

Abstract
Background and objective
Large clinical trials have confirmed the long-term efficacy of inhaled corticosteroid/long-acting β2-agonist combinations in patients with chronic obstructive pulmonary disease (COPD). It was hypothesized that significant treatment effects would already be present within 3 months after the initiation of treatment across a range of clinical outcomes, irrespective of COPD severity.
Methods
Post hoc analysis of 3-month post-randomization outcomes, including exacerbation rates, dropouts, symptoms, reliever use, and lung function, from three studies with similar inclusion criteria of moderate-to-very-severe COPD. Patients (n=1,571) were treated with budesonide/formoterol (B/F) 320/9 μg or placebo, twice daily; in one study, tiotropium 18 μg once daily was also given.
Results
Over the first 3 months of treatment, fewer patients randomized to B/F experienced exacerbations versus the placebo group (111 and 196 patients with ≥1 exacerbation, respectively). This was true in each COPD severity group. Compared with placebo, B/F treatment led to significantly lower 3-month exacerbation rates in the moderate and severe COPD severity groups (46% and 57% reduction, respectively), with a nonsignificant reduction (29%) in very severe COPD. Fewer dropouts occurred among patients treated with B/F versus placebo, this effect being greater with increasing COPD severity. B/F was associated with improved forced expiratory volume in 1 s, morning peak expiratory flow rate, total reliever use, and total symptom score versus placebo.
Conclusion
Treatment with B/F decreased exacerbations in patients with moderate-to-very-severe COPD within 3 months of commencing treatment. This effect was paralleled by improved lung function, less reliever medication use, and fewer symptoms, irrespective of disease severity.
Supplementary materials
Figure S1 Proportion of patients with moderate-to-very-severe COPD who received B/F or placebo and who had zero, 1, 2, or ≥3 exacerbations over the 3-month study period.
Abbreviations: B/F, budesonide/formoterol; COPD, chronic obstructive pulmonary disease.
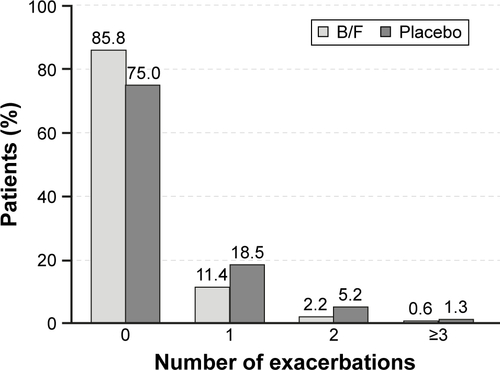
Table S2 Patient demographics and baseline clinical characteristics, by study
References
- SzafranskiWCukierARamirezAEfficacy and safety of budesonide/formoterol in the management of chronic obstructive pulmonary diseaseEur Respir J2003211748112570112
- CalverleyPMBoonsawatWCsekeZZhongNPetersonSOlssonHMaintenance therapy with budesonide and formoterol in chronic obstructive pulmonary diseaseEur RespirJ200322691291914680078
- JenkinsCRJonesPWCalverleyPMEfficacy of salmeterol/fluticasone propionate by GOLD stage of chronic obstructive pulmonary disease: analysis from the randomised, placebo-controlled TORCH studyRespir Res2009105919566934
- WelteTMiravitllesMHernandezPEfficacy and tolerability of budesonide/formoterol added to tiotropium in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2009180874175019644045
Acknowledgments
The authors would like to thank Thomas Similowski and Ian Naya for their contributions to this manuscript. We also thank Katharine Williams and Ash Dunne of inScience Communications, Springer Healthcare, who provided medical writing support funded by AstraZeneca. The sponsor (AstraZeneca) funded this analysis and was involved in the analysis, design, and interpretation of the data, always in conjunction with the authors. The University of Groningen has received money for research by unrestricted educational grants from AstraZeneca and Chiesi. AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and Nycomed have provided support for travel to meetings.
The current address of Anders Persson is Centre of Registers, Västra Götaland, Sweden.
Author contributions
PMC, GE, CRJ, ARA, BJM, AP, MF, and DSP all contributed to the conception, writing, and revision of the manuscript, and approved the final version for submission. AP was responsible for statistical analyses. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
PMC is a board member for Boehringer Ingelheim, the Department of Health Respiratory Programme Board, GlaxoSmithKline, and Nycomed. He has been a consultant for Novartis and provided expert testimony for Forest. PMC has received honoraria for advising on the conduct and analysis of clinical trial data from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Nycomed. He has also spoken at meetings supported by these companies. Support for travel to meetings has been provided by AstraZeneca.
GE is an ex-employee of AstraZeneca. He has consulted for Airsonett, ALK and Novartis, participated in advisory board meeting with Almirall, and is a member of the Medicon Village Inhalation Centre (MVIC).
CRJ is an advisory board member for AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Novartis, and a consultant for AstraZeneca, GlaxoSmithKline, Pieris, and Chiesi. Educational presentations have been developed for AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Novartis, with honoraria paid to CRJ or her institution. Lectures have been presented on behalf of AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Novartis. Support for travel to meetings has been provided by AstraZeneca and Boehringer Ingelheim.
ARA is a consultant and speaker for AstraZeneca, Bayer Pharma, Boehringer Ingelheim, Dey Pharma, GlaxoSmithKline, and Pfizer, and has received honoraria from these companies. Educational presentations have been developed for AstraZeneca, Bayer Pharma, Boehringer Ingelheim, Dey Pharma, GSK, and Pfizer. The University of Texas Health Science Center at San Antonio has received money for research to perform clinical trials. Support for travel to meetings has also been provided by AstraZeneca.
BJM is an advisory board member for Aerocrine, AstraZeneca, Forest, Boehringer Ingelheim, CSL Bering, Forest, Novartis, and Theravance and a consultant for Astellas, Forest, and Chiesi. Clinical trial data have been reviewed for Spiration, with grants received and controlled by National Jewish Health from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Forest, MedImmune, Nabi, National Institutes of Health, Pfizer, and Sunovian. Lectures have been presented on behalf of Boehringer Ingelheim and GlaxoSmithKline. Educational presentations and programs have been developed (Carden Jennings, Cleveland Clinic, Consensus Medical, Foundation for Improving Patient Outcomes, Hybrid Communications, Integrity, Intellisphere, Medscape, National Jewish Health, Projects in Knowledge, SPIRE, Synapse, and WebMD). Royalties have been received from Up-To-Date. BJM has been a speaker for educational programs at Abbott, the American Academy of Family Practice, the American College of Chest Physicians, and the American Thoracic Society. Support for travel to meetings has also been provided by AstraZeneca.
AP and MF are employees of AstraZeneca and own stocks within the company.
The University of Groningen has received honoraria for DSP advising on the conduct and analysis of clinical trial data from AstraZeneca, Nycomed, and Teva, as well as for lectures at meetings supported by AstraZeneca, Chiesi, GlaxoSmithKline, Nycomed, and Teva.