
Abstract
Purpose
Cancer patients have faced intersecting crises during the COVID-19 pandemic. This review aimed to examine patients’ and caregivers’ experiences of accessing cancer services during the pandemic and its perceived impact on their psychological wellbeing.
Patients and Methods
A protocol-led (CRD42020214906) systematic review was conducted by searching six databases including EMBASE, MEDLINE and CINAHL for articles published in English-language between 1/2020 and 12/2020. Data were extracted using a pilot-tested, structured data extraction form. Thematic synthesis of data was undertaken and reported as per the PRISMA guideline.
Results
A total of 1110 articles were screened, of which 19 studies met the inclusion criteria. Studies originated from 10 different countries including the US, UK, India and China. Extracted data were categorised into seven themes. Postponement and delays in cancer screening and treatment, drug shortages and inadequate nursing care were commonly experienced by patients. Hospital closures, resource constraints, national lockdowns and patient reluctance to use health services due to infection worries contributed to the delay. Financial and social distress, isolation, and spiritual distress were also commonly reported. Caregivers in addition felt anxious about infecting cancer patients with COVID-19.
Conclusion
Patients and caregivers experienced delays in cancer screening, treatment and care during the COVID-19 pandemic and negatively affected their psychological wellbeing. Their views and preferences should be accounted to minimise the impact of the current and any future pandemics and ensure resilient cancer services.
Protocol Registration
Published protocol registered with Centre for Review and Dissemination CRD42020214906 (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=214906).
Introduction
Coronavirus disease 2019 (COVID-19), caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2),Citation1 has challenged the resilience of healthcare systems and economies globally. The pandemic has placed an immense strain on cancer services, resulting in disruptions largely due to measures necessary to minimise patient exposure to the virus coupled with strains on health services resources. Such disruptions for cancer patients can accentuate the poor prognosis compared to non-cancer patients.Citation2 Notably, the overall case fatality rate due to COVID-19 for cancer patients during initial phase of the pandemic was reported to be 23.4% (95% Cl= 9.7% to 40.5%) compared to 5.9% (95% Cl= 1.9% to 11.7%) for non-cancer patients.Citation3 Data estimates suggest that a reduction of up to 85% in US-based cancer screening services at the height of the first wave (March–July 2020).Citation4 In England, urgent referrals for suspected cancer were down 16% (348,000 referrals) compared with data in the previous year.Citation5 Given that early diagnosis and timely access to appropriate treatment modality are critical factors for positive patient outcomes,Citation2,Citation6–Citation8 The number of avoidable cancer-related deaths is therefore predicted to substantially increase.Citation6 These service interruptions are also likely to impact negatively those receiving or awaiting palliative care.
The pandemic and the consequent disruption in health services have led many to suggest that cancer has become the “forgotten C”.Citation9,Citation10 Whilst current research places appropriate emphasis on the relationship between COVID-19 and treatment adjustments and survival outcomes,Citation3,Citation6–Citation8,Citation11,Citation12 it is important to consider patient and caregiver views and experiences. These could inform the further development of resilient cancer services for the current and future pandemics. This systematic review aimed to examine patients’ and caregivers’ experiences of accessing cancer services during the COVID-19 pandemic and the perceived impact on psychological wellbeing.
Methods
The systematic review was conducted and reported in accordance with the recommendation of Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines,Citation13 based on a published protocol (CRD42020214906). Reporting was done as per PRISMA checklist [13] (electronic Supplementary Material 2).
Literature Search
CINAHL, EMBASE, MEDLINE, Google Scholar, Wellcome Open Research and Authorea (for unpublished studies and ongoing peer reviews) databases were searched systematically using medical subject headings (MeSH) and free-text keywords including “cancer”, ‘oncology, and “Coronavirus”, ‘COVID-19ʹ and related terms (electronic Supplementary Material 1) from January 2020 till December 2020. Boolean operators were used to refine the search.
Inclusion and Exclusion Criteria
Studies published in English on the views, experiences and perceived impact of COVID-19 on cancer screening and care from the perspectives of patients/public and/or their caregivers (both formal and informal) were included. The search was not restricted to any cancer types (including palliative care), settings or participant demography.
Screening and Selection
Initial screening of titles was conducted independently by two investigators (SD and VP), with any disagreements resolved through discussion and consultation with a third investigator where needed. Title screening was followed by abstract and full-text screening with reference to the inclusion and exclusion criteria.
Data Extraction and Analysis
Data were extracted by one author (SD) and confirmed by another author (VP) using a pilot tested, structured data collection form. A thematic synthesis was adopted to analyse the extracted data, which were reported into themes and subthemes.Citation14
Quality Assessment
A Critical Appraisal Skills Programme (CASP) tool was used to assess the quality of qualitative studiesCitation15 and the “NIH Quality of Observational, Cohort and Cross-Sectional Studies Assessment Tool” for survey studies.Citation16 Quality assessment was undertaken by SD and VP.
Results
Characteristics and Quality of Included Studies
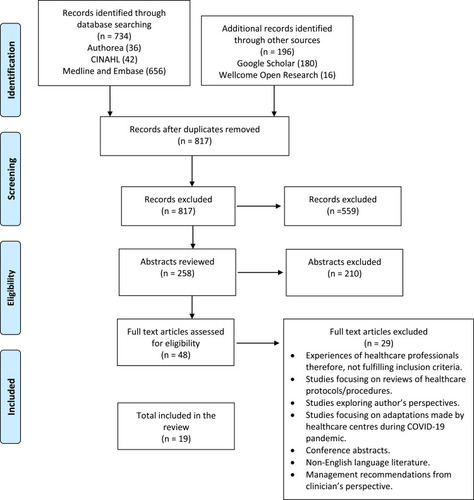
The initial search yielded 1110 results, with 19Citation17–Citation35 included in data extraction and synthesis (). Studies reported experiences from participants in 10 countries, largely Italy (n=4) the US (n=3), India (n=3), the UK and the Netherlands (n=2 each). The majority of studies employed a cross-sectional survey methodology (n=14) and five were qualitative ( and ). Results of quality assessment are presented in electronic Supplementary Material 3 and 4.
Table 1 Characteristics of Qualitative Studies and Key Results
Table 2 Characteristics of Quantitative Studies and Key Results
Figure 1 PRISMA diagram.
Results of Thematic Synthesis
Seven key themes of synthesised data and several subthemes were identified, relating to experiences of accessing cancer screening and diagnosis; experiences of accessing cancer treatment and care services; communication in relation to cancer care; perceived risks of infection; anxiety and fear; adverse impact on personal life, family and finances; resilience and coping mechanisms and caregivers’ specific concerns ().
Table 3 Emerging Themes and Subthemes from Thematic Synthesis
Experiences of Accessing Cancer Screening and Diagnostic Services
Disruption to cancer screening and diagnosis was a commonly reported theme. A cross-sectional survey assessing the experiences of sarcoma patients at two of the largest specialist sarcoma centres in Europe reported that one-third experienced postponement of appointments or scans by at least three months.Citation35 Patients also reported cancellations of routine follow-up clinic appointments in studies conducted in the UK and US.Citation31,Citation34 In a further two studies, patients expressed anxiety and fear due to postponement of cancer-related laboratory tests and diagnostic imaging.Citation24,Citation31 This overwhelming sense of anxiety amongst patients was further demonstrated in one study, with patients describing the pandemic as overshadowing the needs of families and severely affecting the quality and scope of cancer services.Citation29 Some patients described their experiences of COVID-19 prevention taking precedence over cancer treatment and care.Citation29
Experiences of Accessing Cancer Treatment and Care Services
Participants in most studies reported treatment delays,Citation17,Citation18,Citation20,Citation22,Citation24–Citation31 for a number of varied reasons including hospital cancellations, city lockdowns and COVID-19 testing requirements. Deferral of planned radiotherapy and very long appointment waiting were amongst the issues cited by a number of participants in a study conducted in India.Citation30 Participants in a US study study reported that radiation, infusion therapies and surgical tumour removal were subject to severe disruption.Citation31 The impact on cancer surgery was highlighted in a US study, where 10 of 38 participants experiencing delays for ovarian cancer surgery.Citation24 A study conducted at a tertiary-care referral hospital in Italy reported a median surgery waiting time of 53 days (IQR: 35–72 days) which was reported to be a marked increase on pre-pandemic waiting times.Citation26
A study based in India reported additional issues of access including the deferral of nutritionist input, lack of availability of psychological counselling and peer group support services.Citation30 There was a dearth of availability to online counselling services.
Emotional distress was common in patients who had experienced disruption.Citation28 The uncertainty surrounding medication availability and the lack of nursing care available for patients was an issue, particularly for those living alone.Citation22,Citation30 For example, patients with cervical and oral cancer struggled to source certain dressing materials and had utilise defective dressings.Citation22 Family and friends were prohibited from accompanying patients to appointments and visiting inpatients, leading to distress for both. In a study conducted at a palliative care centre in the US, participants likened the experience to being “prisoners in a cage”.Citation21
Communication in Relation to Cancer Care
Disruptions to regular communications between patients and health services were commonly reported, with many studies reporting the use of remote forms of communications including telecommunication and telephone.Citation17,Citation20,Citation22,Citation30,Citation35 Patients identified positive aspects of telecommunication for example, the ease of accessing care from the privacy and comfort of one’s home and the ability to maintain physical distance.Citation22 The majority of patients in one study hoped for continuation of online services post-pandemic.Citation25 In another study, almost two-thirds of patients felt that they were still able to contact the healthcare team and so expressed feelings of reassurance.Citation35 However, in one study conducted in India, patients reported difficulties in booking virtual appointments and unpredictable network issues.Citation30
Anxiety, Fear and Perceived Risk of Infection
Feelings of anxiety and fear surrounding the pandemic were common, with eighteen studies referencing changes in emotional and psychological functioning.Citation17–Citation30,Citation32–Citation35 Approximately 55% of the 204 participants in one study conducted in a tertiary-institution felt that it was not safe to visit the hospital.Citation17 Notably, cancer patients expressed fear about the consequences and complications arising from them contracting COVID-19.Citation17 There were emotional reactions to the prospect of not being able to say a final farewell to family and friends.Citation33 References were also made to fears surrounding family members contracting the virus and patients expressed worries and concerns about treatment delays due to the postponement of elective procedures.Citation32 More than half of the participants in a US study reported new-onset of anxiety or depression.Citation24 Nearly a quarter (23% of the 204) participants in one study were in receipt of the government “shielding” advice.Citation34
Studies conducted in Saudi Arabia and Iran examined anxiety responses amongst children and their caregivers.Citation17,Citation29 Parents reported fears surrounding COVID-19 mortality rates and expressed concerns about the high transmissibility and limited knowledge surrounding the virus.Citation29 In one of these studies, over two-thirds of parents reported the onset of new behavioural issues amongst their children since the pandemic.Citation17 Parents were worried about the negative effects of the pandemic on children’s mental and physical health, both now and in the long-term.
Adverse Impact on Personal Life, Family and Finances
Ten studies reported consequences of the pandemic on cancer patients’ personal lives, their families and the potential finances.Citation17,Citation19,Citation22,Citation24,Citation28,Citation29,Citation32–Citation35 Impact on social activities due to lockdowns was also described, with loneliness fuelling patients’ worries about their cancer.Citation33 Concerns surrounding loss of income and employment instability for cancer patients and family members were reported.Citation35 Those receiving palliative care expressed frustration and fear at the possibility of not being able to fulfil their last wishes.Citation22
Caregiver Specific Concerns
Concerns raised by caregivers were reported in two studies.Citation22,Citation33 In one study, conducted in the Netherlands, more than half of the participants reported being worried about infecting cancer patients with COVID-19.Citation33 In another study, caregivers reported feelings of guilt due to their inability to ease their relatives’ suffering and, in some cases, were reluctant to provide appropriate care (eg, changing dressings) due to worries about transmitting COVID-19.Citation22 Moreover, caregivers reported that once lockdown commenced, they experienced feelings of helplessness as social distancing impacted their ability to provide adequate care.Citation22
Employment uncertainty was often reported to divert caregivers’ focus from caring to attempting to address the financial strain, worsening feeling of guilt.Citation22 There were also reports of the difficulties arising from a lack of clear information and guidance about COVID-19 and its potential impact on already vulnerable cancer patients.Citation22
Developing Resilience and Coping Mechanisms
Patient and/or carer strategies to developing resilience and coping mechanisms were described in five studies.Citation19,Citation28,Citation29,Citation33,Citation35 For example, in one paediatric hospital-based study, patients reported that, together with their families, they altered their attitudes towards COVID-19 nervousness and fear to regain control of living with the virus.Citation29 In two further studies, patients emphasised their appreciation for everyday life and reported feeling content as a result of lockdown.Citation28,Citation33 They reported that the lockdown offered them the time to reflect positively and focus on the “silver lining”, creating a sense of peace which appeared to ease their worries.Citation28 Several patients who were house bound due to their cancer reported a sense of belonging with the rest of the community being in lockdown.Citation33
Discussion
Discussion of Key Findings and Implications
This is the first systematic review that has explored the impact of the pandemic on the experiences of cancer patients and their caregivers regarding the impact on aspects of cancer screening and care. The review has identified major recurring themes of barriers to accessing cancer screening and diagnosis; anxiety and fear; perceived risks of infection; adverse impact on personal life, family and finances; caregivers concerns and resilience; and coping mechanisms adopted by patients and carers.
The entire landscape of cancer management has changed as a result of the COVID-19 pandemic.Citation36 This is reinforced by findings of this review which also adds to the evidence based on the experiences of patients and carers. As a result of diagnostic and treatment delays, governments and health systems are expecting a surge in the number of avoidable, cancer-related deaths.Citation2 Participants in studies included in this review expressed concerns surrounding incomplete treatment, complications associated with contracting COVID-19 and changes to their psychological and emotional wellbeing. The suspension of cancer screening, cancellation of routine oncology appointments and postponement of treatment were linked to increased feelings of stress and anxiety; suggesting that there is a critical gap in disaster preparedness.Citation37 Consequently, vulnerable patients were at greater risk of poor cancer outcomes, with further implications for mental health, symptom control and quality of life. For patients actively seeking end of life treatment, it was evident that strict social distancing measures limited caregiver–patient interactions and many caregivers felt disheartened that they could not provide support during this crucial time.Citation22,Citation33 However, the evidence base relating to caregivers is limited, with only two studies reporting their perspectives. Further research in this key population is warranted.
Anxiety and fear, and perceived risk of infection when using cancer services were commonly reported. For example, a study conducted in Gaza reported that prior to COVID-19, only one toilet was available for public use in the oncology department and with cancer patients expressing their fears about the lack of social distancing and, close proximity.Citation18 The World Health Organization (WHO) has also voiced concern about the lack of personal protective equipment (PPE) and drug deficit.Citation38 The repercussions of resource limitations on cancer treatment outcomes outlined above needs to be explored further.Citation39
Lessons learnt from this pandemic should become an integral part of the management of cancer patients, including those receiving palliative care, ensuring a continuum of cancer care. Future pandemic preparedness is necessary in order to minimise the disruption experienced by both cancer patients and their caregivers. Efforts should firstly be placed on restoring cancer services with the prioritisation of screening, early detection and diagnosis. As primary care is focal to diagnosis, it is vital that patients with symptoms are encouraged to present, feeling comfortable to seeking medical help and are then assessed in a timely manner.Citation40 Remote consulting comes with many communication challenges for example, “missed cues” which would may be more apparent in face-to-face consultations.
Introducing innovations such as triage tests for patients reporting a specific set of symptoms may help to address such challenges and ensure that prompt referrals are made.Citation40 The consequent delay of treatment due to COVID-related measures should be considered on an individual, case by case basis for each patient; ensuring that critical patients receive adequate therapy. Alongside this, the public health implications of potentially delaying treatment versus COVID-19 prevention should be assessed.
Internationally, the professional cancer societies, including The American Society of Clinical Oncology (ASCO), have produced guidance in relation to safe provision and continuity of cancer care during the pandemic.Citation41,Citation42 While this guidance advocates greater flexibility and alternative treatment options to suit patient circumstances, the impact on personal, psychological and financial wellbeing on patients need to be considered. Patient centred communications from health service providers to address patient fears of contracting the virus while on treatment and reluctance to use health services are essential.
Throughout the pandemic, it is necessary to evaluate detection rates, treatment uptake and outcomes so that valid pre-pandemic comparisons can be made. It is also imperative to consider healthcare professionals’ and wider stakeholders’ experiences of delivering cancer services. Roles of non-medical healthcare professionals including pharmacists can be diversified to support cancer servicesCitation43–Citation45 including their roles in administering COVID-19 vaccination.Citation46 Novel, faster and accurate methods of detection of symptomatic and asymptomatic COVID-19 can minimise disruptions to the services in the future.Citation46,Citation47
Strengths and Limitations
The review was conducted using a rigorous and systematic approach in line with best practice. There are, however, a number of limitations. The search period was limited to one year; given the very dynamic and ever changing nature of the pandemic and the associate literature, it is possible that new studies will rapidly emerge. In synthesising data from studies conducted in a number of countries, the differing healthcare structures and processes may impact the generalisability and transferability of the findings.
Conclusion
This systematic review suggests that globally cancer patients are experiencing postponement and delays in the cancer screening and treatment, drug shortages and inadequate nursing care were commonly experienced. These factors contributed to anxiety, loneliness and fear amongst patients and carers. Lockdowns, financial issues faced by patients and patient reluctance to use services contributed to the treatment delays and cancellations. Future service models should incorporate patient and caregiver views identified from this study. Improving infection control measures and vaccination rates can bring COVID-19 infection down to manageable levels and minimise cancer service disruptions.
Abbreviations
ASCO, The American Society of Clinical Oncology; CASP, Critical Appraisal Skills Programme; NIH, National Institute of Health; PPE, personal protective equipment; PRISMA, Preferred Reporting Items for Systematic Review and Meta-analysis.
Data Sharing Statement
The data underlying this article are available in the article and https://www.dovepress.com/get_supplementary_file.php?f=12189801.docx Supplementary Materials submitted with the manuscript.
Disclosure
The authors declare that they have no conflicts of interest in this work.
Acknowledgments
We would like to thank the University of Birmingham Library services for their support in the search process.
References
- National Institute of Allergy and Infectious Diseases. Coronaviruses. Available from: https://www.niaid.nih.gov/diseases-conditions/coronaviruses. Accessed 310, 2020.
- Maringe C, Spicer J, Morris M, et al. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: a national, population-based, modelling study. Lancet Oncol. 2020;21(8):1023–1034.32702310
- Zhang H, Han H, He T, et al. Clinical characteristics and outcomes of COVID-19-infected cancer patients: a systematic review and meta-analysis. J Natl Cancer Inst. 2020. doi:10.1093/jnci/djaa168
- Patt D, Gordan L, Diaz M, et al. Impact of COVID-19 on cancer care: how the pandemic is delaying cancer diagnosis and treatment for American seniors. JCO Clin Cancer Info. 2020;4:1059–1071. doi:10.1200/CCI.20.00134
- Cancer Research UK. 2000 fewer people in England began cancer treatment in January. Available from: https://www.cancerresearchuk.org/about-us/cancer-news/news-report/2021-03-11-2000-fewer-people-in-england-began-cancer-treatment-in-january. Accessed 412, 2021.
- Gheorghe A, Maringe C, Spice J, et al. Economic impact of avoidable cancer deaths caused by diagnostic delay during the COVID-19 pandemic: A national population-based modelling study in England, UK. Eur J Cancer. 2021;152:233–242.
- Neal RD, Tharmanathan P, France B. Is increased time to diagnosis and treatment in symptomatic cancer associated with poorer outcomes? Systematic review. Br J Cancer. 2015;112(suppl 1):S92–S107. doi:10.1038/bjc.2015.4825734382
- Burki TK. Cancer guidelines during the COVID-19 pandemic. Lancet Oncol. 2020;21(5):629–630. doi:10.1016/S1470-2045(20)30217-532247319
- Yorkshire Evening Post. Leeds mum diagnosed with stage four cancer months after screening was cancelled due to Covid. Available from: https://www.yorkshireeveningpost.co.uk/health/leeds-mum-diagnosed-stage-four-cancer-months-after-screening-was-cancelled-due-covid-3038701. Accessed 720, 2021
- Macmillan Cancer Support. ‘The forgotten ‘C’? The impact of COVID-19 on cancer care. Available from: https://www.macmillan.org.uk/assets/forgotten-c-impact-of-covid-19-on-cancer-care.pdf. Accessed 720, 2021
- Hartman HE, Sun Y, Devasia TP, et al. Integrated survival estimates for cancer treatment delay among adults with cancer during the COVID-19 pandemic. JAMA Oncol. 2020;6(12):1881–1889. doi:10.1001/jamaoncol.2020.540333119036
- Carreira H, Strongman H, Peppa M, et al. Prevalence of COVID-19-related risk factors and risk of severe influenza outcomes in cancer survivors: a matched cohort study using linked English electronic health records data. eClinicalMedicine. 2020;29:100656. doi:10.1016/j.eclinm.2020.10065633437952
- Moher D, Liberati A, Tetzlaff J, Altman DG, Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.100009719621072
- Lucas PJ, Baird J, Arai L, Law C, Roberts HM. Worked examples of alternative methods for the synthesis of qualitative and quantitative research in systematic reviews. BMC Med Res Method. 2007;7(1):1–7. doi:10.1186/1471-2288-7-4
- Critical Appraisal Skills Programme. Critical appraisal skills programme (CASP) checklists. Available from: https://casp-uk.net/casp-tools-checklists/. Accessed 315, 2021.
- National Heart, Lung and Blood Institute. Quality assessment tool for observational cohort and cross-sectional studies. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed 1105, 2020.
- AlShahrani M, Elyamany G, Sedik Q, et al. The impact of COVID-19 pandemic in children with cancer: a report from Saudi Arabia. SAGE Open. 2020. doi:10.1177/1178632920984161
- AlWaheidi S, Sullivan R, Davies EA. Additional challenges faced by cancer patients in Gaza due to COVID- 19. eCancer Med Sci. 2020;14:ed100. doi:10.3332/ecancer.20202.ed.100
- Casanova M, Pagani Bagliacca E, Silva M, et al. How young patients with cancer perceive the COVID‐19 (coronavirus) epidemic in Milan, Italy: is there room for other fears? Pediatr Blood Cancer. 2020;67(7):e28318. doi:10.1002/pbc.28318.32240567
- de Joode K, Dumoulin DW, Engelen V, et al. Impact of the Coronavirus disease 2019 pandemic on cancer treatment: the patients’ perspective. Eur J Cancer. 2020;136:132–139. doi:10.1016/j.ejca.2020.06.01932683273
- Desideri I, Ciccone PL, Stocchi G, et al. Impact of COVID-19 on patient-doctor interaction in a complex radiation therapy facility. Support Care Cancer. 2020:1–7. doi:10.1007/s00520-020-05793-3.
- Dhavale P, Koparkar A, Fernandes P. Palliative care interventions from a social work perspective and the challenges faced by patients and caregivers during COVID-19. Indian J Palliat Care. 2020;26(5):58–62. doi:10.4103/IJPC.IJPC_149_20
- Falcone R, Grani G, Ramundo V, et al. Cancer care during COVID-19 era: the quality of life of patients with thyroid malignancies. Front Oncol. 2020. doi:10.3389/fonc.2020.01128.24
- Frey MK, Ellis AE, Zeligs K, et al. Impact of the coronavirus disease 2019 pandemic on the quality of life for women with ovarian cancer. Am J Obstet Gynecol. 2020;223(5):725–e1. doi:10.1016/j.ajog.2020.06.04932598911
- Ghosh J, Ganguly S, Mondal D, Pandey P, Dabkara D, Biswas B. Perspective of oncology patients during COVID-19 pandemic: a prospective observational study from India. J Glob Oncol. 2020;6(6):844–851. doi:10.1200/GO.20.00172
- Greco F, Altieri VM, Esperto F, Mirone V, Scarpa RM. Impact of COVID-19 pandemic on health-related quality of life in uro-oncologic patients: what should we wait for? Clin Genitourin Cancer. 2020. doi:10.1016/j.clgc.2020.07.008
- Guven DC, Sahin TK, Aktepe OH, Yildirim HC, Aksoy S, Kilickap S. Perspectives, knowledge, and fears of cancer patients about COVID-19. Front Oncol. 2020;10:1553. doi:10.3389/fonc.2020.0155333014800
- Hyland KA, Jim HSL. Behavioural and psychosocial responses of people receiving treatment for advanced lung cancer during the COVID‐19 pandemic: a qualitative analysis. Psycho-Oncol. 2020;29(9):1387–1392. doi:10.1002/pon.5445
- Mirlashari J, Ebrahimpour F, Salisu WJ. War on two fronts: experience of children with cancer and their family during COVID-19 pandemic in Iran. J Pediatr Nurs. 2021;57:25–31. doi:10.1016/j.pedn.2020.10.02433212343
- Mitra M, Basu M. A study on challenges to health care delivery faced by cancer patients in India during the COVID-19 pandemic. J Prim Care Community Health. 2020;11:1–5. doi:10.1177/2150132720942705
- Papautsky EL, Hamlish T. Patient-reported treatment delays in breast cancer care during the COVID-19 pandemic. Breast Cancer Res Treat. 2020;184(1):249–254. doi:10.1007/s10549-020-05828-732772225
- Qian Y, Wu K, Xu H, et al. A survey on physical and mental distress among cancer patients during the COVID-19 epidemic in Wuhan, China. J Palliat Med. 2020;23(7):888–889. doi:10.1089/jpm.2020.024032408790
- Schellekens MPJ, van der Lee M. Loneliness and belonging: exploring experiences with the COVID-19 pandemic in psycho-oncology. Psycho-Oncol. 2020;29(9):1399–1401. doi:10.1002/pon.5459
- Swainston J, Chapman B, Grunfeld EA, Derakshan N. COVID-19 lockdown and its adverse impact on psychological health in breast cancer. Front Psychol. 2020;11:2033. doi:10.3389/fpsyg.2020.62603832982846
- Younger E, Smrke A, Lidington E, et al. Health-related quality of life and experiences of sarcoma patients during the COVID-19 pandemic. Cancers. 2020;12(8):2288. doi:10.3390/cancers12082288
- Jones D, Neal RD, Duffy SRG, Scott SE, Whitaker KL, Brain K. Impact of the COVID-19 pandemic on the symptomatic diagnosis of cancer: the view from primary care. Lancet Oncol. 2020;21(6):748–750. doi:10.1016/S1470-2045(20)30242-432359404
- International Federation of Red Cross and Red Crescent. Disaster preparedness. Available from: https://media.ifrc.org/ifrc/what-we-do/disaster-and-crisis-management/disaster-preparedness/. Accessed 402, 2021.
- World Health Organisation. Occupied Palestinian territory COVID-19 response plan 2020. Available from: https://www.who.int/health-cluster/countries/occupied-palestinian-territory/Occupied-Palestinian-Territory-COVID-19-Humanitarian-Response-Plan-April-2020.pdf?ua=1. Accessed 720, 2021. Accessed 4 15, 2021.
- Jazieh AR, Akbulut H, Curigliano G, et al. Impact of the COVID-19 pandemic on cancer care: a global collaborative study. JCO Glob Oncol. 2020;6:1428–1438. doi:10.1200/GO.20.0035132986516
- Neal RD, Nekhlyudov L, Wheatstone P, Koczwara B. Cancer care during and after the pandemic. Br Med J. 2020;370:m2622. doi:10.1136/bmj.m262232616512
- NHS England. NHS England interim treatment options during the COVID-19 pandemic. Available from: https://www.nice.org.uk/guidance/ng161/resources/interim-treatment-change-options-during-the-covid19-pandemic-endorsed-by-nhs-england-pdf-8715724381. Accessed 720, 2021.
- American Society Clinical Oncology, (ASCO). ASCO special report: a guide to cancer care delivery during the COVID-19 pandemic. Available from: https://www.asco.org/sites/new-www.asco.org/files/content-files/2020-ASCO-Guide-Cancer-COVID19.pdf. Accessed 428, 2021.
- Hussain AZ, Paudyal V, Hadi MA. Impact of the COVID-19 pandemic on the prescribing patterns of first-line antibiotics in english primary care: a longitudinal analysis of national prescribing dataset. Antibiotics. 2021;10(5):591. doi:10.3390/antibiotics1005059134067546
- Paudyal V, Sun S, Hussain R, Abutaleb MH, Hedima EW. Complementary and alternative medicines use in COVID-19: A global perspective on practice, policy and research. Research in Social and Administrative Pharmacy. 2021. doi:10.1016/j.sapharm.2021.05.004
- Paudyal V, Cadogan C, Fialová D, et al. Provision of clinical pharmacy services during the COVID-19 pandemic: experiences of pharmacists from 16 European countries. Res Soc Administrative Pharm. 2020;30:46.
- Paudyal V, Fialová D, Henman MC, Hazen A, Okuyan B, Lutters M, Cadogan C, Da Costa FA, Galfrascoli E, Pudritz YM, Rydant S. Pharmacist’s involvement in COVID-19 vaccination across Europe: a situational analysis of current practice and policy. International Journal of Clinical Pharmacy. 2021. 10.1007/s11096-021-01301-7
- Manigandan S, Wu MT, Ponnusamy VK, Raghavendra VB, Pugazhendhi A, Brindhadevi K. A systematic review on recent trends in transmission, diagnosis, prevention and imaging features of COVID-19. Process Biochem. 2020;98:233–240. doi:10.1016/j.procbio.2020.08.01632843849
- Islam MM, Karray F, Alhajj R, Zeng J. A review on deep learning techniques for the diagnosis of novel coronavirus (covid-19). IEEE Access. 2021;9:30551–30572. doi:10.1109/ACCESS.2021.3058537