

Abstract
Background
When discontinuation in COPD randomized controlled trials (RCTs) is unevenly distributed between treatments (differential dropout), the capacity to demonstrate treatment effects may be reduced. We investigated the impact of the time of differential dropout on exacerbation outcomes in RCTs, in relation to study duration and COPD severity.
Methods
A post hoc analysis of 2,345 patients from three RCTs of 6- and 12-month duration was performed to compare budesonide/formoterol and formoterol in moderate, severe, and very severe COPD. Outcomes were exacerbation rate, time-to-first exacerbation, or discontinuation; patients were stratified by disease severity. Outcomes were studied by censoring data monthly from 1 to 12 months.
Results
In patients treated with budesonide/formoterol, annualized exacerbation rates (AERs) were comparable for each study duration (rate ratio [RR] =0.6). With formoterol, the AER decreased with study duration (RR =1.20 at 1 month to RR =0.86 at 12 months). There was a treatment-related difference in exacerbation rates of 45%–48% for shorter study durations (≤4 months) and 27% for 12-month duration. This treatment-related difference in exacerbation rates was comparable for the three disease severities in studies ≤4 months (range: 39%–51%), but this difference decreased with longer study durations, especially in more severe groups (22% and 29% at 12 months). There were fewer discontinuations with budesonide/formoterol; the treatment-related difference in time-to-first discontinuation decreased by study duration (35%, 30%, 26%, and 22% at 3, 6, 9, and 12 months, respectively). Numbers of differential dropouts increased with increasing disease severity, being greatest during second, third, and fourth months.
Conclusions
COPD severity and study duration impact exacerbation as an outcome in double-blind RCTs. This effect is most obvious in patients with severe/very severe COPD and in studies that are longer than 4 months. Early differential dropout particularly impacts study outcome, producing a “healthy survivor effect,” which reduces estimations of treatment impact on exacerbations.
Supplementary materials
Figure S1 Exacerbation rate for budesonide/formoterol and formoterol over time according to COPD disease severity: (A) moderate COPD, (B) severe COPD, and (C) very severe COPD.
Note: Data are presented as 95% confidence intervals.
Abbreviations: BUD, budesonide; FORM, formoterol.
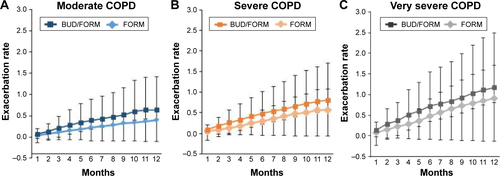
Table S1 Annualized exacerbation rates for budesonide/formoterol and formoterol for all patients
Table S2 Exacerbation rate ratios for budesonide/formoterol compared with formoterol in all patients and in the three COPD disease severity groups
Table S3 Time-to-first exacerbation for budesonide/formoterol and formoterol in all patients and according to COPD disease severity group
Table S4 Time-to-discontinuations for budesonide/formoterol versus formoterol in all patients and according to COPD disease severity group
Acknowledgments
This study was funded by AstraZeneca. The authors would like to thank Shaun Foley and Clair Clowes of inScience Communications, Springer Healthcare, who provided editing assistance, funded by AstraZeneca.
Author contributions
All authors contributed to data interpretation, and conceiving, writing, and revising of the manuscript. All authors approved the final version of the manuscript. ML was responsible for statistical analyses. GE, the corresponding author, had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Disclosure
GE consults for Airsonett, ALK, Almirall, MVIC, and Novartis. He is an ex-employee of AstraZeneca (March 2013).
PMC is a board member for Boehringer Ingelheim, the Department of Health Respiratory Programme Board, GlaxoSmithKline, and Nycomed. He has been a consultant for Novartis and provided expert testimony for Forest. PMC has received honoraria for advising on the conduct and analysis of clinical trial data from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Nycomed. He has also spoken at meetings supported by these companies. Support for travel to meetings has been provided by AstraZeneca.
CRJ is an advisory board member for AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Merck Limited, and Novartis, and a consultant for AstraZeneca, GlaxoSmithKline, Pieris, and Chiesi. Educational presentations have been developed for AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Novartis, with honoraria paid to CRJ or her institution. Lectures have been presented on behalf of AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, and Novartis. Support for travel to advisory meetings has been provided by AstraZeneca, Novartis, and Boehringer Ingelheim.
ARA is a consultant and speaker for AstraZeneca, Bayer Pharma, Boehringer Ingelheim, Sunovion Pharma, GlaxoSmithKline, and Pfizer, and has received honoraria from these companies. Educational presentations have been developed for AstraZeneca, Bayer Pharma, Boehringer Ingelheim, Sunovion Pharma, GSK, and Pfizer. University of Texas Health Science Center at San Antonio has received money for research to perform clinical trials. Support for travel to meetings has also been provided by AstraZeneca.
BJM is an advisory board member for Aerocrine, AstraZeneca, Boehringer Ingelheim, CSL Bering, Forest, Novartis, and Theravance, and a consultant for Astellas, Forest, and Chiesi. Clinical trial data have been reviewed for Spiration, with grants received and controlled by National Jewish Health from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Forest, MedImmune, Nabi, National Institutes of Health, Pfizer, and Sunovion. Lectures have been presented on behalf of Boehringer Ingelheim and GlaxoSmithKline. Educational presentations and programs have been developed (Carden Jennings, Cleveland Clinic, Consensus Medical, Foundation for Improving Patient Outcomes, Hybrid Communications, Integrity, Intellisphere, Medscape, National Jewish Health, Projects in Knowledge, SPIRE, Synapse, and WebMD). Royalties have been received from Up-To-Date. BJM has been a speaker for educational programs at Abbott, the American Academy of Family Practice, the American College of Chest Physicians, and the American Thoracic Society. Support for travel to meetings has also been provided by AstraZeneca.
The University of Groningen has received honoraria for DSP advising on the conduct and analysis of clinical trial data from AstraZeneca, Nycomed, and Teva, as well as for lectures at meetings supported by AstraZeneca, Chiesi, GlaxoSmithKline, Nycomed, and Teva. The University of Groningen has received money for research by unrestricted educational grants from AstraZeneca and Chiesi. AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and Nycomed have provided support for travel to meetings.
ML and MF are employees of AstraZeneca and own stocks within the company.