
Abstract
Background
The FLAME study demonstrated that indacaterol/glycopyrronium (IND/GLY), the fixed-dose combination of a long-acting β2-agonist (LABA, IND) and a long-acting muscarinic antagonist (LAMA, GLY), was superior to salmeterol/fluticasone combination (SFC) in preventing exacerbations in COPD patients with a high risk of exacerbations. In this study, we report a prespecified analysis of the efficacy and safety of IND/GLY versus SFC in Asian patients from the FLAME study.
Patients and methods
Patients from Asian centers with moderate-to-very severe COPD and ≥1 exacerbation in the previous year from the 52-week, randomized FLAME study were included. IND/GLY was compared versus SFC for effects on exacerbations, lung function (forced expiratory volume in 1 second [FEV1] and forced vital capacity [FVC]), health status (St George’s Respiratory Questionnaire [SGRQ]), rescue medication use, and safety.
Results
A total of 510 Asian patients (IND/GLY, n=250 or SFC, n=260) were included. Compared to the overall FLAME population, the Asian cohort had more males, a shorter duration of COPD, fewer patients using inhaled corticosteroid (ICS) at screening, fewer current smokers, and more patients with very severe COPD. IND/GLY significantly reduced the rate of moderate/severe exacerbations (rate ratio: 0.75; 95% confidence interval: 0.58–0.97; P=0.027) and prolonged time to first moderate/severe exacerbation versus SFC (hazard ratio: 0.77; 95% confidence interval: 0.59–1.01; P=0.055). Predose trough FEV1 and FVC significantly improved in Asian patients (P<0.001). IND/GLY improved SGRQ for COPD (SGRQ-C score; P=0.006) and reduced rescue medication use (P=0.058) at week 52. Pneumonia incidence was 3.6% with IND/GLY and 7.7% with SFC (P=0.046).
Conclusion
In exacerbating Asian COPD patients, IND/GLY was more effective than SFC.
Introduction
COPD is a progressive disease characterized by partially reversible airflow limitation and poses a major health care and socioeconomic burden.Citation1–Citation4 Differences in disease prevalence and clinical practice for COPD exist between Asian and other populations, including higher rates of COPD-associated mortality and morbidity due to differences in exposure to tobacco use, environmental pollutants, health care management structure, and cultural differences.Citation5,Citation6 Patients with COPD are prone to experiencing exacerbations, which clinically manifest as an acute worsening of symptoms that is beyond normal day-to-day variations and leads to a change in the treatment regimen.Citation7 Exacerbations are a significant cause of morbidity, mortality, and increased health care costs.Citation8 Hence, prevention of exacerbations is important in the clinical management of COPD, and treatments that can prevent exacerbations would have beneficial effects on patients’ health status and disease outcomes.Citation9 Combination of LABA and ICS (LABA/ICS) or LAMA monotherapy has been recommended by most COPD treatment guidelines as the first choice of treatment for COPD patients with a high risk of exacerbation.Citation10,Citation11 However, LABA/ICS combination therapy is associated with an increased risk of pneumonia, along with other steroid-related adverse effects.Citation12,Citation13 A dual bronchodilator regimen of LABA/LAMA is an attractive alternative to the LABA/ICS combination in COPD patients at risk of exacerbations.Citation14 Prospective exploratory analyses showed for the first time in the LANTERN study that a fixed-dose combination of IND (a LABA) and GLY (a LAMA) was more effective in reducing exacerbations compared with SFC (a LABA/ICS) in patients with moderate-to-severe COPD.Citation15 In Asian patients, IND/GLY was shown to be superior over monobronchodilators in improving lung function, symptoms, and health status and reducing exacerbations without any safety concerns.Citation16 The recently reported subgroup analysis of the SHINE study demonstrated that IND/GLY showed superior efficacy and comparable safety compared with its monocomponents, open-label tiotropium, and placebo in Japanese patients with moderate-to-severe COPD.Citation17
The 52-week FLAME study was the first study to demonstrate that IND/GLY was superior to SFC in reducing the risk of exacerbations in patients with moderate-to-very severe COPD with a high exacerbation risk.Citation18 The FLAME study provided an opportunity to assess the efficacy of IND/GLY in COPD patients from different regions; the study included ~15% of patients from Asia. As ethnic differences between the Western and Asian population, including those in the pathogenesis of COPD and its natural course, genetic makeup, clinical practice, and pharmacogenomics could influence the relative efficacy and safety of available therapies, it is important to assess the efficacy and safety of new therapies specifically within this population. In this study, we present the results from a comprehensive analysis of the efficacy and safety of IND/GLY in Asian COPD patients from the FLAME study.
Patients and methods
Study design
This was a prespecified analysis of Asian patients from the multicenter, randomized, double-blind, double-dummy, parallel-group, noninferiority, active-controlled FLAME study.
Patients
The FLAME study enrolled male or female patients aged ≥40 years with stable COPD and moderate-to-very severe airflow limitation (GOLD 2011 criteria). Eligible patients had a postbronchodilator FEV1 ≥25% and <60% predicted and postbronchodilator FEV1/FVC <0.70 at the start of the run-in period. Patients were included if they had a documented history of ≥1 COPD exacerbation (that required treatment with systemic corticosteroids and/or antibiotics) in the previous 12 months and a dyspnea mMRC grade ≥2 at the start of the run-in period. Patients were excluded from the study if they had an exacerbation that required treatment with antibiotics and/or systemic corticosteroids and/or hospitalization in the 6 weeks prior to screening and during the run-in period; patients with a blood eosinophil count of >600/mm3 at the start of run-in were also excluded.
The study protocol and all amendments were reviewed and approved by the IEC or IRB for each center. For a full list of the ethics committees please view them here. This trial is registered at ClinicalTrials.gov (NCT1782326). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Written informed consent was obtained from all patients.
Treatments
Eligible patients were randomized (1:1) to receive either IND/GLY 110/50 µg q.d. or SFC 50/500 µg b.i.d. for 52 weeks, with a 30-day follow-up. At screening, patients were provided with a short-acting β2-agonist (salbutamol or albuterol) inhaler to use as rescue medication on an “as needed” basis throughout the study.
Study outcomes
Exacerbation end points
Efficacy of IND/GLY was compared with SFC, primarily in terms of rate of all (mild, moderate, or severe) COPD exacerbations (primary end point of the overall FLAME study), rate of moderate/severe COPD exacerbations, and time to first moderate/severe COPD exacerbation (secondary end points of the overall FLAME study). Exacerbations were defined as per the standard Anthonisen criteriaCitation19,Citation20 and were categorized as mild (worsening of symptoms for >2 consecutive days, not treated with systemic corticosteroids and/or antibiotics), moderate (requiring treatment with systemic corticosteroids or antibiotics or both), and severe (leading to patient hospitalization [emergency room visit of >24 hours considered as a hospitalization] in addition to treatment with systemic corticosteroids and/or antibiotics).
Other efficacy end points
Lung function (predose FEV1 and predose FVC after 4, 12, 26, 38, and 52 weeks of treatment), health status (SGRQ-C total score after 4, 12, 26, 38, and 52 weeks of treatment), and rescue medication use (number of puffs taken in the previous 12 hours recorded in the morning and evening by the patient using eDiary) were also assessed during 52 weeks of treatment.
Safety assessments
Safety assessments included incidence of treatment-emergent AEs, SAEs, AEs suspected to be related to study drug, deaths, and time to first pneumonia (consolidated term). All cases of pneumonia were confirmed by CXR.
Statistical analysis
The full analysis set and safety set included all randomized patients who received at least 1 dose of double-blind drug. The number of exacerbations during the 52-week treatment period was analyzed using a negative binomial model including terms for treatment, smoking status at baseline, ICS use at screening, baseline severity of airflow limitation, and region as fixed effects. The model also contained baseline total symptom score and number of exacerbations in the year prior to screening, as covariates. The time-to-event end points were analyzed using a Cox regression model that included the same terms as the negative binomial model. The primary noninferiority analysis was powered based on the overall sample size. This study was not designed to demonstrate noninferiority in any cohort, including the Asian cohort. A chi-square test was performed to assess whether there was a significant difference between IND/GLY and SFC in the pneumonia rate.
Results
Study population
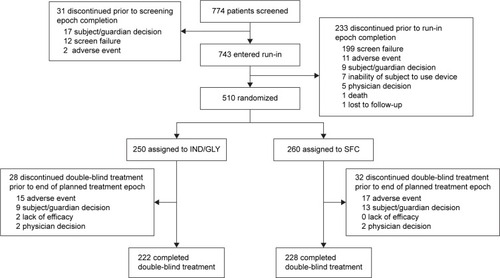
A total of 510 (IND/GLY, n=250; SFC, n=260) patients (295 from China, 5 from Hong Kong, 80 from Japan, 35 from The Philippines, 71 from Korea, 16 from Taiwan, and 8 from Thailand) were included in this analysis (Table S1), representing 15.2% of the overall FLAME study population. The rates of discontinuation from double-blind treatment were 11.2% versus 12.3% in the IND/GLY and SFC groups (). A total of 505 patients (IND/GLY, n=247; SFC, n=258) were included in the full analysis set.
Figure 1 Patient disposition of Asian cohort from the FLAME study.
Abbreviations: GLY, glycopyrronium; IND, indacaterol; SFC, salmeterol/fluticasone propionate combination.
Overall, the Asian cohort had a higher proportion of males, with a lower BMI, shorter duration of COPD, fewer patients who used ICS at screening, a lower percentage of current smokers, and a higher proportion of patients with very severe COPD compared with the overall population (). The majority of patients in the Asian cohort were in GOLD group D (77.8%), with moderate-to-very severe airflow limitation and a mean postbronchodilator FEV1 of 42.7% of the predicted normal value. A total of 18.6% of patients had a history of ≥2 moderate or severe exacerbations in the past year. Within the Asian cohort, there were no baseline imbalances in the proportion of patients who had a history of either 1 or 2 or more exacerbations in the previous year.
Table 1 Baseline patient demographics and clinical characteristics of the FLAME overall population and Asian cohort
Efficacy – COPD exacerbations
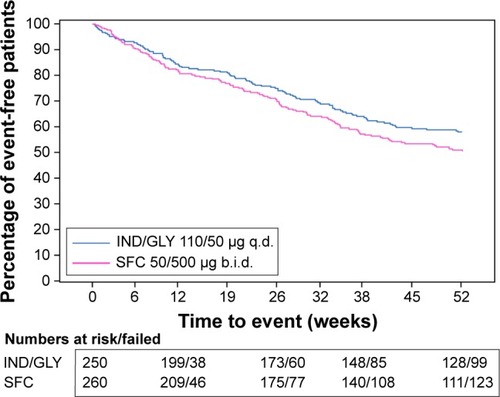
IND/GLY significantly reduced the rate of moderate or severe exacerbations (health care utilization) by 25% (RR, 0.75; 95% CI: 0.58–0.97; P=0.027; ) compared with SFC. The rate reduction with IND/GLY in the Asian cohort was comparable with that observed in the overall population (17% reduction; ). Furthermore, the annualized rate of moderate or severe exacerbations was lower in the Asian cohort than in the overall population (Table S2). IND/GLY prolonged the time to first moderate or severe exacerbation with a 23% reduction in risk (180 days [95% CI, 135–223] versus 148 days [95% CI, 98–184]; HR, 0.77; 95% CI, 0.59–1.01; P=0.055; ) versus SFC, in line with the observations from the overall population (HR, 0.78; 95% CI, 0.70–0.86; P<0.001). Less than 50% of patients in both treatment groups had an exacerbation; therefore, time to first moderate or severe exacerbation in the first quartile of patients was calculated instead of the median time. IND/GLY reduced the annualized rate of all (mild, moderate, or severe) COPD exacerbations versus SFC (RR, 0.94; 95% CI: 0.76–1.16; P=0.567) in the full analysis set of the Asian population. The rate of all (mild, moderate, or severe) COPD exacerbations was lower with both treatments in the Asian cohort compared with the overall population (Table S3).
Figure 2 Rate of moderate or severe COPD exacerbations during 52 weeks of treatment (full analysis set).
Abbreviations: b.i.d., twice daily; CI, confidence interval; GLY, glycopyrronium; IND, indacaterol; q.d., once daily; RR, rate ratio; SFC, salmeterol/fluticasone propionate combination.
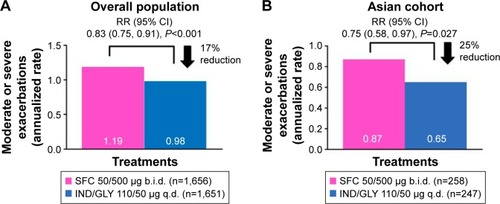
Figure 3 Kaplan–Meier plot of time to first moderate or severe COPD exacerbation during 52 weeks of treatment.
Efficacy – lung function
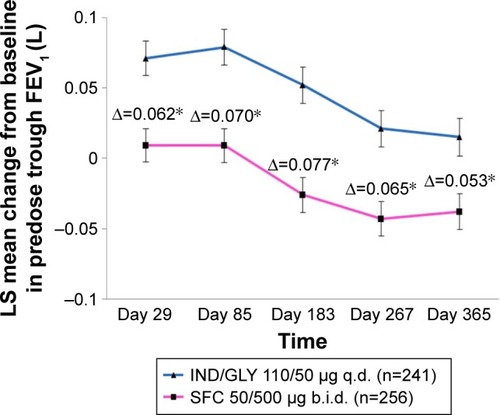
Improvement in predose trough FEV1 was significantly greater with IND/GLY versus SFC, with a treatment difference of 53 mL at week 52 (P<0.001). Treatment differences at all other time points were significant (P<0.001), and a clear separation was seen between the 2 treatments from day 29, which was sustained until day 365 (). Improvement in trough FVC at week 52 was also significantly greater with IND/GLY compared with SFC, with a treatment difference of 213 mL (P<0.001). Treatment differences at all other time points (weeks 4, 12, 26, and 38) were also significant (P<0.001).
Figure 4 Change from baseline in predose trough FEV1 (L) over treatment duration (full analysis set).
Abbreviations: b.i.d., twice daily; FEV1, forced expiratory volume in 1 second; GLY, glycopyrronium; IND, indacaterol; LS, least squares; q.d., once daily; SFC, salmeterol/fluticasone propionate combination.
Efficacy – health status
Improvement in SGRQ-C total score over the 52-week treatment period was greater with IND/GLY compared with SFC, with a treatment difference of -3.1 units at week 52 (P=0.006; Figure S1). IND/GLY showed a greater improvement in SGRQ-C score versus SFC at week 52 in the Asian cohort compared with that observed in the overall population (−1.3 units).
Efficacy – rescue medication use
Rescue medication use (puffs/day) was numerically reduced with IND/GLY versus SFC (treatment difference, −0.25; 95% CI: -0.50 to 0.01; P=0.058), and the change from baseline in percentage of rescue medication-free days was also numerically greater with IND/GLY compared with SFC (treatment difference, 2.7; 95% CI: −2.2 to 7.7; P=0.277).
Safety
The incidence of AEs was similar between the IND/GLY and SFC groups. COPD was the most frequently reported AE, and the incidence was similar between the 2 treatment groups (). The incidence of SAEs was numerically higher in the SFC group compared with the IND/GLY group. The number of patient deaths was comparable between the IND/GLY (n=4) and SFC (n=5) groups. The primary causes of deaths were cardiovascular and respiratory disorders. The incidence of pneumonia was numerically lower in the IND/GLY group compared with the SFC-treated patients (3.6 versus 7.7%; P=0.046), and this incidence was higher in the Asian cohort than in the overall study population (IND/GLY, 3.2%; SFC, 4.8%). Additionally, IND/GLY delayed the time to first pneumonia (using the consolidated term of pneumonia [preferred terms of pneumonia, lung infection and pneumonia bacterial]) compared with SFC (P=0.054). The incidence of other respiratory tract infections (including influenza) was numerically higher with SFC, as was the incidence of oral candidiasis (IND/GLY, 1.2%; SFC, 7.7%). The incidence of MACEs was low and comparable between the treatment groups (IND/GLY, 1.2%; SFC, 2.3%); the incidence of cardiovascular deaths was the same in the 2 groups (IND/GLY, 0.4%; SFC, 0.4%).
Table 2 AEs by preferred term (≥3% in any treatment group) and SAEs (safety set)
Discussion
Acute COPD exacerbations cause considerable morbidity and mortality and incur significant health care utilization and associated costs.Citation21,Citation22 In this context, global treatment guidelines for COPD do not recommend region-specific treatment options;Citation10 hence, regional guidelines draw heavily from the global guidelines for treatment recommendations. The great majority of data comparing therapeutic options has been generated in the Western population. Yet, Asian population differs from the Western population in disease reporting, socioeconomic factors as well as disease management practices; additionally, previous data suggest that disease manifestations may differ between these populations.Citation23 Therefore, evaluation of efficacy and safety of therapeutic options in COPD patients from Asia are of considerable clinical importance to validate the treatment effects seen globally.Citation24,Citation25
FLAME was the first study which compared the effect of LABA/LAMA (IND/GLY 110/50 µg q.d.) therapy versus LABA/ICS (SFC 50/500 µg b.i.d.) evaluating exacerbations as the primary end point in COPD patients with moderate-to-very severe airflow limitation and with a high risk of future exacerbations.Citation18 This analysis of FLAME study data provides an insight into treatment effects in Asian patients relative to those in other regions in terms of response to LABA/LAMA dual bronchodilator therapy versus LABA/ICS combination therapy. It is notable that the rate of exacerbations in both treatment groups was lower in the Asian cohort than in the overall population. Such lower frequency of exacerbations compared with the total population was also observed in similar cohort analyses of Japanese patients participating in the UPLIFT trialCitation26 and in another Japanese cohort study.Citation27
In the Asian cohort, IND/GLY was superior to SFC in providing statistically significant reduction in the rate of moderate or severe COPD exacerbations, which is important since reduced risk of these exacerbations is linked with decreased morbidity, mortality, and health care costs in COPD patients.Citation28 This finding is consistent with the overall study findings and with those from a previous study in exacerbating patients in which IND/GLY significantly reduced the risk of moderate or severe exacerbation versus LABA/ICS in predominantly Chinese patients with moderate-to-severe COPD.Citation15 The results are also in line with previous reports where effect of IND/GLY on exacerbations was superior to LAMA monotherapy in patients with severe-to-very severe COPD.Citation29 Furthermore, IND/GLY prolonged the time to first moderate or severe COPD exacerbation versus SFC in Asian patients with an effect similar to that seen in the overall study population. The reduced time to exacerbation with IND/GLY in this cohort is notable because it is the first LABA/LAMA to demonstrate this, whereas another LABA/LAMA umeclidinium/vilanterol failed to prolong time to first exacerbation versus placebo at 62.5/25 µg (its approved dose in Asia) in Asian patients.Citation30 In the Asian cohort, the effect of IND/GLY compared with SFC in reducing the rate of all (mild, moderate, or severe) COPD exacerbations was comparable to that seen in the overall FLAME study; however, statistical significance could not be reached in this cohort, which represented <20% of the overall study population. This may also be due to the smaller effect observed with all exacerbations in the Asian cohort compared with the overall study population.
IND/GLY also provided consistently superior improvement in lung function over the study duration. Furthermore, exacerbations and health status are closely related,Citation19 and reducing exacerbations improves health status. IND/GLY improved the health status of patients, as evident in the improvements in SGRQ-C total scores throughout the treatment duration. Symptomatic benefits with IND/GLY were seen in terms of reduced rescue medication use compared with SFC. These findings are also consistent with the results of previous studies conducted in predominantly Caucasian patients with COPD, which also indicated improvements in lung function, symptoms, and health status with once-daily IND/GLY compared with SFC in patients with or without a history of COPD exacerbations.Citation14,Citation31 Overall, the pattern of response to IND/GLY treatment in Asian patients for efficacy parameters was generally comparable with that observed in the overall population. Furthermore, it has been previously shown that in patients with severe COPD receiving LABA/LAMA therapy along with ICS, the risk of moderate or severe exacerbations was similar among those who discontinued ICS and those who continued ICS; therefore, ICS therapy may not be essential in these patients.Citation32
Once-daily IND/GLY was well tolerated with a good safety profile in terms of incidence of AEs, SAEs, deaths, and MACEs, similar to that reported previously.Citation33,Citation34 The incidence of AEs with IND/GLY and SFC was comparable; no new safety concerns were identified. Importantly, the risk of pneumonia was less with IND/GLY compared with SFC. ICS therapy has been shown to be associated with an increased risk of pneumonia in patients with COPD,Citation35,Citation36 which was reflected in this study where a 2-fold higher incidence of pneumonia was reported with SFC compared with IND/GLY. Again, it is notable that pneumonia was reported more commonly in the Asian cohort than in the overall study population.
Our findings indicate that together with the exacerbation outcomes and lowered risk of pneumonia, LABA/LAMA therapy could be positioned as potential first-line maintenance treatment option in COPD treatment guidelines, especially in the context of the Asian population.Citation37–Citation39
Conclusion
Despite minor differences in baseline characteristics and perceived influence of interethnic differences between the Asian and overall populations of the FLAME study, IND/GLY 110/50 µg q.d. showed generally similar reductions in moderate or severe COPD exacerbations, improved lung function, and improved health status versus SFC in the Asian cohort when compared with the total FLAME population. An overall benefit was observed with a reduced risk of pneumonia and with no other discernible safety concern for IND/GLY. These findings represent important new evidence in the pharmacological management of COPD. Results of this Asian cohort analysis combined with the overall FLAME results and previous findings from LANTERN shed new light and expand the evidence for dual bronchodilator therapy to be the first-line treatment option in symptomatic COPD patients at risk for future exacerbations in different regions, especially in Asia.
Author contributions
JAW, NZ, MI, MH, RF, CT, FP, and DB all made substantial contributions to the conception and design of the study, the acquisition, analysis, and interpretation of data. All authors contributed toward the drafting of the article and revising it critically for important intellectual content. All authors provided their final approval of the version to be published. The authors are accountable for the accuracy and integrity of this work.
Abbreviations
| AE | = | adverse event |
| b.i.d. | = | twice daily |
| BMI | = | body mass index |
| CXR | = | chest X-ray |
| FEV1 | = | forced expiratory volume in 1 second |
| FVC | = | forced vital capacity |
| GOLD | = | Global initiative for chronic Obstructive Lung Disease |
| GLY | = | glycopyrronium |
| HR | = | hazard ratio |
| ICS | = | inhaled corticosteroid |
| IEC | = | Independent Ethics Committee |
| IND | = | indacaterol |
| IRB | = | Institutional Review Board |
| LABA | = | long-acting β2-agonist |
| LAMA | = | long-acting muscarinic antagonist |
| MACE | = | major adverse cardiovascular event |
| mMRC | = | modified Medical Research Council |
| q.d. | = | once daily |
| RR | = | rate ratio |
| SAE | = | serious adverse event |
| SFC | = | salmeterol/fluticasone propionate combination |
| SGRQ-C | = | St George’s Respiratory Questionnaire for COPD |
Acknowledgments
The authors would like to thank the patients and staff at participating centers in this study. The authors were assisted in the preparation of this manuscript by Rahul Lad, Professional Medical Writer (Novartis). The study was funded by Novartis Pharma AG, Basel, Switzerland.
Supplementary materials
Figure S1 Adjusted mean change from baseline in SGRQ-C total score over 52 weeks (full analysis set).
Abbreviations: b.i.d., twice daily; GLY, glycopyrronium; IND, indacaterol; q.d., once daily; SFC, salmeterol/fluticasone propionate combination; SGRQ-C, St George’s Respiratory Questionnaire for COPD.
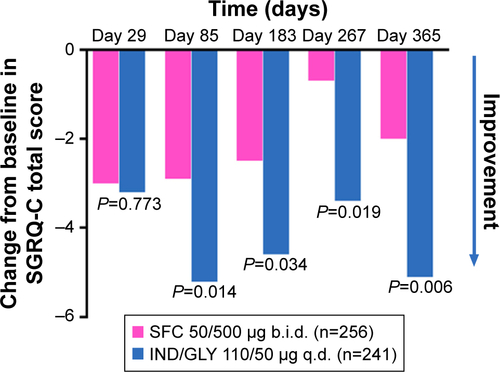
Table S1 Number of patients from each Asian country by treatment
Table S2 Moderate or severe COPD exacerbations during double-blind treatment (full analysis set)
Table S3 COPD exacerbations (mild, moderate, or severe) during double-blind treatment (full analysis set)
Disclosure
JAW has received no honoraria from industry for lectures and/or advisory boards from January 2015. Prior to January 2015 she received honoraria for lectures and/or advisory boards from Novartis, GSK, Astra Zeneca, Boehringer Ingelheim, Takeda, and Johnson and Johnson. JAW has received research grant funding in the last 3 years from Johnson and Johnson, Takeda, GSK, and Vifor Pharma. MI has served on Scientific Advisory Boards for AstraZeneca, Nippon Boehringer Ingelheim, and Novartis Pharma KK from January 2015. MI has received honoraria for speaking from AstraZeneca, GSK, Nippon Boehringer Ingelheim, Kyorin, and Novartis Pharma in 2015. NZ does not have any competing interests to declare. MH, RF, CT, FP, and DB are Novartis employees. The authors report no other conflicts of interest in this work.
References
- Lopez-CamposJLTanWSorianoJBGlobal burden of COPDRespirology2016211142326494423
- World Health Organization [webpage on the Internet]Global Burden of Chronic Respiratory Disease2016 Available from: http://www.who.int/respiratory/copd/burden/en/Accessed May 3, 2016
- OhYMBhomeABBoonsawatWCharacteristics of stable chronic obstructive pulmonary disease patients in the pulmonology clinics of seven Asian citiesInt J Chron Obstruct Pulmon Dis20138313923378753
- LimSLamDCMuttalifARImpact of chronic obstructive pulmonary disease (COPD) in the Asia-Pacific region: the EPIC Asia population-based surveyAsia Pac Fam Med2015141425937817
- TanWCSealePIpMTrends in COPD mortality and hospitalizations in countries and regions of Asia-PacificRespirology2009141909719144054
- ZhongNWangCYaoWPrevalence of chronic obstructive pulmonary disease in China: a large, population-based surveyAm J Respir Crit Care Med2007176875376017575095
- CaramoriGAdcockIMPapiAClinical definition of COPD exacerbations and classification of their severitySouth Med J2009102327728219204646
- AnzuetoAImpact of exacerbations on COPDEur Respir Rev20101911611311820956179
- WedzichaJASeemungalTACOPD exacerbations: defining their cause and preventionLancet2007370958978679617765528
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) [homepage on the Internet]The Global Strategy for the Diagnosis, Management and Prevention of COPD2016 Available from: http://www.goldcopd.orgAccessed 3 May 2016
- National Institute for Health and Care Excellence (NICE)Chronic Obstructive Pulmonary Disease. Management of Chronic Obstructive Pulmonary Disease in Adults in Primary and Secondary Care. NICE Clinical Guideline 101 (Partial Update)LondonNational Institute for Health and Care Excellence (NICE)2010
- CrimCCalverleyPMAndersonJAPneumonia risk in COPD patients receiving inhaled corticosteroids alone or in combination: TORCH study resultsEur Respir J200934364164719443528
- SuissaSPatenaudeVLapiFErnstPInhaled corticosteroids in COPD and the risk of serious pneumoniaThorax201368111029103624130228
- MateraMGRoglianiPCazzolaMQVA149 (indacaterol/glycopyrronium) for the treatment of chronic obstructive pulmonary diseaseExpert Opin Pharmacother20151671079109025843089
- ZhongNWangCZhouXLANTERN: a randomized study of QVA149 versus salmeterol/fluticasone combination in patients with COPDInt J Chron Obstruct Pulmon Dis2015101015102626082625
- AsaiKMinakataYHirataKQVA149 once-daily is safe and well tolerated and improves lung function and health status in Japanese patients with COPD: the ARISE studyEur Repir J2013423392
- HashimotoSIkeuchiHMurataSKitawakiTIkedaKBanerjiDEfficacy and safety of indacaterol/glycopyrronium in Japanese patients with COPD: a subgroup analysis from the SHINE studyInt J Chron Obstruct Pulmon Dis2016112543255127785010
- WedzichaJABanerjiDChapmanKRIndacaterol-glycopyrronium versus salmeterol-fluticasone for COPDN Engl J Med2016374232222223427181606
- SeemungalTADonaldsonGCPaulEABestallJCJeffriesDJWedzichaJAEffect of exacerbation on quality of life in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med1998157141814229603117
- AnthonisenNRManfredaJWarrenCPHershfieldESHardingGKNelsonNAAntibiotic therapy in exacerbations of chronic obstructive pulmonary diseaseAnn Intern Med19871061962043492164
- HurstJRVestboJAnzuetoASusceptibility to exacerbation in chronic obstructive pulmonary diseaseN Engl J Med2010363121128113820843247
- BlasiFCesanaGContiSThe clinical and economic impact of exacerbations of chronic obstructive pulmonary disease: a cohort of hospitalized patientsPLoS One201496e10122824971791
- TanWCNgTPWhere east meets westChest200813351752718252918
- YasudaSUZhangLHuangSMThe role of ethnicity in variability in response to drugs: focus on clinical pharmacology studiesClin Pharmacol Ther200884341742318615002
- MartinABadrickEMathurRHullSEffect of ethnicity on the prevalence, severity, and management of COPD in general practiceBr J Gen Pract201262595e76e8122520773
- FukuchiYFernandezLKuoHPEfficacy of tiotropium in COPD patients from Asia: a subgroup analysis from the UPLIFT trialRespirology201116582583521539680
- SuzukiMMakitaHItoYMHokkaido COPD Cohort Study InvestigatorsClinical features and determinants of COPD exacerbation in the Hokkaido COPD cohort studyEur Respir J20144351289129724232696
- SeemungalTAHurstJRWedzichaJAExacerbation rate, health status and mortality in COPD – a review of potential interventionsInt J Chron Obstruct Pulmon Dis2009420322319554195
- WedzichaJADecramerMFickerJHAnalysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomised, double-blind, parallel-group studyLancet Respir Med20131319920924429126
- ZhengJZhongNNewlandsAChurchAGohAHEfficacy and safety of once-daily inhaled umeclidinium/vilanterol in Asian patients with COPD: results from a randomized, placebo-controlled studyInt J Chron Obstruct Pulmon Dis2015101753176726366068
- VogelmeierCFBatemanEDPallanteJEfficacy and safety of once-daily QVA149 compared with twice-daily salmeterol-fluticasone in patients with chronic obstructive pulmonary disease (ILLUMINATE): a randomised, double-blind, parallel group studyLancet Respir Med201311516024321804
- MagnussenHDisseBRodriguez-RoisinRWithdrawal of inhaled glucocorticoids and exacerbations of COPDN Engl J Med2014371141285129425196117
- WedzichaJADahlRBuhlRPooled safety analysis of the fixed-dose combination of indacaterol and glycopyrronium (QVA149), its monocomponents, and tiotropium versus placebo in COPD patientsRespir Med2014108101498150725135743
- DahlRChapmanKRRudolfMSafety and efficacy of dual bronchodilation with QVA149 in COPD patients: the ENLIGHTEN studyRespir Med2013107101558156723867808
- DiSantostefanoRLSampsonTLeHVHindsDDavisKJBakerlyNDRisk of pneumonia with inhaled corticosteroid versus long-acting bronchodilator regimens in chronic obstructive pulmonary disease: a new-user cohort studyPLoS One201495e9714924878543
- ErnstPSaadNSuissaSInhaled corticosteroids in COPD: the clinical evidenceEur Respir J201545252553725537556
- HizawaNLAMA/LABA vs ICS/LABA in the treatment of COPD in Japan based on the disease phenotypesInt J Chron Obstruct Pulmon Dis2015101093110226089659
- HoritaNKanekoTRole of combined indacaterol and glycopyrronium bromide (QVA149) for the treatment of COPD in JapanInt J Chron Obstruct Pulmon Dis20151081382225960646
- SinghDNew combination bronchodilators for chronic obstructive pulmonary disease: current evidence and future perspectivesBr J Clin Pharmacol201579569570825377687