% (95% CI =44.40–47.78) and 12.00% (95% CI =10.52–13.58), respectively, which was significantly better than that in the group of patients treated with sorafenib only, with 20.45% (95% CI =19.00–21.93) and 7.03% (95% CI =5.80–8.40), respectively (, P<0.0001). Of those patients who underwent hepatectomy following sorafenib treatment, 12 patients (13.33%) were alive with no evidence of HCC recurrence. In addition, 13 patients (72.22%) who had liver transplantation following sorafenib treatment were alive with no evidence of HCC recurrence by the date of the last follow-up in this study.
Figure 4 Kaplan–Meier survival curves in patients based on additional locoregional therapy after propensity score matching. The outcomes of patients who had received additional locoregional therapy were also significantly better than those of patients who had only given sorafenib treatment. Group 1, patients had received sorafenib and additional locoregional therapy. Group 2, patients had only sorafenib treatment (P<0.0001).
Discussion
As in the well-known studies on the effectiveness of sorafenib for patients with advanced HCC by Llovet et al and Cheng et al,Citation4,Citation10 sorafenib is initially the only regimen listed in the treatment algorithm of HCC worldwide including BCLC and APASL as the standard of care.Citation13,Citation14 Along with the advancement of oncology, numerous molecular targeted agents including regorafenib, lenvatinib, cabozantinib, ramucirumab, and immunotherapy of nivolumab are getting more attention to be an effective regiment for advanced HCC nowadays. To the best of our knowledge, this is one of the largest cohort studies in a single country, performed to evaluate the effectiveness of sorafenib treatment for advanced HCC in clinical practice. This study found that a limited number of patients with advanced HCC had initial therapeutic response of sorafenib treatment and only 8.9%–15.49% were able to stay on the treatment for more than 6 months of DDD or therapeutic duration. Importantly, a combination of multimodality treatments consisting of sorafenib plus locoregional therapy, followed by surgical managements, could provide favorable benefits for specific groups of patients with advanced HCC.
Although the multikinase inhibitor is able to inhibit the growth of tumor cells in a wide range of malignancies, sorafenib could also affect the physiological function of normal cells leading to numerous drug-related side effects. As such, the most common side effects of sorafenib included hand-foot skin reaction, diarrhea, and fatigue. These side effects may lead to a reduction in dose or interruption of treatment in the clinical scenario. As shown in this study, 67.67% of patients were prescribed no more than 240 tablets of sorafenib in total, but only 46.77% of patients with less than 2 months in duration of treatment received this number of tablets. This discrepancy represented ~20% of patients who had a dose reduction instead of the standard sorafenib dosage (800 mg/day). However, the NHI registration database was not able to identify the cause of dose reduction in these patients. It is possible that some physicians may prefer therapeutic strategy that prescribes sorafenib at a lower initial dosage and with a subsequent increase in dosage according to the patient’s ability to tolerate sorafenib.Citation15–Citation17 Equally, certain patients could have undergone a dose reduction due to side effects as shown in the Asia-Pacific study.Citation10
However, it remains debatable whether the full initial dose implies a better sorafenib efficacy and some studies reported that a lower starting dosage might result in similar outcomes.Citation16,Citation17 Importantly, a lower starting dosage could also enhance patients’ compliance, taking into consideration performance status and comorbidities of patients. In addition, the application of sorafenib has to be reviewed and approved by external experts in every term, based on the imaging evidence of therapeutic efficacy in the NHI program. Patients who had stable disease or regression were eligible for another term of sorafenib usage. Therefore, the overall therapeutic response of sorafenib for patients with advanced HCC may be better reflected by the treatment duration instead of total dosage in this study.
Meanwhile, 15.49% patients in this study that had sorafenib for at least 6 months may be interpreted as experiencing a short-term therapeutic response. With regard to the long-term therapeutic response, the percentage decreased to only 4.9% of patients with sorafenib treatment lasting longer than 12 months. Accordingly, the ratio of therapeutic response in terms of disease control by this analysis was lower than that in the initial SHARP and Asia-Pacific studies. These differences could be associated with some unobtainable factors from this NHI database that related to both the sorafenib dose and prognosis, such as performance status of patients and the tumor characteristics of HCC.
In line with previous studies, patients treated using a combination of treatments had a better outcome compared with patients treated with only sorafenib in this study. Although the therapeutic effects were not truly related to sorafenib, additional locoregional therapy and radiotherapy would provide benefit to these patients. Locoregional therapy not only induces tumor necrosis and diminished tumor burden but also possibly lessens several risk factors.Citation18 Meanwhile, locoregional therapy may also mitigate tumor progression in certain circumstances, and a combination of radiotherapy targeting portal vein tumor thrombosis and locoregional therapy for intrahepatic HCC could be a promising strategy for patients with advanced stage HCC.Citation19,Citation20 However, numerous well-known prospective randomized trials had failed to show survival benefit in terms of combination of TACE and sorafenib for patients with unresectable HCC.Citation21–Citation23 Whereas, most of the evidence based on retrospective studies had shown that the combination of locoregional therapy and sorafenib is well tolerated and efficacious for patients with advanced HCC.Citation24–Citation26 Nowadays, the concept of managing advanced HCC has evolved multimodality treatments, thus sorafenib is rarely applied as the sole treatment for HCC in clinical practice nowadays. As shown in this study, nearly half of the patients received sorafenib concurrently with other treatments including locoregional therapy and radiotherapy.
Indeed, patients who had additional locoregional therapy might be doubted naturally in a better clinical condition than patients not receiving locoregional therapy. Despite a propensity score matching analysis, numerous unobtainable factors from this database might also affect decision-making in therapeutic strategy for patients. As such, the limitation of the study design was not able to clarify the difference. Although the best therapeutic approach for advanced HCC remains uncertain, the accumulated evidence and this study have shown that an aggressive attitude using multidisciplinary treatment simultaneously could effectively provide benefits to patients. Nonetheless, combination treatments such as those frequently seen in this database are not endorsed by current guidelines of HCC treatment.
In addition, few patients had the chance to undergo surgical resection including hepatectomy and liver transplantation following sorafenib treatment. Despite having few number, patients who had their HCC well controlled and/or experienced a regression change after treatment may have opportunity to receive surgical management. Currently, curative resection by surgical management remains the gold standard treatment for HCC, as well as providing best survival benefit and curing selected patients.Citation27–Citation29 Hence, the best scenario for patients would be turning an unresectable HCC into one eligible for surgical resection, including hepatectomy and liver transplantation. As this study showed, patients who eventually underwent hepatectomy and liver transplantation enjoyed a better outcome compared with other patients. Moreover, a certain population of patients was initially diagnosed with advanced HCC and subsequently free of HCC following these treatments.
However, there were a few concerns and limitations in this retrospective study. First, the database does not contain laboratory tests and imaging examination results; therefore, numerous elements including liver function tests, AFP, well-established prognostic factors of HCC, performance status of patients, and sorafenib-related adverse events were not explicitly taken into consideration in the data analysis. Accordingly, the reasons for terminating sorafenib prescription for patients could not be assessed. Second, drug exposure in terms of nonadherence when patients failed to comply and take the prescribed sorafenib likely leads to a misestimate of the therapeutic response. Apart from that, possible errors in the coding of registration data could occur, and the study thus cannot evaluate exactly the population included and determine the determinants of treatment choice. Therefore, the study cannot conclude about the true effect of sorafenib and the true effect of combination treatment. Nonetheless, the strength of the present study is the large sample size, covering a nationwide database, in which the results are likely to illustrate marked information in the therapeutic strategy for patients with advanced HCC as well.
Conclusion
In summary, the study demonstrated that a considerable number of patients with advanced HCC received sorafenib treatment in a clinical practice. The median OS of 5.4 months is not so different from the 6.5 months of the Asia-Pacific study, and the median TDS of 2.5 months is similar to the median time to progression of 2.8 months of the Asia-Pacific study. Therefore, the truly therapeutic effect in terms of disease control rate for patients with advanced HCC in the study seems to be similarly poor as shown in the initial report from both the SHARP and Asia-Pacific trials. However, the combination of sorafenib and additional multimodality treatments perhaps may offer survival benefit for patients with advanced HCC. Eventually, a number of patients with a good therapeutic response should be reevaluated for possible surgical resection in order to gain the best outcome as well as cure of HCC.
Key points
The study showed an outcome analysis of patients with advanced HCC under sorafenib treatment from a nationwide population database.
This Taiwan NHI program consists of detailed healthcare information related to claims data and is believed to be the most comprehensive and reliable database for assessing the practice in terms of treatment outcomes of sorafenib in patients with advanced HCC.
The disease control rate of sorafenib in advanced HCC patients in this study appear to act similarly poorer as what has been previously reported by clinical trials.
The combination of multimodality treatments consisting of sorafenib plus locoregional therapy, followed by surgical managements, could provide survival benefits and possibly cure disease for specific groups of few patients with advanced HCC.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank the support of the Maintenance Project of the Center for Big Data Analytics and Statistics (Grant CLRPG3D0044) at Chang Gung Memo rial Hospital and Miss Meng-Jiun Chiou for the statistical assistance and data analysis. This work was supported by grants from Chang Gung Medical Research Program (Grant CLRPG3D0044).
Disclosure
The authors report no conflicts of interest in this work.
References
- StravitzRTHeumanDMChandNSurveillance for hepatocellular carcinoma in patients with cirrhosis improves outcomeAm J Med2008121211912618261500
- LlovetJMBruixJSystematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survivalHepatology200337242944212540794
- LopezPMVillanuevaALlovetJMSystematic review: evidence-based management of hepatocellular carcinoma – an updated analysis of randomized controlled trialsAliment Pharmacol Ther200623111535154716696801
- LlovetJMRicciSMazzaferroVSorafenib in advanced hepatocellular carcinomaN Engl J Med2008359437839018650514
- ChangYSAdnaneJTrailPASorafenib (Bay 43-9006) inhibits tumor growth and vascularization and induces tumor apoptosis and hypoxia in RCC xenograft modelsCancer Chemother Pharmacol200759556157417160391
- WilhelmSCarterCLynchMDiscovery and development of sorafenib: a multikinase inhibitor for treating cancerNat Rev Drug Discov200651083584417016424
- AvilaMABerasainCSangroBPrietoJNew therapies for hepatocellular carcinomaOncogene200625273866388416799628
- CarlomagnoFAnagantiSGuidaTBay 43-9006 inhibition of oncogenic RET mutantsJ Natl Cancer Inst200698532633416507829
- HwangYHChoiJYKimSOver-expression of C-raf-1 proto-oncogene in liver cirrhosis and hepatocellular carcinomaHepatol Res200429211312115163433
- ChengALKangYKChenZEfficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trialLancet Oncol2009101253419095497
- FornerAReigMERodriguez de LopeCBruixJCurrent strategy for staging and treatment: the BCLC update and future prospectsSemin Liver Dis2010301617420175034
- OmataMChengALKokudoNAsia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 updateHepatol Int201711431737028620797
- OmataMLesmanaLATateishiRAsian Pacific association for the study of the liver consensus recommendations on hepatocellular carcinomaHepatol Int20104243947420827404
- BruixJShermanMAmerican Association for the study of liver D. management of hepatocellular carcinoma: an updateHepatology20115331020102221374666
- LuLCChenPJYehYCPrescription patterns of sorafenib and outcomes of patients with advanced hepatocellular carcinoma: a national population studyAnticancer Res20173752593259928476832
- NakanoMTanakaMKuromatsuREfficacy, safety, and survival factors for sorafenib treatment in Japanese patients with advanced hepatocellular carcinomaOncology201384210811423147476
- ShinginaAHashimAMHaqueMIn a ‘real-world’, clinic-based community setting, sorafenib dose of 400 mg/day is as effective as standard dose of 800 mg/day in patients with advanced hepatocellular carcimona, with better tolerance and similar survivalCan J Gastroenterol201327739339623862169
- ChanKMYuMCChouHSWuTJLeeCFLeeWCSignificance of tumor necrosis for outcome of patients with hepatocellular carcinoma receiving locoregional therapy prior to liver transplantationAnn Surg Oncol20111892638264621584831
- AgopianVGHarlander-LockeMPRuizRMImpact of pretransplant bridging locoregional therapy for patients with hepatocellular carcinoma within Milan criteria undergoing liver transplantation: analysis of 3601 patients from the US multicenter HCC transplant ConsortiumAnn Surg2017266352553528654545
- ChenMYWangYCWuTHEfficacy of external beam radiation-based treatment plus locoregional therapy for hepatocellular carcinoma associated with portal vein tumor thrombosisBioMed Res Int20162016419
- KudoMImanakaKChidaNPhase III study of sorafenib after transarterial chemoembolisation in Japanese and Korean patients with unresectable hepatocellular carcinomaEur J Cancer201147142117212721664811
- LencioniRLlovetJMHanGSorafenib or placebo plus TACE with doxorubicin-eluting beads for intermediate stage HCC: the space trialJ Hepatol20166451090109826809111
- MeyerTFoxRMaYTSorafenib in combination with transarterial chemoembolisation in patients with unresectable hepatocellular carcinoma (TACE 2): a randomised placebo-controlled, double-blind, phase 3 trialLancet Gastroenterol Hepatol20172856557528648803
- CaiRSongRPangPTranscatheter arterial chemoembolization plus sorafenib versus transcatheter arterial chemoembolization alone to treat advanced hepatocellular carcinoma: a meta-analysisBMC Cancer201717171429110700
- ChungYHHanGYoonJHInterim analysis of start: study in Asia of the combination of TACE (transcatheter arterial chemoembolization) with sorafenib in patients with hepatocellular carcinoma trialInt J Cancer2013132102448245823129123
- ErhardtAKolligsFDollingerMTACE plus sorafenib for the treatment of hepatocellular carcinoma: results of the multi-center, phase II SOCRATES trialCancer Chemother Pharmacol201474594795425173458
- ChanKMChouHSWuTJLeeCFYuMCLeeWCCharacterization of hepatocellular carcinoma recurrence after liver transplantation: perioperative prognostic factors, patterns, and outcomeAsian J Surg201134312813422208688
- DhirMMelinAADouaiherJA review and update of treatment options and controversies in the management of hepatocellular carcinomaAnn Surg201626361112112526813914
- LeeWCLeeCFChengCHOutcomes of liver resection for hepatocellular carcinoma in liver transplantation eraEur J Surg Oncol20154191144115226163047