
Abstract
Purpose
The aim of this study is to analyze the outcomes of platinum-sensitive (PS) recurrent ovarian cancer treated with pegylated liposomal doxorubicin and carboplatin (CD) versus paclitaxel and carboplatin (CP). Clinical features were examined to characterize the patient population that would benefit from CD.
Materials and methods
This is a retrospective review of 122 cases at a tertiary hospital. Patients with PS recurrent ovarian cancer who received CD or CP were included. Progression-free survival (PFS) and overall survival (OS) were evaluated through the Kaplan–Meier method and log-rank test. Cox proportional hazards regression was used to examine PFS predictors.
Results
In total, 122 patients (75% with first recurrence and 25% with second recurrence) were included. The majority of the patients were diagnosed at an advanced stage and with the histology of serous carcinoma. Median PFS and OS were 14.8 and 55.5 months in the CD group and 13.5 and 56.8 months in the CP group. Subgroup analysis of patients revealed that the CD group had longer median PFS than the CP group among patients with PFI>12 months. Additionally, during the second recurrence, longer PFS was observed in the CD group than in the CP group (medians 22.3 and 13.5 months, respectively, p = 0.019).
Conclusion
Comparable outcomes in recurrent platinum-sensitive ovarian cancer treated with CD versus CP were presented in this study. Longer PFS in CD group was observed among patients with PFI for more than 12 months or in second recurrence.
Introduction
Ovarian cancer is an intractable disease with repeated recurrences and has the worst prognosis among all gynecologic cancers.Citation1 More than 238,000 new cases are diagnosed worldwide each year.Citation2 Although most patients with advanced cancer have responded well to initial cytoreductive surgery followed by chemotherapy, recurrence of the disease is frequent.Citation3,Citation4 Patients commonly experience four to five cycles of chemotherapy and determining the drugs for recurrent ovarian cancer is perplexing. Tumor histology, line of therapy, and quality of life due to the adverse effects of treatment should all be considered.
For decades, taxane with platinum-based treatment has played a major role in platinum-sensitive (PS) recurrent ovarian cancer. However, hair loss and neuropathy caused by the treatment significantly decrease patients’ quality of life.Citation5 Therefore, several carboplatin-based combinations had been explored.Citation6–Citation8 In 2010, the Calypso trial demonstrated that pegylated liposomal doxorubicin with carboplatin (CD) showed superiority over paclitaxel and carboplatin (CP) in progression-free survival (PFS) and less overall toxicity.Citation9,Citation10 CD regimen soon became an attractive alternative for ovarian cancer treatment.
Pegylated liposomal doxorubicin (PLD) is one of the first nanotechnology-based anti-cancer drugs with reduced side effects.Citation11–Citation13 Doxorubicin molecules were loaded in liposome vesicles and have been established as an active cytotoxic agent for recurrent ovarian cancer.Citation7,Citation8 Liposomes are composed of phospholipids and cholesterol on the lipid bilayer and are coated with polyethylene glycol.Citation14,Citation15 Unique pharmacokinetic and pharmacodynamic properties are observed from the different phospholipid formulations. Lipo-Dox® (TTY) is formulated with distearoylphosphatidylcholine (DPLD), while hydrogenated soy phosphatidylcholine (HPLD) is used in Doxil® (Janssen). Compared with Doxil, Lipo-Dox demonstrated a lower clearance rate, longer half-life, and smaller distribution volume, indicating its higher stability in plasma.Citation16
In the Calypso trial, HPLD was used while in our institute, DPLD was administered in CD regimen. Therefore, a confirmatory study to the Calypso trial was prompted. This study is aimed to present the outcomes of PS recurrent ovarian cancer treated with CD using DPLD versus CP. Factors influencing the efficacy of each regimen were analyzed.
Materials And Methods
Study Population
This is a retrospective single institutional study. The medical records of patients with PS recurrent epithelial ovarian cancer, fallopian tube cancer, or peritoneal cancer from 2009 to 2016 were collected. The study was conducted in accordance with the ethical standards of Declaration of Helsinki and was approved by the institutional review board of MacKay Memorial Hospital. A waiver of patient consent was granted because the research involved no more than minimal risk to the participants and the waiver will not adversely affect the rights and welfare of the participants. Patients were considered eligible if recurrence occurred more than 6 months from previous platinum-based treatment and received CD or CP during the relapse.
Study Design
The regimen for CD was DPLD (30 mg/m2, Lipo-Dox®, TTY Biopharm Co., Ltd, Taipei, Taiwan) plus carboplatin (AUC5) every 4 weeks and CP was paclitaxel (175 mg/m2, Taxol®; Bristol-Myers Squibb) plus carboplatin (AUC5) every 3 weeks. Cytoreductive surgery with residual tumor of <1 cm was considered an optimal cytoreductive surgery. Tumor response was evaluated for at least 4 weeks after treatment according to RECIST and GCIG CA-125 criteria. Disappearance of all tumor lesions, according to both computed images and CA-125 level, was considered a complete response. A reduction in CA-125 level ≥50% or measurable lesions was defined as a partial response. Progressive disease was defined as new lesion development, an increase in CA-125 level >25% or increase of initial measurable lesions. Stable disease was defined as a condition not meeting any of the aforementioned criteria. The main outcome was PFS which was determined from the date of first chemotherapy to the date of disease progression, death, or final follow-up. Overall survival (OS) was measured from the date of first chemotherapy to the date of death or final follow-up.
Statistical Analysis
Patient demographics and clinical characteristics were compared using χ2 test and Wilcoxon rank-sum test. PFS and OS were evaluated through the Kaplan–Meier method and log-rank test. Multivariate analysis of predictive factors was performed with significant variables (p<0.1) in the univariate analysis, and hazard ratios (HR) with 95% CI were calculated. All statistical analyses were performed using Statistical Package for Science Software (IBM SPSS, version 20.0, Armonk, NY, USA), and a p-value <0.05 was considered statistically significant.
Results
In total, 122 patients with recurrent PS ovarian cancer who received CD or CP chemotherapy in our hospital were included. Demographic and clinical characteristics of these patients are shown in . The mean ages of the patients were 56 and 53 years, respectively. In both groups, approximately 75% were in first recurrence and 25% with two recurrences. The majority of the patients were diagnosed at an advanced stage (stage III or IV, 81% in the CD group and 64% in the CP group) with histologically confirmed serous carcinoma (80% in the CD group and 68% in the CP group). Patients with an initial stage higher than IC were treated with CP as adjuvant chemotherapy after the primary surgery. The period between the final platinum treatment and relapse ranged from 6.2 to 79.6 months with medians of 12.4 and 14 months, respectively. Similarly, in both groups, the disease recurred within 6 to 12 months in 40% of the patients, 40% of the patients recurred within 12 to 24 months, and 20% of them recurred after 24 months. Detailed toxicities of chemotherapy were not reported in this study; however, the side effects were tolerable and more than 80% of the patients in each group received more than 6 cycles of chemotherapy. Those who received only 3 cycles were mainly by reason of disease progression. Surgical intervention was performed in 50% and 61% of the patients in the CD and CP groups and optimal cytoreductive surgery was achieved in 90% and 83%, respectively. Regarding metastatic sites, relapse with lymph node metastasis was more prevalent in the no surgery group (50% vs 25%).
Table 1 Patient Demographics (N = 122)
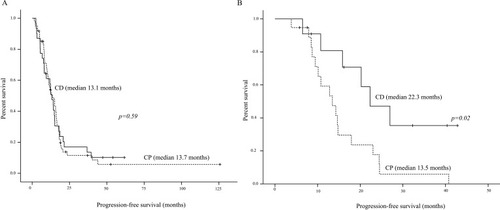
Evaluation of CA-125 levels and computed tomography indicated response rate and disease control rate of 60%, 79% in CD group and 76%, 90% in CP groups. Median PFS was 14.8 months in the CD group and 13.5 months in the CD group (). Median OS was 55.5 months in the CD group and 56.6 months in the CP group. Patients were stratified for subgroup analysis according to platinum-free interval (PFI) and times of recurrence. The results revealed that median PFS was statistically different in the PFI>12 months group. Individuals with PFI>12 months had median PFS as 20.8 and 15.8 months when treated with CD versus CP (). In addition, as shown in , during the second relapse, longer PFS was observed in the CD group than in the CP group (medians of 22.3 months and 13.5 months, respectively, p = 0.02).
Figure 1 Progression-free survival of CP and CD groups.
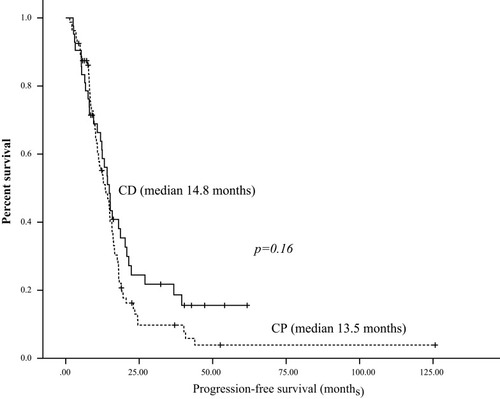
Figure 2 Progression-free survival in relation to platinum-free interval (PFI). (A) Patients with PFI 6–12 months. (B) Patients with PFI >12 months.
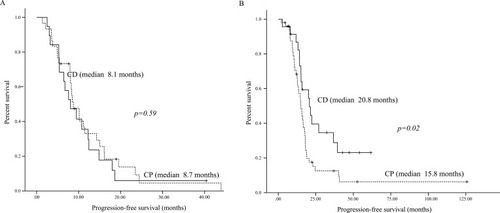
Figure 3 Progression-free survival based on relapse. (A) Patients with first recurrence. (B) Patients with second recurrence.
Exploratory analyses were conducted to determine the prognostic factors including age, initial International Federation of Gynecology and Obstetrics stage, histologic subtypes, surgery at relapse, platinum-free interval, chemotherapy for first relapse, chemotherapy for second relapse, and CA-125 level using Cox proportional hazards regression. Age, PFI, chemotherapy for first and second relapse were statistically significant and multivariate analysis was performed. As shown in , use of CD in the second relapse was statistically significant (hazard ratio [HR], 0.36; p = 0.038).
Table 2 Multivariate Analysis Of Predictive Factors On Progression-Free Survival After Second Relapse
Discussion
With the biological nature of repeated recurrences, quality of life has become an essential factor in decision-making about ovarian cancer treatment. Despite the effectiveness of paclitaxel in ovarian cancer survival, its major side effects of hair loss and neuropathy are distressing for most patients. The Calypso study provided clear proof of therapeutic advantage of CD using HPLD in PS recurrent ovarian cancer with less toxicity. In this study, real-world experience of CD using DPLD in PS ovarian cancer is presented.
In our study, the PFS and OS were 14.8 and 55.5 months for CD group which is comparable with the Calypso study when a median of 11.3 and 30.7 months was reported.Citation9,Citation17 In comparison to the Calypso study, the patient population reported in this study were younger and more percentage of patients received cytoreductive surgery for the recurrence. Four other separate trials of CD in recurrent PS ovarian cancer had been published showing similar median PFS as 9.4–12 months.Citation18–Citation21 In regard to response rate of disease progression, the Calypso study reported 21% and 20% in CD and CP groups whereas in our population, 21% and 10% were observed in CD and CP groups. More cytoreductive surgeries were performed in the present study may contribute to the increased response rate in our CP group.
In this study, median PFS between first and second recurrence was equivalent (12.7 and 12.5 months for first and second recurrence), not shortened as anticipated.Citation22 Notably prolonged PFS for the CD group on second relapse was observed (). Multivariate analysis further confirmed that use of CD is a significant predictor on PFS (HR, 0.36; p = 0.038). The superiority of CD to CP for PFS was even more evident for individuals with PFI >12 months (). In studies of recurrent ovarian cancer, patients with first or second relapses were generally grouped together, and the response to second- or third-line treatment is poorly described independently. In present study, PFS was superior in CD group than CP group in the second relapse which was not observed in the first relapse. Recent advances in the molecular basis of ovarian cancer cells, including intra-tumoral and inter-tumoral heterogeneity lead us to better understanding of the mechanisms for tumor recurrence and therapeutic resistance.Citation23,Citation24 Cancer stem cells with different characteristics may survive from therapies eliminating fast-dividing tumor cells. Growth from the stem cells slowly develops recurrent tumors which may be genetically distinct from previous tumors, thus causing multiple rounds of recurrences and metastases. In summary, alteration of the molecular portraits of tumor cells during the second relapse may contribute to the improved PFS for patients receiving CD.
Over the past decades, much effort has been invested to investigate the molecular basis that predicts the chemosensitivity of recurrent ovarian cancer. Assessment of tumor subtype-specific mutations and molecular aberrations indicated distinct clinical behaviors in recurrent ovarian cancer.Citation25 Most notably, patients with BRCA mutations exhibited delayed relapse and improved prognosis, regardless of platinum sensitivity.Citation26 BRCA-family genes play crucial roles in homologous recombination in the DNA repair pathway (HRD), which is the common pathway for repairing the double-strand breaks caused by chemotherapy. This subset of ovarian cancer with mutation of BRCA or other inherited mutations, such as those of BARD1, CHECK2, and PALB2, related to HRD is referred to as the “BRCAness” phenotype.Citation27,Citation28 Hypersensitivity to platinum and a high response rate to PLD were observed among women with BRCA mutation.Citation29 Moreover, the clinicopathological features of BRCA1 and BRCA2 mutation were discovered to be distinct. BRCA-associated ovarian cancer, especially that associated with BRCA1, tends to metastasize to visceral organs.Citation30 Furthermore, interesting results emerged when investigators started dissecting the implications of BRCA1 and BRCA2 for nonplatinum agents. Both BRCA1- and BRCA2-associated ovarian cancer have been discovered to be more sensitive to PLD compared with BRCA wild type-associated ovarian cancer,Citation31,Citation32 whereas BRCA1-associated ovarian cancer may be more resistant to taxanes.Citation33,Citation34 Determining the chemosensitivity of recurrent ovarian cancer became even more complex after restored protein function was reported after treatment for cancer related to secondary BRCA mutation.Citation35 Investigation of this reversion and its clinical correlations are eagerly anticipated.
Latest treatment of ovarian cancer had even gone beyond combination chemotherapy. Breakthrough drugs as PARP inhibitors,Citation36 anti-angiogenesis bevacizumabCitation37 and immunotherapyCitation38 had yielded promising results. Therefore, current efforts should be focused on optimizing the use of chemotherapy with multiple alternative strategies being carefully evaluated and employed when appropriate in the treatment of ovarian cancer.
The retrospective nature of the study with small sample size is the limitation of our study. Patients were treated with CD or CP according to the physicians’ preference which may cause selection bias. Moreover, toxicity profiles were not precisely documented in the medical records and could not be analyzed in our study. Inclusion of consecutive cases from multiple institutes is necessary to confirm our results.
In conclusion, real-world experience of comparable outcomes in recurrent PS ovarian cancer treated with CD using DPLD versus CP was presented in this study. Improved PFS in individuals treated with CD was observed in the subgroup of patients with PFI for more than 12 months or during second recurrence. Future sequential identification of genomic tumor changes must be exploited and may influence choices for chemotherapeutic drugs.
Ethics Approval And Consent To Participate
This study was conducted in accordance with the regulations on patient confidentiality and the ethical standards of Declaration of Helsinki. This research was approved by the institutional review board of MacKay Memorial Hospital. A waiver of patient consent was granted because the research involved no more than minimal risk to the participants and the waiver will not adversely affect the rights and welfare of the participants.
Available Of Data And Materials
Please contact the corresponding author (Dr Chih-Long Chang) for data requests.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflict of interest in this work.
References
- Momenimovahed Z, Tiznobaik A, Taheri S, Salehiniya H. Ovarian cancer in the world: epidemiology and risk factors. Int J Women’s Health. 2019;11:287–299. doi:10.2147/IJWH.S19760431118829
- Coburn SB, Bray F, Sherman ME, Trabert B. International patterns and trends in ovarian cancer incidence, overall and by histologic subtype. Int J Cancer. 2017;140(11):2451–2460. doi:10.1002/ijc.v140.1128257597
- Piccart MJ, Bertelsen K, Stuart G, et al. Long-term follow-up confirms a survival advantage of the paclitaxel-cisplatin regimen over the cyclophosphamide-cisplatin combination in advanced ovarian cancer. Int J Gynecol Cancer. 2003;13(Suppl 2):144–148.14656271
- Bergamini A, Bocciolone L, Fodor A, Candiani M, Mangili G. Management of recurrent ovarian cancer: when platinum-based regimens are not a therapeutic option. Int J Gynecologic Cancer. 2019;ijgc-2019-000624.
- Khalifa AM, Elsheikh MA, Khalifa AM, Elnaggar YSR. Current strategies for different paclitaxel-loaded Nano-delivery Systems towards therapeutic applications for ovarian carcinoma: a review article. J Controlled Release. 2019;311–312:125–137. doi:10.1016/j.jconrel.2019.08.034
- Parmar MKLJ, Colombo N, Du Bois A, et al. Paclitaxel plus platinum-based chemotherapy versus conventional platinum-based chemotherapy in women with relapsed ovarian cancer: the ICON4/AGO-OVAR-2.2 trial. Lancet. 2003;361(9375):2099–2106.12826431
- Pfisterer J, Plante M, Vergote I, et al. Gemcitabine plus carboplatin compared with carboplatin in patients with platinum-sensitive recurrent ovarian cancer: an intergroup trial of the AGO-OVAR, the NCIC CTG, and the EORTC GCG. J Clin Oncol. 2006;24(29):4699–4707. doi:10.1200/JCO.2006.06.091316966687
- Sehouli J, Chekerov R, Reinthaller A, et al. Topotecan plus carboplatin versus standard therapy with paclitaxel plus carboplatin (PC) or gemcitabine plus carboplatin (GC) or pegylated liposomal doxorubicin plus carboplatin (PLDC): a randomized phase III trial of the NOGGO-AGO-study group-AGO Austria and GEICO-ENGOT-GCIG intergroup study (HECTOR). Ann Oncol. 2016;27(12):2236–2241. doi:10.1093/annonc/mdw41827789470
- Pujade-Lauraine E, Wagner U, Aavall-Lundqvist E, et al. Pegylated liposomal doxorubicin and carboplatin compared with paclitaxel and carboplatin for patients with platinum-sensitive ovarian cancer in late relapse. J Clin Oncol. 2010;28(20):3323–3329. doi:10.1200/JCO.2009.25.751920498395
- Brundage M, Gropp M, Mefti F, et al. Health-related quality of life in recurrent platinum-sensitive ovarian cancer – results from the CALYPSO trial. Ann Oncol. 2012;23(8):2020–2027. doi:10.1093/annonc/mdr58322291207
- Shanmuganathan R, Edison TNJI, LewisOscar F, Kumar P, Shanmugam S, Pugazhendhi A. Chitosan nanopolymers: an overview of drug delivery against cancer. Int J Biol Macromol. 2019;130:727–736. doi:10.1016/j.ijbiomac.2019.02.06030771392
- Pugazhendhi A, Edison TNJI, Velmurugan BK, Jacob JA, Karuppusamy I. Toxicity of Doxorubicin (Dox) to different experimental organ systems. Life Sci. 2018;200:26–30. doi:10.1016/j.lfs.2018.03.02329534993
- Yamada Y, Kawaguchi R, Ito F, et al. Skin-mucous membrane disorder and therapeutic effect of pegylated liposomal doxorubicin in recurrent ovarian cancer. J Obstet Gynaecol Res. 2017;43(7):1194–1199. doi:10.1111/jog.2017.43.issue-728544386
- Gabizon A, Catane R, Uziely B, et al. Barenholz Y: prolonged circulation time and enhanced accumulation in malignant exudates of doxorubicin encapsulated in polyethylene-glycol coated liposomes. Cancer Res. 1994;54(4):987.8313389
- Lorusso D, Sabatucci I, Maltese G, et al. Treatment of recurrent ovarian cancer with pegylated liposomal doxorubicin: a reappraisal and critical analysis. Tumori J. 2019;105(4):282–287. doi:10.1177/0300891619839308
- Hong R-L, Tseng Y-L. Phase I and pharmacokinetic study of a stable, polyethylene-glycolated liposomal doxorubicin in patients with solid tumors. Cancer. 2001;91(9):1826–1833. doi:10.1002/(ISSN)1097-014211335910
- Wagner U, Marth C, Largillier R, et al. Final overall survival results of phase III GCIG CALYPSO trial of pegylated liposomal doxorubicin and carboplatin vs paclitaxel and carboplatin in platinum-sensitive ovarian cancer patients. Br J Cancer. 2012;107(4):588–591. doi:10.1038/bjc.2012.30722836511
- Ferrero JM, Weber B, Geay JF, et al. Second-line chemotherapy with pegylated liposomal doxorubicin and carboplatin is highly effective in patients with advanced ovarian cancer in late relapse: a GINECO phase II trial. Ann Oncol. 2007;18(2):263–268. doi:10.1093/annonc/mdl37617108151
- Alberts DS, Liu PY, Wilczynski SP, et al., Southwest Oncology G. Randomized trial of pegylated liposomal doxorubicin (PLD) plus carboplatin versus carboplatin in platinum-sensitive (PS) patients with recurrent epithelial ovarian or peritoneal carcinoma after failure of initial platinum-based chemotherapy (Southwest Oncology Group Protocol S0200). Gynecol Oncol. 2008;108(1):90–94. doi:10.1016/j.ygyno.2007.08.07517949799
- Power P, Stuart G, Oza A, et al. Efficacy of pegylated liposomal doxorubicin (PLD) plus carboplatin in ovarian cancer patients who recur within six to twelve months: a phase II study. Gynecol Oncol. 2009;114(3):410–414. doi:10.1016/j.ygyno.2009.04.03719520420
- Bafaloukos D, Linardou H, Aravantinos G, et al. A randomized phase II study of carboplatin plus pegylated liposomal doxorubicin versus carboplatin plus paclitaxel in platinum sensitive ovarian cancer patients: a Hellenic Cooperative Oncology Group study. BMC Med. 2010;8:3. doi:10.1186/1741-7015-8-320055981
- Hanker LC, Loibl S, Burchardi N, et al. The impact of second to sixth line therapy on survival of relapsed ovarian cancer after primary taxane/platinum-based therapy. Ann Oncol. 2012;23(10):2605–2612. doi:10.1093/annonc/mds20322910840
- Jiménez-Sánchez A, Memon D, Pourpe S, et al. Heterogeneous tumor-immune microenvironments among differentially growing metastases in an ovarian cancer patient. Cell. 2017;170(5):927–938.e920. doi:10.1016/j.cell.2017.07.02528841418
- Roberts CM, Cardenas C, Tedja R. The role of intra-tumoral heterogeneity and its clinical relevance in epithelial ovarian cancer recurrence and metastasis. Cancers. 2019;11(8):1083. doi:10.3390/cancers11081083
- Hollis RL, Gourley C, L Hollis R. Genetic and molecular changes in ovarian cancer. Cancer Biol Med. 2016;13(2):236–247. doi:10.20892/j.issn.2095-3941.2016.002427458531
- Safra T, Borgato L, Nicoletto MO, et al. Grenader TJMct: BRCA mutation status and determinant of outcome in women with recurrent epithelial ovarian cancer treated with pegylated liposomal doxorubicin. Mol Cancer Ther. 2011;10(10):2000–2007. doi:10.1158/1535-7163.MCT-11-027221835933
- Tan DS, Rothermundt C, Thomas K, et al. Gore MEJJoCO: “BRCAness” syndrome in ovarian cancer: a case-control study describing the clinical features and outcome of patients with epithelial ovarian cancer associated with BRCA1 and BRCA2 mutations. J Clin Oncol. 2008;26(34):5530–5536. doi:10.1200/JCO.2008.16.170318955455
- Hollis RL, Churchman M, Gourley CJO. Therapy: distinct implications of different BRCA mutations: efficacy of cytotoxic chemotherapy, PARP inhibition and clinical outcome in ovarian cancer. OncoTargets Ther. 2017;10:2539.
- Hollis RL, Meynert AM, Churchman M, et al. Enhanced response rate to pegylated liposomal doxorubicin in high grade serous ovarian carcinomas harbouring BRCA1 and BRCA2 aberrations. BMC Cancer. 2018 Jan 3;18(1):16. doi:10.1186/s12885-017-3981
- Gourley C, Michie CO, Roxburgh P, et al. Reed NJJoCO: increased incidence of visceral metastases in Scottish patients with BRCA1/2-defective ovarian cancer: an extension of the ovarian BRCAness phenotype. J Clin Oncol. 2010;28(15):2505–2511. doi:10.1200/JCO.2009.25.108220406939
- Adams SF, Marsh EB, Elmasri W, et al. A high response rate to liposomal doxorubicin is seen among women with BRCA mutations treated for recurrent epithelial ovarian cancer. Gynecol Oncol. 2011;123(3):486–491. doi:10.1016/j.ygyno.2011.08.03221945552
- Safra T, Borgato L, Nicoletto MO, et al. BRCA mutation status and determinant of outcome in women with recurrent epithelial ovarian cancer treated with pegylated liposomal doxorubicin. Mol Cancer Ther. 2011;10(10):2000–2007. doi:10.1158/1535-7163.MCT-11-027221835933
- Quinn JE, James CR, Stewart GE, et al. BRCA1 mRNA expression levels predict for overall survival in ovarian cancer after chemotherapy. Clin Cancer Res. 2007;13(24):7413–7420. doi:10.1158/1078-0432.CCR-07-108318094425
- Tan DSP, Yap TA, Hutka M, et al. Implications of BRCA1 and BRCA2 mutations for the efficacy of paclitaxel monotherapy in advanced ovarian cancer. Eur J Cancer. 2013;49(6):1246–1253. doi:10.1016/j.ejca.2012.11.01623265709
- Mayor P, Gay LM, Lele S, Elvin JA. BRCA1 reversion mutation acquired after treatment identified by liquid biopsy. Gynecologic Oncol Rep. 2017;21:57–60. doi:10.1016/j.gore.2017.06.010
- Markman M. Pharmaceutical management of ovarian cancer: current status. Drugs. 2019;79(11):1231–1239. doi:10.1007/s40265-019-01158-131267481
- Shoji T, Eto H, Sato T, et al. A new therapeutic strategy for recurrent ovarian cancer – bevacizumab beyond progressive disease. Healthcare. 2019;7:3. doi:10.3390/healthcare703010930497933
- Lee EK, Konstantinopoulos PA. Combined PARP and Loibl S, Burchardi N immune checkpoint inhibition in ovarian cancer. Trends Cancer. 2019;5(9):524–528. doi:10.1016/j.trecan.2019.06.00431474356