

Abstract
Background and objective
Identification of smokers having predisposition to COPD is important for early intervention to reduce the huge global burden of the disease. Using a guinea pig model, we have shown that p-benzoquinone (p-BQ) derived from cigarette smoke (CS) in the lung is a causative factor for CS-induced emphysema. p-BQ is also derived from CS in smokers and it elicits the production of anti-p-BQ antibody in humans. We therefore hypothesized that anti-p-BQ antibody might have a protective role against COPD and could be used as a predictive biomarker for COPD in smokers. The objective of this study was to compare the serum anti-p-BQ antibody level between smokers with and without COPD for the evaluation of the hypothesis.
Methods
Serum anti-p-BQ antibody concentrations of current male smokers with (n=227) or without (n=308) COPD were measured by an indirect enzyme-linked immunoabsorbent assay (ELISA) developed in our laboratory. COPD was diagnosed by spirometry according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines.
Results and discussion
A significant difference was observed in the serum anti-p-BQ antibody level between smokers with and without COPD (Mann–Whitney U-test =4,632.5, P=0.000). Receiver operating characteristic (ROC) curve analysis indicated that the ELISA had significant precision (area under the curve [AUC] =0.934, 95% confidence interval [CI]: 0.913–0.935) for identifying smokers with COPD from their low antibody level. The antibody cutoff value of 29.4 mg/dL was constructed from the ROC coordinates to estimate the risk for COPD in smokers. While 90.3% of smokers with COPD had a low antibody value (≤29.4 mg/dL), the majority (86.4%) of smokers without COPD had a high antibody value (≤29.4 mg/dL); 13.6% of current smokers without COPD having an antibody level below this cutoff value (odds ratio [OR] =59.3, 95% CI: 34.15–101.99) were considered to be at risk for COPD.
Conclusion and future directions
Our results indicate that serum anti-p-BQ antibody level may be used as a biomarker to identify asymptomatic smokers at risk for COPD for early intervention of the disease.
Supplementary materials
Figure S1 Standard curve showing amount of anti-p-BQ antibody against absorbance at 490 nm (A490).
Notes: Standard curve was obtained by plotting mean ± SD (n=3) ELISA absorbance at 490 nm (A490) values (y-axis) against amount (nanograms) of polyclonal anti-p-BQ antibody added per well (x-axis). Polyclonal anti-p-BQ antibody was raised in rabbit (Abexome Biosciences, Bangalore, India). Each well on the ELISA plate was coated with 100 ng of HSA-p-BQ conjugate (1:60). Details are given in the “Methods” section. The R2 value of the curve (equation: y =0.011x) was 0.991.
Abbreviations: BQ, benzoquinone; ELISA, enzyme-linked immunoabsorbent assay; HSA, human serum albumin.
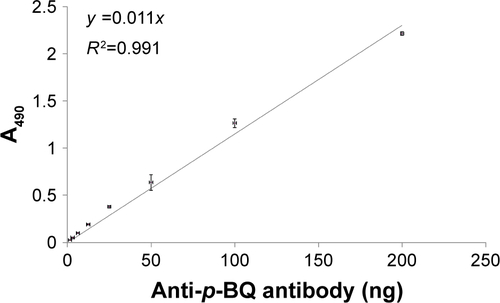
Table S1 Descriptive statistics of attributes age, BMI, postbronchodilator FEV1 (% predicted), postbronchodilator FEV1/FVC (%) in smokers without and with COPD
Table S2 Descriptive statistics of attributes pack-years of smoking and serum anti-p-BQ antibody (mg/dL of serum) in smokers without COPD and smokers with COPD
Acknowledgments
This work was supported by grants from the Juthika Research Foundation and the Krishna and Sukhomay Lahiri Cancer Research Foundation of Calcutta University.
Author contributions
IBC conceived the idea and the project, supervised the project and wrote the manuscript. IBC and SB designed and performed the experiments and partly carried out statistical analysis. PB supplied blood samples and reviewed the clinical data and the manuscript critically. SM supplied blood samples and reviewed the clinical data. SK was an advisor for the project and participated in the design of the experiment. SP reviewed the clinical data and carried out statistical analysis. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.