

Abstract
Background
Patients with COPD may be prescribed multiple inhalers as part of their treatment regimen, which require different inhalation techniques. Previous literature has shown that the effectiveness of inhaled treatment can be adversely affected by incorrect inhaler technique. Prescribing a range of device types could worsen this problem, leading to poorer outcomes in COPD patients, but the impact is not yet known.
Aims
To compare clinical outcomes of COPD patients who use devices requiring similar inhalation technique with those who use devices with mixed techniques.
Methods
A matched cohort design was used, with 2 years of data from the Optimum Patient Care Research Database. Matching variables were established from a baseline year of follow-up data, and two cohorts were formed: a “similar-devices cohort” and a “mixed-devices cohort”. COPD-related events were recorded during an outcome year of follow-up. The primary outcome measure was an incidence rate ratio (IRR) comparing the rate of exacerbations between study cohorts. A secondary outcome compared average daily use of short-acting beta agonist (SABA).
Results
The final study sample contained 8,225 patients in each cohort (mean age 67 [SD, 10], 57% males, 37% current smokers). Patients in the similar-devices cohort had a lower rate of exacerbations compared with those in the mixed-devices cohort (adjusted IRR 0.82, 95% confidence interval [CI] 0.80–0.84) and were less likely to be in a higher-dose SABA group (adjusted proportional odds ratio 0.54, 95% CI 0.51–0.57).
Conclusion
COPD patients who were prescribed one or more additional inhaler devices requiring similar inhalation techniques to their previous device(s) showed better outcomes than those who were prescribed devices requiring different techniques.
Supplementary materials
Figure S1 Effect of similar versus mixed devices on primary and secondary COPD outcomes – alternative categorization of devices.
Notes: aIRR adjusted by COPD consultations, use of antibiotics, statins and paracetamol. OR adjusted by SABA dosage, use of statins, beta-blockers and paracetamol. n=7,545 in each cohort, for this categorization of devices.
Abbreviations: CI, confidence interval; SABA, short-acting beta agonist.
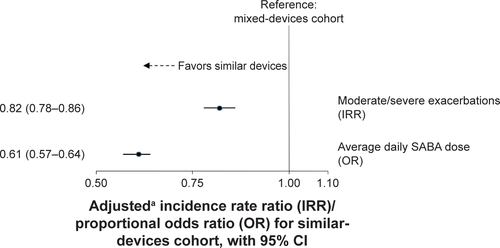
Figure S2 Effect of similar versus mixed devices on primary and secondary COPD outcomes – largest treatment combination subgroup.
Notes: aIRR adjusted by antibiotics courses, asthma diagnosis and use of paracetamol. OR adjusted by SABA dosage, use of statins, beta-blockers and paracetamol. n=3,680 (44.7%) in similar-devices cohort and n=2,859 (34.8%) in mixed-devices cohort.
Abbreviations: CI, confidence interval; SABA, short-acting beta agonist.
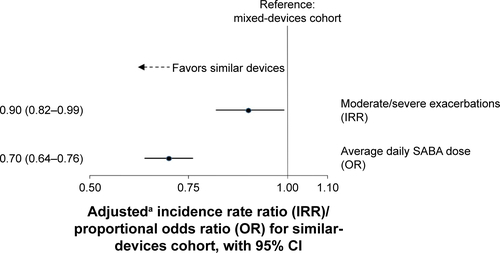
Figure S3 Effect of similar versus mixed devices on primary and secondary COPD outcomes – alternative categorization of devices and largest treatment combination subgroup.
Notes: aIRR adjusted by antibiotics courses, asthma diagnosis and use of paracetamol. OR adjusted by SABA dosage, use of statins, beta-blockers and paracetamol. n=3,762 (49.9%) in similar-devices cohort and n=2,577 (34.2%) in mixed-devices cohort.
Abbreviations: CI, confidence interval; SABA, short-acting beta agonist.
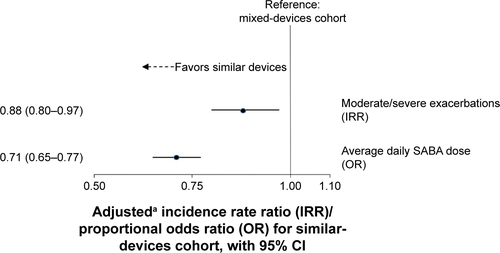
Table S1 Comorbidities, baseline co-medications and COPD classifications in each study cohort
Table S2 Combinations of COPD therapy during baseline year in each study cohort
Table S3 Combinations of COPD therapy during outcome year in each study cohort
Acknowledgments
This study was funded by Teva Pharmaceutical Industries Ltd. The authors would like to thank Lisa Law and Simon van Rysewyck for medical writing and Arjun Jain for statistical analysis. Many thanks to Derek Skinner for preparation of data for analysis.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
SBA has no shares in any pharmaceutical companies. She has received sponsorship to carry out studies, together with Board Membership, consultant agreements and honoraria for presentation, from several pharmaceutical companies that market inhaled products. These include AstraZeneca, GlaxoSmithKline, Meda, Mundipharma and Teva.
HC has no shares in any pharmaceutical companies. He has received sponsorship to carry out studies, together with Board Membership, consultant agreements and honoraria for presentation, from several pharmaceutical companies that market inhaled products. These include Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Innovata Biomed, Meda, Napp Pharmaceuticals, Mundipharma, NorPharma, Norvartis, Orion, Sanofi, Teva, Truddell Medical International, UCB and Zentiva. Research sponsorship has also been received from grant awarding bodies (EPSRC and MRC). He is the owner of Inhalation Consultancy Ltd. He is also an employee of Research in Real Life Ltd, which conducted this study and which has conducted paid research in respiratory disease on behalf of the following other organizations in the past 5 years: Aerocrine, AKL Ltd, Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Meda, Mundipharma, Napp, Novartis, Orion, Takeda, Teva, and Zentiva, a Sanofi company.
RC has a patent on an audio-based technology to assess response to inhaled medication. He currently has grants from GSK and Aerogen and receives speaker and Advertisement board fees from GSK Novartis, Boehringer and TEVA.
FL has no shares in any pharmaceutical companies. FL reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla and Teva Pharmaceuticals. FL has board membership with Boehringer Ingelheim, Chiesi, Teva Pharmaceuticals. RRR reports grants and personal fees from Almirall, AstraZeneca, Boehringer Ingelheim, Ferrer Group, Mylan, Novartis, Pearl Therapeutics, Takeda, and TEVA and grants and personal fees from Menarini during the conduct of the study. He is member of the GOLD Board of Directors and of the Scientific Committee.
SY is employed by Observational and Pragmatic Research Institute Pte Ltd, which receives funding from UK National Health Service, British Lung Foundation, Aerocrine, AKL Ltd, Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Eli Lilly, GlaxoSmithKline, Meda, Merck, Mundipharma, Napp, Novartis, Orion, Pfizer, Respiratory Effectiveness Group, Takeda, Teva Pharmaceuticals and Zentiva.
DP has board membership with Aerocrine, Almirall, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Meda, Mundipharma, Napp, Novartis and Teva Pharmaceuticals; consultancy with Almirall, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Meda, Mundipharma, Napp, Novartis, Pfizer and Teva Pharmaceuticals; grants and unrestricted funding for investigator-initiated studies (conducted through Research in Real-Life Ltd, which is subcontracted by Observational and Pragmatic Research Institute Pte Ltd, and OPRI) from UK National Health Service, British Lung Foundation, Aerocrine, AKL Ltd, Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Eli Lilly, GlaxoSmithKline, Meda, Merck, Mundipharma, Napp, Novartis, Orion, Pfizer, Respiratory Effectiveness Group, Takeda, Teva Pharmaceuticals and Zentiva; payments for lectures/speaking from Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Meda, Merck, Mundipharma, Novartis, Pfizer, Skyepharma, Takeda and Teva Pharmaceuticals; payment for manuscript preparation from Mundipharma and Teva Pharmaceuticals; patents (planned, pending or issued) from AKL Ltd; payment for the development of educational materials from GlaxoSmithKline and Novartis; stock/stock options from AKL Ltd which produces phytopharmaceuticals; owns 80% of Research in Real Life Ltd, which is subcontracted by OPRI, 75% of the social enterprise Optimum Patient Care Ltd and 75% of OPRI; received payment for travel/accommodations/meeting expenses from Aerocrine, Boehringer Ingelheim, Mundipharma, Napp, Novartis and Teva Pharmaceuticals; funding for patient enrolment or completion of research from Almirral, Chiesi, Teva Pharmaceuticals and Zentiva; and peer reviewer for grant committees of the Medical Research Council (2014), Efficacy and Mechanism Evaluation programme (2012), HTA (2014).
The other authors report no conflicts of interest in this work.