
Abstract
Objective
To evaluate the correlation between systemic inflammation markers and sarcopenia in elderly patients with esophageal squamous cell carcinoma (ESCC) and their prognostic value.
Materials and Methods
The clinical data of 121 elderly patients with ESCC were collected. The skeletal muscle area at the level of the third lumbar vertebrae (L3) was measured by computed tomography (CT), and then the skeletal muscle index (SMI) was calculated. The neutrophil-to-lymphocyte ratio (NLR), prognostic nutritional index (PNI) and Geriatric Nutritional Risk Index (GNRI) were calculated according to laboratory standards. Univariate and multivariate Cox proportional hazards models were used to determine prognostic factors for overall survival (OS).
Results
A total of 121 elderly ESCC patients were enrolled. Among them, 65 patients had sarcopenia. NLR, PNI and GNRI are significantly related to sarcopenia. The OS of ESCC patients with sarcopenia and/or NLR>2.24 was significantly worse.
Conclusion
PNI, GNRI, NLR and sarcopenia were significantly related. Sarcopenia and NLR are independent prognostic factors for elderly ESCC, and when combined have better prognostic value.
Introduction
Esophageal cancer is a highly aggressive malignancy. Its incidence rate and mortality rate are very high, ranking ninth and sixth in the world, respectively.Citation1 The prognosis of patients with esophageal cancer is poor, and the 5-year survival rate is only 18%.Citation2 The main pathological types of esophageal carcinoma include esophageal squamous cell carcinoma (ESCC) and adenocarcinoma. At present, surgical treatment is still the main treatment for ESCC. With the gradual progress of population ageing, the number of elderly patients with ESCC is gradually increasing. The treatment of elderly patients with ESCC is an important challenge. Therefore, the prognostic evaluation of elderly patients with ESCC is very important to guide the treatment plan and follow-up strategy.
The progressive growth of tumors in ESCC patients often causes the mechanical obstruction of the esophagus as well as symptoms of progressive dysphagia, which leads to reduced nutritional intake in ESCC patients, and then leads to cachexia.Citation3 Many studies have focused on the nutritional status of cancer patients. The Geriatric Nutritional Risk Index (GNRI) is a simplified screening tool based on serum albumin and body weight that can be used to assess nutrition-related risks.Citation4 The prognostic nutritional index (PNI) is calculated by the serum albumin concentration and the total number of peripheral blood lymphocytes.Citation5 Sarcopenia is a manifestation of body cachexia, which is mainly manifested as a gradual decline in the strength and quality of skeletal muscle.Citation6 Because the early symptoms of esophageal cancer are often not considered, most patients can only take in liquid or are unable to eat before going to the doctor, which also causes their nutritional status to be poor. We also found that systemic inflammation is a risk factor for sarcopenia.Citation7 Sarcopenia has been used as a predictor of poor prognosis in many gastrointestinal malignancies.Citation8 The reduction in skeletal muscle mass measured by computed tomography (CT) is considered to be the gold standard for the diagnosis of sarcopenia.Citation9
Complete blood cell count is an easy and inexpensive test in clinical treatment. The systemic inflammatory response is considered to play an important role in the occurrence and development of cancer.Citation10 The systemic inflammatory response of cancer patients shows significant changes.Citation11–Citation13 Studies have confirmed that lymphocyte and platelet count, platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR) and neutrophil-to-lymphocyte ratio (NLR) are related to the prognosis of many cancers.Citation14–Citation16
The purpose of this study was to explore the relationship between preoperative systemic inflammation, GNRI, PNI and sarcopenia in elderly ESCC patients and to evaluate their correlation with the prognosis of ESCC patients.
Materials and Methods
Study Population and Design
From September 2013 to August 2017, 121 elderly patients with ESCC were recruited from the First Affiliated Hospital of Guangxi Medical University (Nanning, China). The inclusion criteria were as follows: (a) ESCC proved by pathology; (b) McKeown or Ivor-Lewis esophagectomy; (c) no distant metastasis found in preoperative examination; (d) age ≥ 65 years; and (e) complete clinical and follow-up data. The exclusion criteria were as follows: (a) the presence of other malignant tumors; (b) incomplete resection (R1 and R2); and (c) patients with systemic infections and blood diseases. Preoperative blood test results, including complete blood count, albumin, etc., were collected. All blood samples were sent to the same laboratory for analysis. A complete blood count and measurement of height and weight were performed one week before surgery, and then the values of neutrophils (N), platelets (P), monocytes (M), lymphocytes (L) and red blood cell distribution width (RDW), NLR as N/L, MLR as M/L, PLR as P/L were recorded.Citation17 The PNI was calculated using the following formula: 10×serum albumin value (g/dl) +0.005×total lymphocyte count in the peripheral blood (per mm3).Citation5 Body mass index (BMI) was calculated as the square of weight (kg)/height (m2). GNRI was calculated as follows: GNRI=1.489×serum albumin (g/dl) + 41.7×the weight/ideal body weight.Citation4 We use the 8th edition of the American Joint Committee on Cancer (AJCC) TNM grading system to stage patients after surgery. The study was conducted in accordance with the Declaration of Helsinki. All patients in the study provided written informed consent, and the study was approved by the Ethics Committee of the First Affiliated Hospital of Guangxi Medical College, and the Ethical approval number was 2021 (KY-E-045).
Skeletal Muscle Tissue Measurement
An enhanced CT scan of the abdomen of the patient during the week before treatment was used to collect two consecutive images at the third lumbar vertebrae (L3) level. L3 skeletal muscles include the paraspinal muscles, psoas major, rectus abdominis, internal oblique, external oblique, and transverse abdominal muscles.Citation18 The skeletal muscle index (SMI) was calculated as the square of the skeletal muscle area (cm2)/height (m2). Sarcopenia was defined as the sex-specific cut-off value of L3 SMI ≤52.4cm2/m2 for males and ≤38.5cm2/m2 for females, which correlates with mortality determined by optimal stratification.Citation19
Follow-Up
The deadline for follow-up was December 1, 2020. The patients were followed up through outpatient follow-up visits or telephone interviews. Overall survival (OS) was defined as the time from surgery to the last follow-up or death from any cause.
Statistical Analysis
All statistical analysis was performed using SPSS version 19.0 (SPSS Inc., Chicago, Illinois, USA), and graphs were drawn using GraphPad Prism version 5.0 (GraphPad software, Inc., La Jolla, CA, USA) and R version 4.0.2 (https://www.r-project.org/). The time-dependent receiver operating characteristic (ROC) curve was used to determine the clinical index cut-offs, optimal sensitivity, specificity and area under the curve (AUC). Logistic regression analysis was used to evaluate the relationship between sarcopenia and systemic inflammation indicators. Kaplan-Meier analysis was performed to construct survival curve. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using univariate and multivariate Cox proportional hazards regression models. According to the results of univariate and multivariate Cox regression analysis, a clinical prediction model nomogram was constructed, and then the calibration curve and concordance index (C index) were used to evaluate the prediction accuracy of the nomogram. P<0.05 was considered statistically significant.
Results
Baseline Characteristics of the Patients and Tumors
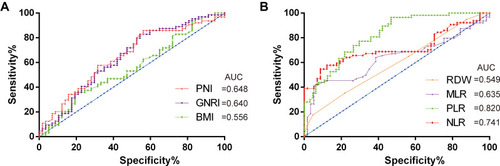
A total of 121 patients with ESCC were enrolled. The clinical characteristics of the patients are shown in . The median age was 69 years (65–86 years and 70.34±4.57 years). Sixty-five patients (53.7%) had sarcopenia. We constructed the ROC curves () to determine the cut-off value, sensitivity, specificity and AUC value, which were 92.9, 82.8%, 45.6%, and 0.640 (95% CI =0.541–0.740) for GNRI; 43.35, 85.9%, 44.9%, and 0.648 (95% CI =0.550–0.747) for PNI; and 22.49, 35.9%, 80.7%, and 0.556 (0.453–0.659) for BMI in 121 elderly ESCC patients.
Table 1 Baseline Characteristics of Patients and Tumors
Figure 1 The receiver-operating characteristic (ROC) curves for (A) GNRI, BMI and PNI; (B) Inflammation index.
Systemic Inflammation Markers
The cut-off value, sensitivity, specificity and AUC value of systemic inflammation markers were determined according to the ROC curve (). The cut-off value, sensitivity, specificity and AUC in our cohort were 2.24, 91.2%, 54.7% and 0.714 (95% CI =0.620–0.808) for NLR; 0.135, 35.1%, 78.1% and 0.594 (95% CI=0.493–0.695) for RDW; 129.65, 96.5%, 53.1% and 0.820 (95% CI=0.747–0.892) for PLR; and 0.295, 94.7%, 40.6% and 0.635 (95% CI=0.534–0.735) for MLR.
Correlation Between Sarcopenia and Clinical Features
We conducted logistic regression analysis on the clinical and pathological characteristics of sarcopenia and patients and systemic inflammation indicators to confirm the relationship between them (). We found that GNRI (OR = 0.436, 95% CI= 0.194–0.982, P = 0.045), PNI (OR = 0.418, 95% CI= 0.182–0.957, P = 0.039), and NLR (OR = 3.750, 95% CI = 1.762–7.979, P=0.001) were significantly related to sarcopenia.
Table 2 Association Between Clinical Parameters and Sarcopenia
Survival Analysis and Risk Factors for OS
The follow-up period ended on December 1, 2020. A total of 57 patients died. The median follow-up period was 39.0 months (range, 1–82). Univariate Cox analysis () showed that lymphatic metastasis, cancer embolus, degree of differentiation, tumor depth, sarcopenia, GNRI, PNI, MLR, PLR and NLR were significantly related to OS. We performed multivariate Cox analysis on the statistically significant indicators in the univariate Cox analysis (). We found that sarcopenia and NLR were independent prognostic factors for elderly patients with ESCC.
Table 3 Univariate and Multivariate Analyses of Overall Survival (OS) in the Eligible Patients
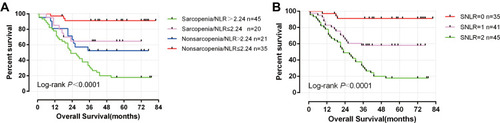
Survival analysis showed that patients with sarcopenia had significantly lower OS than those without sarcopenia (P<0.0001, ), and patients with a high NLR had a significantly lower OS than patients with a low NLR (P<0.0001, ). According to the presence of sarcopenia and the NLR value (>2.24 or ≤2.24), we divided the 121 elderly ESCC patients into four subgroups: sarcopenia/NLR>2.24, sarcopenia/NLR≤2.24, no muscle loss symptoms/NLR> 2.24 and no sarcopenia/NLR ≤ 2.24. We found that compared with patients in the other groups, the OS of patients with sarcopenia/NLR>2.24 was significantly worse (P<0.0001, ). We combined the two subgroups and established the sarcopenia and NLR (SNLR) group to evaluate the combined prognostic value of SNLR in elderly ESCC patients, defined as follows: no sarcopenia or NLR≤2.24 was assigned 0 points (N=35); sarcopenia or NLR>2.24 was assigned 1 point (N=41); and both sarcopenia and NLR>2.24 was assigned two points (N=45). Survival analysis showed that patients with an SNLR score of 0 had a significantly longer OS than patients with a score of 1 or 2 (P<0.0001, ).
Figure 2 Kaplan–Meier survival curve of overall survival in patients: (A) Sarcopenia; (B) NLR.
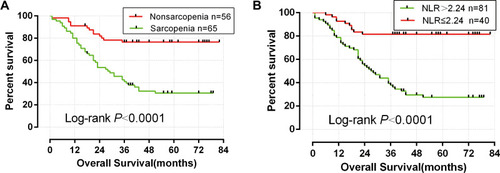
Figure 3 Kaplan–Meier survival curve of overall survival in patients: (A) Sarcopenia and NLR; (B) SNLR.
Survival Prediction Nomogram Model
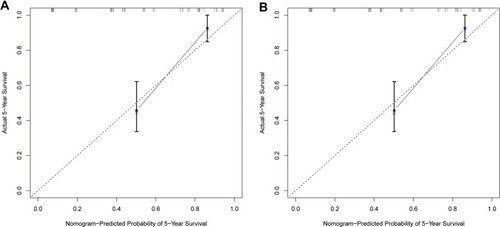
Based on the results of multivariate Cox analysis, we established a nomogram for elderly ESCC patients (). The results showed that NLR had the greatest impact on OS, followed by lymphatic metastasis, sarcopenia and tumor depth. At the same time, we evaluated the prognostic value of sarcopenia and NLR combined. We constructed nomograms integrating SNLR, lymphatic metastasis and tumor depth (). We found that SNLR was the most important factor for OS, followed by lymphatic metastasis and tumor depth. We used the Coxph method to calculate two nomograms, which had accuracy values of 0.759 and 0.761. By establishing a 5-year OS model for the two nomograms (–), we found that there was a consistency between the predicted survival probabilities and the actual survival probabilities.
Figure 4 Nomogram for esophageal squamous cell carcinoma. The points identified on the top scale for each independent covariate were added to determine the estimated overall survival and the probability of 1-, 3- and 5- year survival. (A) non-SNMR-based nomogram of overall survival. (B) SNMR-based nomogram of overall survival.
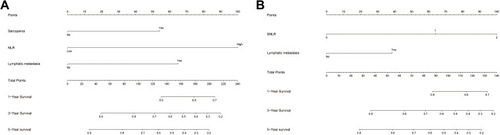
Figure 5 The calibration plot for 5-year survival of (A) non-SNLR and (B) SNLR. The X-axis presents the predicted probability and the Y -axis shows the actual probability.
Discussion
Many studies have confirmed that sarcopenia and systemic inflammation are related to the prognosis of various cancers. At present, with the ageing of the world’s population, the proportion of elderly people is gradually increasing. The ageing process is related to a decline in skeletal muscle mass, and elderly individuals are more likely to suffer from sarcopenia.Citation20 Some studies have shown that sarcopenia is not an independent prognostic factor after neoadjuvant treatment for esophageal cancer.Citation21 However, other studies have confirmed that for elderly patients with ESCC, sarcopenia is an independent prognostic factor after neoadjuvant chemotherapy.Citation22 Therefore, the role of sarcopenia in neoadjuvant therapy still needs further research. Some studies have confirmed the relationship between sarcopenia and the prognosis of patients with ESCC,Citation23–Citation25 while other studies have confirmed the relationship between systemic inflammation and the prognosis of patients with ESCC. However, these studies did not explore the relationship between sarcopenia and systemic inflammation. Therefore, the relationship between sarcopenia and systemic inflammation and its prognostic role in elderly ESCC patients are still unclear. Whether there is a correlation between sarcopenia and systemic inflammation and its prognostic value are unclear. Therefore, it is necessary to study the prognostic value of sarcopenia and systemic inflammation in elderly patients with ESCC. Through research, we can confirm that NLR and sarcopenia are independent prognostic factors for elderly ESCC patients, sarcopenia is significantly related to NLR, and a higher NLR may cause sarcopenia. Through the joint survival analysis of sarcopenia and NLR, we found that ESCC patients with sarcopenia and high NLR had poor OS. By combining sarcopenia and NLR, we found that elderly ESCC patients with an SNLR score of 0 had a significantly better prognosis. Through the nomogram, we found that sarcopenia had a greater impact on the OS of elderly ESCC patients, and SNLR had the greatest impact on the OS of elderly ESCC patients. Surgery is still the first choice for the treatment of resectable esophageal cancer. In today’s ageing population, our findings have important clinical significance.
For elderly patients with ESCC, due to the special characteristics of this population, elderly ESCC patients are prone to complications and sarcopenia during surgery.Citation26 Therefore, the lack of nutrition in the elderly patients with ESCC is a problem worthy of attention. Due to the characteristics of mechanical obstruction in the esophagus caused by esophagus cancer, the incidence of malnutrition in patients with esophageal cancer is significantly higher.Citation27 A previous study found that ESCC patients with a lower GNRI had a significantly worse prognosis,Citation28,Citation29 and another study found that a low PNI was significantly associated with poor prognosis in ESCC patients.Citation30 However, in ESCC patients undergoing radical resection of esophageal cancer, the negative effects of surgery and subsequent treatment will further aggravate the original sarcopenia. Although in this study, GNRI and PNI were not independent prognostic factors for ESCC patients, sarcopenia was significantly related to PNI and GNRI. ESCC patients with low PNI and GNRI are more likely to develop sarcopenia. At the same time, sarcopenia has been indicated to have a variety of adverse effects in patients, including a decreased ability to live independentlyCitation31 and an increased chance of accidental falls and fractures.Citation32 These are all factors that lead to poor prognosis in elderly ESCC patients with sarcopenia. Therefore, in the treatment of elderly ESCC patients, a personalized and adequate treatment plan is very important.
Previous studies have found that skeletal muscle can secrete interleukin 15 (IL-15).Citation33 IL-15 can bind to natural killer (NK) lymphocytes with high affinity through a variety of signaling pathways and protect NK cells from apoptosis by upregulating bcl-2 to ensure the normal development and survival of NK cells.Citation34 Elderly ESCC patients with sarcopenia have a significant decrease in skeletal muscle mass, which will lead to a decrease in IL-15 secretion, resulting in a decline in the antitumor ability of the immune system, leading to tumor progression and ultimately a poor prognosis.
The relationship between sarcopenia and systemic inflammation is very close. Skeletal muscle tissue secretes numerous proinflammatory factors, such as TNF-α and IL-6, leading to the progression of systemic inflammation.Citation34 However, certain proinflammatory factors can promote the decomposition of skeletal muscle and inhibit the differentiation of skeletal muscle cells by inflammatory cells and tumor cells, leading to skeletal muscle atrophy.Citation35 This muscle atrophy caused by inflammation further aggravates systemic inflammation, leading to harmful inflammation- related muscle weakness.Citation36 Previous studies have also found that PNI is significantly related to tumor-infiltrating lymphocytes (TILs). TILs are a special histological feature of human cancer and reflect the individual immune response of tumors.Citation30 Our study also found that in elderly ESCC patients, sarcopenia is significantly related to NLR, and both are independent prognostic factors for ESCC patients. Patients with a higher NLR have more significant sarcopenia. We believe that this is because systemic inflammation induces the release of proinflammatory cytokines and growth factors, which in turn has a catabolic effect on host metabolismCitation37 and ultimately leads to a decrease in skeletal muscle mass.Citation38
Our research has certain limitations. Our study is a retrospective study, and it was only conducted in a single center. It is necessary to conduct further large-scale cohort studies to obtain more specific results and validate our findings.
Conclusion
GNRI, NRI and NLR are significantly associated with sarcopenia. Both sarcopenia and NLR are independent predictors of postoperative OS in elderly ESCC patients, and they have good comprehensive prognostic value. Sarcopenia and NLR are easily obtained clinical indicators.
Disclosure
The authors declare that they have no competing interests.
Acknowledgments
This work was supported in part by the National Natural Science Foundation of China (81660387) and Development and Application of Medical and Health Appropriate Technology of Guangxi (S201654).
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.2149230207593
- Peery AF, Crockett SD, Barritt AS, et al. Burden of gastrointestinal, liver, and pancreatic diseases in the United States. Gastroenterology. 2015;149(7):1731–1741 e1733. doi:10.1053/j.gastro.2015.08.04526327134
- Mariette C, De Botton ML, Piessen G. Surgery in esophageal and gastric cancer patients: what is the role for nutrition support in your daily practice? Ann Surg Oncol. 2012;19(7):2128–2134. doi:10.1245/s10434-012-2225-622322948
- Bouillanne O, Morineau G, Dupont C, et al. Geriatric nutritional risk index: a new index for evaluating at-risk elderly medical patients. Am J Clin Nutr. 2005;82(4):777–783. doi:10.1093/ajcn/82.4.77716210706
- Onodera T, Goseki N, Kosaki G. [Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients]. Nihon Geka Gakkai Zasshi. 1984;85(9):1001–1005. Japanese.6438478
- Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on sarcopenia in older people. Age Ageing. 2010;39(4):412–423. doi:10.1093/ageing/afq03420392703
- Wallengren O, Iresjo BM, Lundholm K, Bosaeus I. Loss of muscle mass in the end of life in patients with advanced cancer. Support Care Cancer. 2015;23(1):79–86. doi:10.1007/s00520-014-2332-y24975045
- Shachar SS, Williams GR, Muss HB, Nishijima TF. Prognostic value of sarcopenia in adults with solid tumours: a meta-analysis and systematic review. Eur J Cancer. 2016;57:58–67. doi:10.1016/j.ejca.2015.12.03026882087
- Mourtzakis M, Prado CM, Lieffers JR, Reiman T, McCargar LJ, Baracos VE. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab. 2008;33(5):997–1006. doi:10.1139/H08-07518923576
- Templeton AJ, McNamara MG, Seruga B, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014;106(6):dju124. doi:10.1093/jnci/dju12424875653
- Balkwill F, Mantovani A. Cancer and inflammation: implications for pharmacology and therapeutics. Clin Pharmacol Ther. 2010;87(4):401–406. doi:10.1038/clpt.2009.31220200512
- Zheng L, Zou K, Yang C, Chen F, Guo T, Xiong B. Inflammation-based indexes and clinicopathologic features are strong predictive values of preoperative circulating tumor cell detection in gastric cancer patients. Clin Transl Oncol. 2017;19(9):1125–1132. doi:10.1007/s12094-017-1649-728315180
- Bozkaya Y, Kurt B, Gurler F. A prognostic parameter in advanced non-small cell lung cancer: the ratio of hemoglobin-to-red cell distribution width. Int J Clin Oncol. 2019;24(7):798–806. doi:10.1007/s10147-019-01417-x30783810
- Wang Y, Li Y, Chen P, Xu W, Wu Y, Che G. Prognostic value of the pretreatment systemic immune-inflammation index (SII) in patients with non-small cell lung cancer: a meta-analysis. Ann Transl Med. 2019;7(18):433. doi:10.21037/atm.2019.08.11631700869
- Toda M, Tsukioka T, Izumi N, et al. Platelet-to-lymphocyte ratio predicts the prognosis of patients with non-small cell lung cancer treated with surgery and postoperative adjuvant chemotherapy. Thorac Cancer. 2018;9(1):112–119. doi:10.1111/1759-7714.1254729105365
- Watanabe K, Yasumoto A, Amano Y, et al. Mean platelet volume and lymphocyte-to-monocyte ratio are associated with shorter progression-free survival in EGFR-mutant lung adenocarcinoma treated by EGFR tyrosine kinase inhibitor. PLoS One. 2018;13(9):e0203625. doi:10.1371/journal.pone.020362530192878
- Walsh SR, Cook EJ, Goulder F, Justin TA, Keeling NJ. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J Surg Oncol. 2005;91(3):181–184. doi:10.1002/jso.2032916118772
- Onishi S, Tajika M, Tanaka T, et al. Prognostic significance of sarcopenia in patients with unresectable advanced esophageal cancer. J Clin Med. 2019;8(10):1647. doi:10.3390/jcm8101647
- Prado CM, Lieffers JR, McCargar LJ, et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol. 2008;9(7):629–635. doi:10.1016/S1470-2045(08)70153-018539529
- Rosenberg IH. Sarcopenia: origins and clinical relevance. J Nutr. 1997;127(5 Suppl):990S–991S. doi:10.1093/jn/127.5.990S9164280
- Grun J, Elfinger L, Le H, et al. The influence of pretherapeutic and preoperative sarcopenia on short-term outcome after esophagectomy. Cancers. 2020;12(11):3409. doi:10.3390/cancers12113409
- Onishi S, Tajika M, Tanaka T, et al. Prognostic impact of sarcopenic obesity after neoadjuvant chemotherapy followed by surgery in elderly patients with esophageal squamous cell carcinoma. J Clin Med. 2020;9(9):2974. doi:10.3390/jcm9092974
- Harada K, Ida S, Baba Y, et al. Prognostic and clinical impact of sarcopenia in esophageal squamous cell carcinoma. Dis Esophagus. 2016;29(6):627–633. doi:10.1111/dote.1238126123787
- Nishigori T, Okabe H, Tanaka E, Tsunoda S, Hisamori S, Sakai Y. Sarcopenia as a predictor of pulmonary complications after esophagectomy for thoracic esophageal cancer. J Surg Oncol. 2016;113(6):678–684. doi:10.1002/jso.2421426936808
- Nakashima Y, Saeki H, Nakanishi R, et al. Assessment of sarcopenia as a predictor of poor outcomes after esophagectomy in elderly patients with esophageal cancer. Ann Surg. 2018;267(6):1100–1104. doi:10.1097/SLA.000000000000225228437312
- Wagner D, DeMarco MM, Amini N, et al. Role of frailty and sarcopenia in predicting outcomes among patients undergoing gastrointestinal surgery. World J Gastrointest Surg. 2016;8(1):27–40. doi:10.4240/wjgs.v8.i1.2726843911
- Jordan T, Mastnak DM, Palamar N, Kozjek NR. Nutritional therapy for patients with esophageal cancer. Nutr Cancer. 2018;70(1):23–29. doi:10.1080/01635581.2017.137441729016197
- Kubo N, Sakurai K, Tamura T, et al. The impact of geriatric nutritional risk index on surgical outcomes after esophagectomy in patients with esophageal cancer. Esophagus. 2019;16(2):147–154. doi:10.1007/s10388-018-0644-630311102
- Migita K, Matsumoto S, Wakatsuki K, et al. The prognostic significance of the geriatric nutritional risk index in patients with esophageal squamous cell carcinoma. Nutr Cancer. 2018;70(8):1237–1245. doi:10.1080/01635581.2018.151264030235009
- Okadome K, Baba Y, Yagi T, et al. Prognostic nutritional index, tumor-infiltrating lymphocytes, and prognosis in patients with esophageal cancer. Ann Surg. 2020;271(4):693–700. doi:10.1097/SLA.000000000000298530308614
- Dos Santos L, Cyrino ES, Antunes M, Santos DA, Sardinha LB. Sarcopenia and physical independence in older adults: the independent and synergic role of muscle mass and muscle function. J Cachexia Sarcopenia Muscle. 2017;8(2):245–250. doi:10.1002/jcsm.1216027897417
- Schaap LA, van Schoor NM, Lips P, Visser M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: the longitudinal aging study amsterdam. J Gerontol a Biol Sci Med Sci. 2018;73(9):1199–1204. doi:10.1093/gerona/glx24529300839
- Quinn LS. Interleukin-15: a muscle-derived cytokine regulating fat-to-lean body composition. J Anim Sci. 2008;86(14 Suppl):E75–83. doi:10.2527/jas.2007-045817709786
- Lutz CT, Quinn LS. Sarcopenia, obesity, and natural killer cell immune senescence in aging: altered cytokine levels as a common mechanism. Aging (Albany NY). 2012;4(8):535–546. doi:10.18632/aging.10048222935594
- Lin JX, Lin JP, Xie JW, et al. Prognostic value and association of sarcopenia and systemic inflammation for patients with gastric cancer following radical gastrectomy. Oncologist. 2019;24(11):e1091–e1101. doi:10.1634/theoncologist.2018-065130910865
- Kalinkovich A, Livshits G. Sarcopenic obesity or obese sarcopenia: a cross talk between age-associated adipose tissue and skeletal muscle inflammation as a main mechanism of the pathogenesis. Ageing Res Rev. 2017;35:200–221.27702700
- Feliciano EMC, Kroenke CH, Meyerhardt JA, et al. Association of systemic inflammation and sarcopenia with survival in nonmetastatic colorectal cancer: results from the C SCANS Study. JAMA Oncol. 2017;3(12):e172319. doi:10.1001/jamaoncol.2017.231928796857
- Fearon KC, Glass DJ, Guttridge DC. Cancer cachexia: mediators, signaling, and metabolic pathways. Cell Metab. 2012;16(2):153–166. doi:10.1016/j.cmet.2012.06.01122795476