Abstract
Background
Sorafenib has been approved in the indication of unresectable hepatocellular carcinoma, but there are many cases in which administration of the drug is discontinued due to severe side effects. In this study, we compared the characteristics of patients who continued and discontinued sorafenib.
Methods
Ninety-six patients (75 men and 21 women) were initiated on sorafenib from July 2009 through September 2011. The patient characteristics of interest included gender, age, etiology, Child-Pugh classification, treatment history and frequency, and levels of α-fetoprotein, des- gamma-carboxy prothrombin, aspartate amino acid transferase, and alanine aminotransferase. Duration of administration of sorafenib and reasons for its discontinuation were compared.
Results
Median overall survival was 11.8 months. Discontinuation of sorafenib within 90 days was identified as an independent prognostic factor for overall survival on multivariate analysis (P < 0.0001). Transarterial chemoembolization performed six times or more (P = 0.013) was also identified as an independent factor contributing to discontinuation of sorafenib within 90 days in multivariate analysis. Patients who received sorafenib for ≥90 days had significantly longer overall survival than those who discontinued it (P < 0.0001).
Conclusion
Prolonged treatment with sorafenib is an important factor in achieving extended overall survival. We recommend starting sorafenib before latent liver damage has occurred as a result of too many transarterial chemoembolization procedures.
Introduction
In general, hepatocellular carcinoma in its early stages can be treated by surgical resection, radiofrequency ablation,Citation1,Citation2 or liver transplantation when there is a single nodule ≤ 5 cm or three nodules ≤ 3 cm (Milan criteria).Citation3 However, many people are diagnosed in the advanced stages, when only transcatheter arterial infusion chemotherapy and transarterial chemoembolization are performed,Citation4,Citation5 but despite recently improved embolization devices,Citation6 even these therapies have limited success in cases of vascular invasion or extrahepatic spread.Citation7 Because hepatocellular carcinoma has a high recurrence rate, it is important to prevent secondary disease, and several therapies have been reported to prevent recurrence, including interferon,Citation8 retinoids,Citation9 and branched-chain amino acids.Citation10
Recently, a number of molecularly targeted agents have been investigated throughout the world,Citation11–Citation13 and some agents are entering Phase II or III trials.Citation14,Citation15 Sorafenib inhibits the serine/threonine kinases, RAF-1and B-Raf,Citation16,Citation17 inhibits the tyrosine kinase activity of vascular endothelial growth factor receptors 1, 2, and 3 and platelet-derived growth factor receptor β,Citation16,Citation17 which has been shown to trigger production of reactive oxygen species and death of hepatocellular carcinoma cells.Citation18
Sorafenib was approved to treat hepatocellular carcinoma in 2007,Citation19 and is used in patients with advanced stage disease. In two well known studies, sorafenib significantly increased survival time in patients with hepatocellular carcinoma, although there were absolute differences in survival time between the two patient populations because the definition of advanced disease differed between the two studies.Citation20,Citation21
Although administration of 800 mg of sorafenib is recommended, there are many cases in which administration is discontinued or the dosage is reduced because of severe side effects.Citation15,Citation20,Citation22 In this study, we demonstrated the therapeutic effects of sorafenib retrospectively and compared the characteristics of patients who continued and discontinued treatment with this agent.
Materials and methods
Patients
We enrolled 96 patients who had started to receive the drug in our hospital or at one of six affiliated hospitals from July 2009 through September 2011 and were able to be observed for more than 90 days. The patient characteristics investigated included gender, age, etiology, Child-Pugh classification, treatment history and frequency, levels of α-fetoprotein, des-gamma-carboxy prothrombin, aspartate amino acid transferase, and alanine aminotransferase, as well as treatment received prior to administration of sorafenib, eg, surgery, percutaneous ethanol injection therapy, percutaneous microwave coagulation therapy, radiofrequency ablation, transarterial chemoembolization, transcatheter arterial embolization, and/or transcatheter arterial infusion. The effectiveness of the treatments was evaluated according to modified Response Evaluation Criteria In Solid Tumors (RECIST)Citation23 using an enhanced computed tomography scan every 3 months. Duration of administration of sorafenib was noted and the reasons for its discontinuation were identified.
Treatment plan and toxicity evaluation
Sorafenib was initiated at 800 mg/day in two divided doses,Citation24 and dose reduction was allowed for unacceptable adverse effects, ie, grade 3/4 toxicities, and treatment was continued until disease progression, development of intolerable drug toxicity, or patient refusal to continue taking the drug. Patients were followed up on an outpatient basis every 2–4 weeks. Adverse events were assessed according to the National Cancer Institute Common Toxicity Criteria for Adverse Events, version 4.0.
Statistical analysis
Overall survival was estimated using the Kaplan-Meier method, and differences in survival between the groups were compared using the log-rank test. Cox’s proportional hazard model and logistic regression were used to examine likely prognostic factors in each group. The results were reported as hazard ratios with 95% confidence intervals. P < 0.05 was considered to be statistically significant for all analyses. All statistical analyses were performed using JMP version 7.2 software (SAS Institute, Cary, NC).
Results
Patient characteristics
The 96 patients comprised 75 men and 21 women of mean age of 71.2 ± 16.8 (median 71) years (see ). The etiology was hepatitis C virus in 56, hepatitis B virus in 15, and others in 25. Median (range) levels of α-fetoprotein, des- gamma-carboxy prothrombin, aspartate (U/L), and alanine aminotransferase (U/L) were 88.7 (3.2–245,500) ng/mL, 559 (5–75,000) mAU/mL, 54 (19–165) IU/L, and 33 (12–150) IU/L, respectively. Fifty, 44, and two patients had an Eastern Cooperative Oncology Group performance status of 0, 1, and 2, respectively. Child-Pugh classification was 5 in 62, 6 in 30, and 7 in four. Barcelona Clinic Liver Cancer (BCLC) staging was B in 37 and C in 59. Twenty-seven patients had metastatic disease in organs other than the liver. Prior medical history at the time of initiation of sorafenib therapy was surgery in 32, percutaneous ethanol injection therapy in 11, percutaneous microwave coagulation therapy in one, radiofrequency ablation in 42, transarterial chemoembolization and/or transcatheter arterial embolization in 72, transcatheter arterial infusion in 19, and radiation in five cases.
Table 1 Baseline patient characteristics and previous therapy before administration of sorafenib
Efficacy, response, and disease control rates
Median overall survival was 11.8 months. No patients had a complete response, 13 patients (14%) had a partial response, and 31 (32%) had stable disease (according to modified RECIST criteria), whereas 30 patients (31%) had progressive disease and 22 patients were not evaluable. The disease control rate was 46% and the response rate was 14% (see and ).
Figure 1 Overall survival for all patients.
Note: Median overall survival was 11.8 (range 7–763) days.
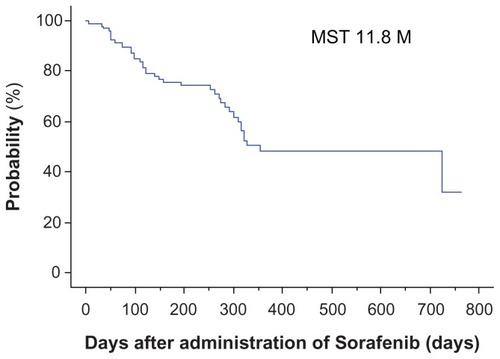
Figure 2 Relationship between continuation of administration and overall survival.
Note: In the group that continued administration for ≥90 days, overall survival was significantly higher than in the group that discontinued administration within 90 days.
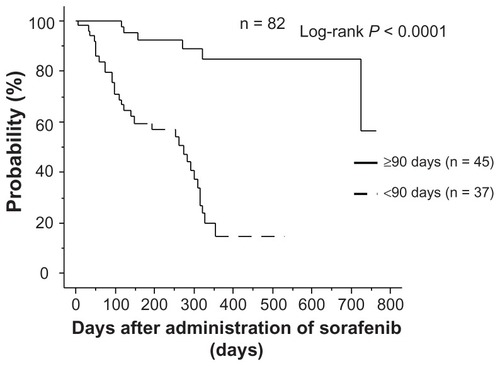
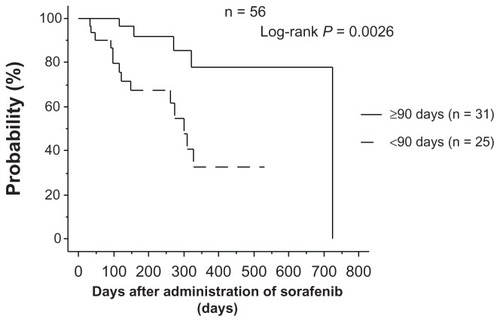
Figure 3 Relationship between continuation of administration and overall survival in patients receiving 200 mg or 400 mg.
Note: In the group that continued administration for ≥90 days, overall survival was significantly higher than in the group who discontinued administration within 90 days. and 3). Therefore, we concluded that treatment with sorafenib for ≥90 days achieves better overall survival, even at a reduced dose.
Compliance with treatment
The mean sorafenib dose was 800 mg in 26 patients (27%), 600 mg in nine (9%), 400 mg in 46 (48%), and ≤200 mg in 15 (16%). Because the median duration of treatment was 87 (range 2–737) days, we divided the patients into two groups, ie, one with ≥90 days of treatment with sorafenib (n = 45) and another within 90 days of treatment with sorafenib (n = 51), and examined factors influencing the patient’s ability to take the drug on a longer-term basis (). Common reasons for discontinuation within 90 days were adverse events (40 patients) and radiologic progression (n = 11). The adverse events were hand-foot skin reactions (n = 3), diarrhea (n = 3), general fatigue (n = 2), rash (n = 3), fever (n = 3), renal failure (n = 2), pancreatitis (n = 1), liver dysfunction (n = 15), and others (n = 8), whereas severe liver dysfunction included liver failure (n = 7), hepatic encephalopathy (n = 3), ascites (n = 3), elevation of aspartate or alanine aminotransferase (n = 1), and jaundice (n = 1).
Table 2 Reasons for discontinuation of sorafenib within 90 days
Prognostic factors for overall survival by univariate and multivariate analysis
On univariate analysis, BCLC (C) staging (P = 0.04), tumor volume ≥ 50% of the liver (P < 0.0001), macroscopic vascular invasion (P = 0.006), and discontinuation of sorafenib administration within 90 days (P < 0.0001) were significant prognostic factors, but only discontinuation of sorafenib within 90 days was identified as an independent prognostic factor contributing to overall survival on multivariate analysis (P < 0.0001, ).
Table 3 Risk factors contributing to overall survival (n = 96)
Relationship between administration for ≥90 days and overall survival
In the group that continued on sorafenib for ≥90 days, overall survival was significantly longer than in the group that discontinued sorafenib within 90 days (P < 0.0001), and the same relationship was found in the 61 patients who had their dose reduced to 400 mg and 200 mg (P = 0.0026,
Risk factors for discontinuation of sorafenib within 90 days by univariate and multivariate analysis
To identify risk factors for discontinuation of sorafenib within 90 days, patients whose observed periods were less than 90 days were eliminated. The total number was 82, with 45 being ≥90 days and 37 being <90 days (). On univariate analysis, des-gamma-carboxy prothrombin (≤400 mAU/mL, P = 0.04), tumor volume ≥ 50% of the liver (P = 0.02), macroscopic vascular invasion (P = 0.03), and six or more transarterial chemoembolizations (P = 0.02) were significant factors, and tumor volume ≥ 50% of the liver (P = 0.04) and six or more transarterial chemoembolizations (P = 0.013) were identified as independent risk factors on multivariate analysis.
Table 4 Risk factors contributing to discontinuation of sorafenib administration within 90 days (n = 82)
Discussion
Sorafenib is considered a drug that should be used for advanced hepatocellular carcinoma, but there are no suitable criteria for treatment of hepatocellular carcinoma at this stage, because the treatment outcomes are affected by multiple variables, including liver function, patient performance status, and tumor stage.Citation25,Citation26 Many trials have reported on the use of sorafenib to prevent hepatocellular carcinoma recurrence after treatment.Citation27 Sorafenib is used with sirolimus or with inhibitors of mammalian target of rapamycinCitation29 to reduce the risk of recurrence of hepatocellular carcinoma after liver transplantation,Citation28 and it has been reported that such combination therapy can be effective. Some adjuvant therapy studies after curative treatment for hepatocellular carcinoma, such as the STORM (Sorafenib as adjuvant Treatment in the prevention Of Recurrence of hepatocellular carcinoMa) trial, are ongoing,Citation27 and concurrent treatment of hepatocellular carcinoma with conventional transarterial chemoembolization and sorafenib has demonstrated a longer time to progression and possible efficacy.Citation30,Citation31 The overall median survival of our subjects was 11.8 months. Our data are slightly more robust than those of the Phase III SHARP (Sorafenib in Advanced Hepatocellular Carcinoma Assessment Randomized Protocol) trial (10.7 months)Citation20 and the tandem study in the Asia-Pacific region (6.5 months), probably because our study included a higher number of BCLC stage B patients than were included in the registration trials.Citation21
Sorafenib has several side effects and is often discontinued when their grade becomes severe. Multikinase inhibitors such as sorafenib have unique clinicopathologic consequences, including hand-foot skin reactions and severe side effects.Citation32–Citation34 The severity of hand-foot skin reactions is dose-related and depends on the duration, dosage, and accumulation of the drug.Citation35 Our data show that almost all patients had side effects, with about 40% of patients discontinuing sorafenib due to adverse events. However, some side effects may predict a response to sorafenib, such as early skin toxicity and diarrhea,Citation22,Citation36–Citation38 and methods have been reported for evaluating efficacy and overall survival.Citation39,Citation40 No studies have reported the efficacy of treatment dose or duration because the Phase III trial for sorafenib used only 800 mg.Citation20 Okuwaki et al reported late-onset progressive disease, indicating that prolonged treatment with sorafenib may be beneficial.Citation41 In our data, several factors in univariate analysis, such as BCLC stage C, tumor volume ≥ 50% of the liver, macroscopic vascular invasion, and discontinuation of sorafenib within 90 days reduced overall survival, but discontinuation of sorafenib within 90 days was the only factor found to reduce overall survival in multivariate analysis. Patients able to take sorafenib for longer than 90 days had better overall survival than those who discontinued within 90 days, even if they could take only 400 mg or less than 400 mg because of side effects. Our data demonstrate the benefit of a long duration of treatment, even in cases of reduced dosage. Interestingly, upon further investigation of patients who could be observed for 90 days or more, multivariate analysis showed that a tumor volume occupying ≥50% of the liver and six or more transarterial chemoembolization procedures prior to initiation of sorafenib were significant prognostic indicators. Our data indicate that prolonged administration is an important factor in obtaining good overall survival, and is better started when the number of transarterial chemoembolizations is less than six. Many transarterial chemoembolization procedures can worsen liver function and, although the Child-Pugh score does not change, there might be latent liver damage.
Sorafenib is indicated for patients with BCLC stage C and transarterial chemoembolization is recommended for patients with BCLC stage B,Citation7,Citation42 so sorafenib is usually used in patients whose tumors are progressing despite locoregional therapy. We recommend starting sorafenib before latent liver damage has occurred as a result of too many transarterial chemoembolization procedures, and prolonged administration of sorafenib is important for long overall survival, even if the dose of sorafenib needs to be reduced because of side effects.
Disclosure
The authors declare that they do not have anything to disclose regarding funding or conflicts of interest with respect to this manuscript.
References
- BruixJLlovetJMPrognostic prediction and treatment strategy in hepatocellular carcinomaHepatology20023551952411870363
- ParkKWParkJWChoiJISurvival analysis of 904 patients with hepatocellular carcinoma in a hepatitis B virus-endemic areaJ Gastroenterol Hepatol20082346747317764529
- MazzaferroVRegaliaEDociRLiver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosisN Engl J Med19963346936998594428
- LlovetJMRealMIMontanaXArterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trialLancet20023591734173912049862
- LoCMNganHTsoWKRandomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinomaHepatology2002351164117111981766
- VarelaMRealMIBurrelMChemoembolization of hepatocellular carcinoma with drug eluting beads: efficacy and doxorubicin pharmacokineticsJ Hepatol20074647448117239480
- BruixJShermanMManagement of hepatocellular carcinoma: an updateHepatology2011531020102221374666
- ShiratoriYShiinaSTerataniTInterferon therapy after tumor ablation improves prognosis in patients with hepatocellular carcinoma associated with hepatitis C virusAnn Intern Med200313829930612585827
- MutoYMoriwakiHNinomiyaMPrevention of second primary tumors by an acyclic retinoid, polyprenoic acid, in patients with hepatocellular carcinoma. Hepatoma Prevention Study GroupN Engl J Med1996334156115678628336
- MutoYSatoSWatanabeAOverweight and obesity increase the risk for liver cancer in patients with liver cirrhosis and long-term oral supplementation with branched-chain amino acid granules inhibits liver carcinogenesis in heavier patients with liver cirrhosisHepatol Res20063520421416737844
- SemelaDPiguetACKolevMVascular remodeling and anti-tumoral effects of mTOR inhibition in a rat model of hepatocellular carcinomaJ Hepatol20074684084817321636
- DempkeWCZippelRBrivanib. A novel dual VEGF-R2/bFGF-R inhibitorAnticancer Res2010304477448321115896
- HuynhHMolecularly targeted therapy in hepatocellular carcinomaBiochem Pharmacol20108055056020371362
- KudoMHepatocellular carcinoma 2009 and beyond: from the surveillance to molecular targeted therapyOncology200875 Suppl 111219092266
- VillanuevaALlovetJMTargeted therapies for hepatocellular carcinomaGastroenterology20111401410142621406195
- WilhelmSMCarterCTangLBAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesisCancer Res2004647099710915466206
- ChangYSAdnaneJTrailPASorafenib (BAY 43-9006) inhibits tumor growth and vascularization and induces tumor apoptosis and hypoxia in RCC xenograft modelsCancer Chemother Pharmacol20075956157417160391
- CoriatRNiccoCChereauCSorafenib-induced hepatocellular carcinoma cell death depends on reactive oxygen species production in vitro and in vivoMol Cancer Ther2012112284229322902857
- WilhelmSMAdnaneLNewellPPreclinical overview of sorafenib, a multikinase inhibitor that targets both Raf and VEGF and PDGF receptor tyrosine kinase signalingMol Cancer Ther200873129314018852116
- LlovetJMRicciSMazzaferroVSorafenib in advanced hepatocellular carcinomaN Engl J Med200835937839018650514
- ChengALKangYKChenZEfficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trialLancet Oncol200910253419095497
- OtsukaTEguchiYKawazoeSSkin toxicities and survival in advanced hepatocellular carcinoma patients treated with sorafenibHepatol Res20124287988622469363
- LencioniRLlovetJMModified RECIST (mRECIST) assessment for hepatocellular carcinomaSemin Liver Dis201030526020175033
- ShimJHParkJWChoiJIPractical efficacy of sorafenib monotherapy for advanced hepatocellular carcinoma patients in a Hepatitis B virus-endemic areaJ Cancer Res Clin Oncol200913561762518846384
- HanKHKudoMYeSLAsian consensus workshop report: expert consensus guideline for the management of intermediate and advanced hepatocellular carcinoma in AsiaOncology201181 Suppl 115816422212951
- LlovetJMDi BisceglieAMBruixJDesign and endpoints of clinical trials in hepatocellular carcinomaJ Natl Cancer Inst200810069871118477802
- KudoMAdjuvant therapy after curative treatment for hepatocellular carcinomaOncology201181 Suppl 1505522212936
- WeinmannANiederleIMKochSSorafenib for recurrence of hepatocellular carcinoma after liver transplantationDig Liver Dis20124443243722265328
- Gomez-MartinCBustamanteJCastroagudinJFEfficacy and safety of sorafenib in combination with mammalian target of rapamycin inhibitors for recurrent hepatocellular carcinoma after liver transplantationLiver Transpl201218455221932373
- SansonnoDLaulettaGRussiSTransarterial chemoembolization plus sorafenib: a sequential therapeutic scheme for HCV-related intermediate-stage hepatocellular carcinoma: a randomized clinical trialOncologist20121735936622334456
- ParkJWKohYHKimHBPhase II study of concurrent transarterial chemoembolization and sorafenib in patients with unresectable hepatocellular carcinomaJ Hepatol2012561336134222314421
- LacoutureMEReillyLMGeramiPHand foot skin reaction in cancer patients treated with the multikinase inhibitors sorafenib and sunitinibAnn Oncol2008191955196118550575
- LacoutureMEWuSRobertCEvolving strategies for the management of hand-foot skin reaction associated with the multitargeted kinase inhibitors sorafenib and sunitinibOncologist2008131001101118779536
- RombolaFCaravettaAMolloFSorafenib, risk of bleeding and spontaneous rupture of hepatocellular carcinoma. A clinical caseActa Medica (Hradec Kralove)20115417717922283115
- Boudou-RouquettePRopertSMirOVariability of sorafenib toxicity and exposure over time: a pharmacokinetic/pharmacodynamic analysisOncologist2012171204121222752067
- VincenziBSantiniDRussoAEarly skin toxicity as a predictive factor for tumor control in hepatocellular carcinoma patients treated with sorafenibOncologist201015859220051477
- BettingerDSchultheissMKnuppelEDiarrhea predicts a positive response to sorafenib in patients with advanced hepatocellular carcinomaHepatology20125678979022307848
- ZhaoYYangMQiXDrug-related adverse events may predict efficacy in sorafenib therapy for hepatocellular carcinomaHepatology20125679079122307917
- HorgerMLauerUMSchramlCEarly MRI response monitoring of patients with advanced hepatocellular carcinoma under treatment with the multikinase inhibitor sorafenibBMC Cancer2009920819558720
- LeeJHParkJYKim doYPrognostic value of 18F-FDG PET for hepatocellular carcinoma patients treated with sorafenibLiver Int2011311144114921745288
- OkuwakiYNakazawaTHidakaHLate-onset benefit in progressive advanced hepatocellular carcinoma with continued sorafenib therapy: a case reportJ Med Case Rep201263822280970
- EASL-EORTC clinical practice guidelines: management of hepatocellular carcinomaJ Hepatol20125690894322424438