Abstract
Introduction
High-intensity noninvasive ventilation (NIV) has been shown to improve outcomes in stable chronic obstructive pulmonary disease patients. However, there is insufficient knowledge about whether with this more controlled ventilatory mode optimal respiratory muscle unloading is provided without an increase in patient–ventilator asynchrony (PVA).
Patients and methods
Ten chronic obstructive pulmonary disease patients on home mechanical ventilation were included. Four different ventilatory settings were investigated in each patient in random order, each for 15 min, varying the inspiratory positive airway pressure and backup breathing frequency. With surface electromyography (EMG), activities of the intercostal muscles, diaphragm, and scalene muscles were determined. Furthermore, pressure tracings were derived simultaneously in order to assess PVA.
Results
Compared to spontaneous breathing, the most pronounced decrease in EMG activity was achieved with the high-pressure settings. Adding a high breathing frequency did reduce EMG activity per breath, while the decrease in EMG activity over 1 min was comparable with the high-pressure, low-frequency setting. With high backup breathing frequencies less breaths were pressure supported (25% vs 97%). PVAs occurred more frequently with the low-frequency settings (P=0.017).
Conclusion
High-intensity NIV might provide optimal unloading of respiratory muscles, without undue increases in PVA.
Disclosure
MLD is the recipient of an European Respiratory Society Long-term Fellowship (LTRF 2014-3126). LAvE did assist with the measurements; however, his company (Inbiolab B.V.) did not have any influence on the design, conduction, or final analyses on the study. PJW has received a research grant and personal speaking fees from Philips/Respironics, the Netherlands. The other authors report no conflicts of interest in this work.
Supplementary materials
Methods
EMG data acquisition and preprocessing
Electrical heart activity, which interferes with diaphragm electromyography (EMG) signals, was removed according to the process described in Figure S1.
Control of breathing and patient–ventilator asynchrony
Control of the breaths and triggering Pressure-supported breath (Figure S2)
Pressure-supported (PS) breaths are breaths delivered by the ventilator following a trigger from the patient. By definition, a PS breath was counted once the diaphragm and/or intercostal EMG signal preceded the onset of the pressure wave.
Pressure-controlled breath (Figure S3)
Pressure-controlled (PC) breaths are breaths delivered by the ventilator without a trigger from the patient. By definition, a PC breath was counted once the diaphragm and/or intercostal EMG signal followed the onset of the pressure wave or was totally abolished.
Patient–ventilator asynchrony
We counted the following patient–ventilator asynchrony (PVAs): ineffective efforts (Figure S4); autotriggering (Figure S5); double or multiple triggering (Figure S6); and cycling asynchronies (premature [Figure S7] and delayed cycling [Figure S8]).
Figure S1 The QRS removal process.
Notes: The averaged EMG (EMGa) shows respiratory activity. As control the signal from the abdominal magnetometer band (Band) is shown. From the diaphragmatic EMG signal (EMGd), the QRS complex was detected and stretched into a standard QRS pulse with a duration of 100 ms (QRS). During the QRS pulse a cut was made in the slightly delayed (40 ms) EMG signal to completely filter out the QRS complex (EMGg). Next, the gated EMG was rectified and averaged with a moving time window of 200 ms. Finally, the missing signal in the gate was filled with the running average resulting in a fairly good interpolation during the gate and an almost QRS-free averaged EMG signal (EMGa).
Abbreviation: EMG, electromyography.
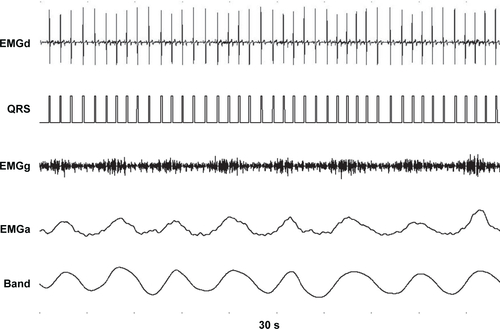
Figure S2 A pressure-supported (PS) breath.
Notes: Shown are (from top to bottom) the raw intercostal signal (Int raw), the raw frontal diaphragm signal (F Dia raw), the raw dorsal diaphragm signal (D Dia raw), the pressure wave (Paw), the average intercostal signal (Interc), the average frontal diaphragm (F Dia) signal, and the average dorsal diaphragm signal (D Dia). Two PS breaths are shown, as electromyography activity (the dotted red line) precedes the pressure wave (the straight blue line). A low backup frequency of 10 breaths/min was set on the ventilator, therefore a 2.6 s time in-between the breaths confirms that breaths were PS and not pressure-controlled (PC).
Abbreviation: EMG, electromyography.
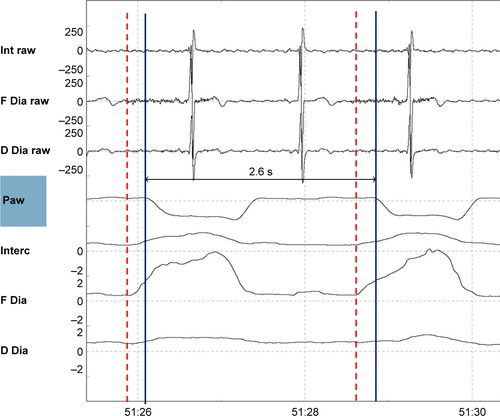
Figure S3 A pressure-controlled (PC) breath.
Notes: Shown are (from top to bottom) the raw intercostal signal (Int raw), the raw frontal diaphragm signal (F Dia raw), the raw dorsal diaphragm signal (D Dia raw), the pressure wave (Paw), the average intercostal signal (Interc), the average frontal diaphragm (F Dia) signal, and the average dorsal diaphragm signal (D Dia). Two PC breaths are shown, electromyography activity (the dotted red line) appears but after the pressure wave (the straight blue line) started. This is a tracing during a high-pressure, high-frequency setting, with a backup frequency of 22 breaths/min, so that an in-between breath time of 2.7 s means that the ventilator delivers a breath at the moment it is supposed to do according to the set-up backup frequency. Of note, electromyography activity was much lower with this setting.
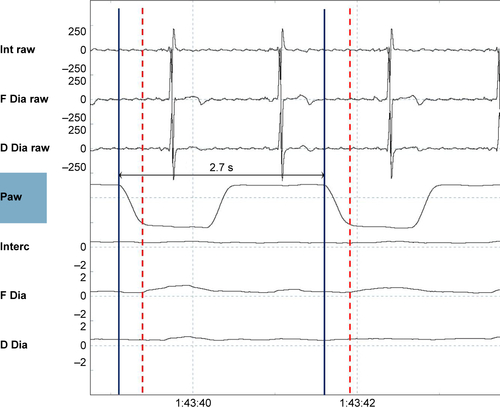
Figure S4 An ineffective effort.
Notes: Shown are (from top to bottom) the raw intercostal signal (Int raw), the raw frontal diaphragm signal (F Dia raw), the raw dorsal diaphragm signal (D Dia raw), the pressure wave (Paw), the average intercostal signal (Interc), the average frontal diaphragm (F Dia) signal, and the average dorsal diaphragm signal (D Dia). An electromyography signal (dotted red line) was not followed by a breath delivered by the ventilator (straight arrow blue line).
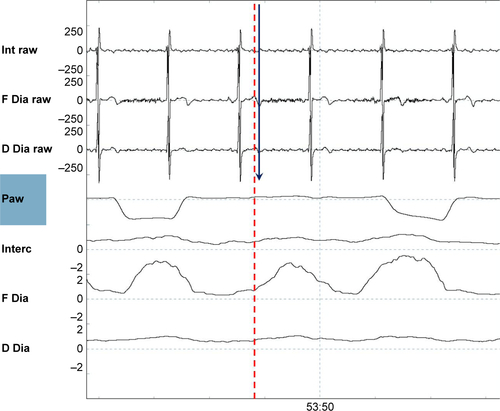
Figure S5 Autotriggering.
Notes: Shown are (from top to bottom) the raw intercostal signal (Int raw), the raw frontal diaphragm signal (F Dia raw), the raw dorsal diaphragm signal (D Dia raw), the pressure wave (Paw), the average intercostal signal (Interc), the average frontal diaphragm (F Dia) signal, and the average dorsal diaphragm signal (D Dia). During this low-frequency setting (backup frequency 10 breaths/min), the two breaths denoted by arrows come too soon to be PC. As it is not preceded by EMG activity, these are defined as inappropriate autotriggered breaths (straight blue lines).
Abbreviations: EMG, electromyography; PC, pressure-controlled.
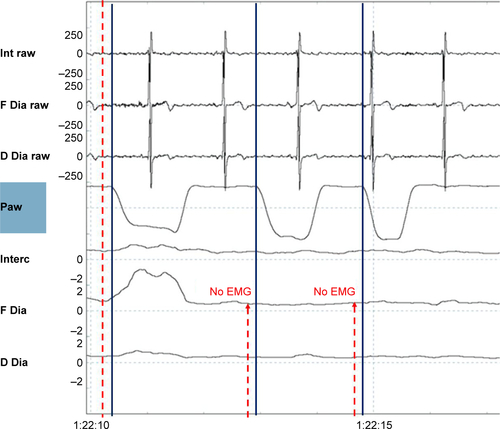
Figure S6 Double triggering.
Notes: Shown are (from top to bottom) the raw intercostal signal (Int raw), the raw frontal diaphragm signal (F Dia raw), the raw dorsal diaphragm signal (D Dia raw), the pressure wave (Paw), the average intercostal signal (Interc), the average frontal diaphragm (F Dia) signal, and the average dorsal diaphragm signal (D Dia). A single electromyography wave (dotted red line) is followed by two ventilator delivered breaths (nr.1 and nr.2 straight blue lines).
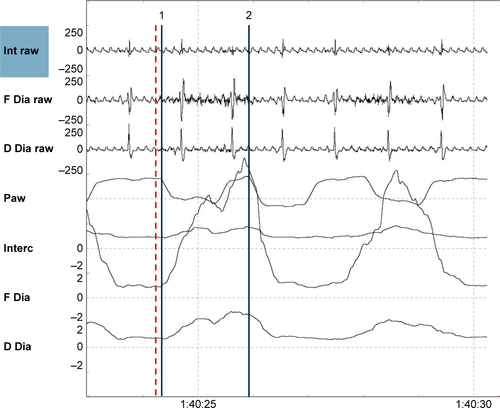
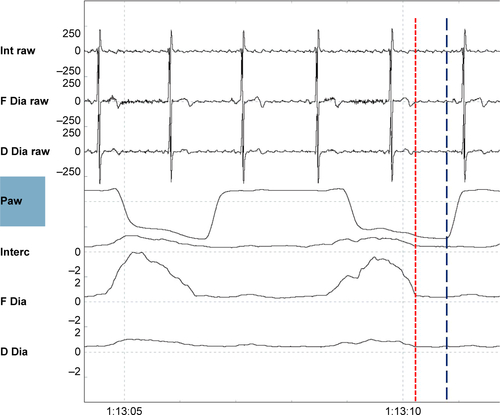
Figure S7 Premature cycling.
Notes: Shown are (from top to bottom) the raw intercostal signal (Int raw), the raw frontal diaphragm signal (F Dia raw), the raw dorsal diaphragm signal (D Dia raw), the pressure wave (Paw), the average intercostal signal (Interc), the average frontal diaphragm (F Dia) signal, and the average dorsal diaphragm signal (D Dia). Electromyography activity (the maximum of the electromyography is depicted by the red dotted line) continues, while the pressure returns to baseline again (the end of the inspiratory pressure delivering is depicted by the blue dotted line).
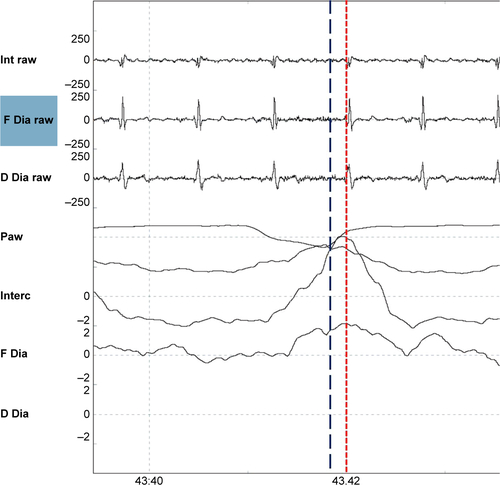
Figure S8 Delayed cycling.
Notes: Shown are (from top to bottom) the raw intercostal signal (Int raw), the raw frontal diaphragm signal (F Dia raw), the raw dorsal diaphragm signal (D Dia raw), the pressure wave (Paw), the average intercostal signal (Interc), the average frontal diaphragm (F Dia) signal, and the average dorsal diaphragm signal (D Dia). The electromyography activity has already ceased (end of the electromyography activity depicted by the red dotted line), while the pressure wave continues, (end of the breaths depicted by the straight blue line).