

Abstract
Chronic obstructive pulmonary disease (COPD), a complex progressive disease, is currently the third leading cause of death worldwide. One recommended treatment option is fixed-dose combination therapy of an inhaled corticosteroid (ICS)/long-acting β-agonist. Clinical trials suggest pressurized metered-dose inhalers (pMDIs) and dry powder inhalers (DPIs) show similar efficacy and safety profiles in COPD. Real-world observational studies have shown that combination therapy has significantly greater odds of achieving asthma control when delivered via pMDIs. Our aim was to compare effectiveness, in terms of moderate/severe COPD exacerbations and long-acting muscarinic antagonist (LAMA) prescriptions, for COPD patients initiating fluticasone propionate (FP)/salmeterol xinafoate (SAL) via pMDI versus DPI at two doses of FP (500 and 1,000 μg/d) using a real-life, historical matched cohort study. COPD patients with ≥2 years continuous practice data, ≥2 prescriptions for FP/SAL via pMDI/DPI, and no prescription for ICS were selected from the Optimum Patient Care Research Database. Patients were matched 1:1. Rate of moderate/severe COPD exacerbations and odds of LAMA prescription were analyzed using conditional Poisson and logistic regression, respectively. Of 472 patients on 500 μg/d, we observed fewer moderate/severe exacerbations in patients using pMDI (99 [42%]) versus DPI (115 [49%]) (adjusted rate ratio: 0.71; 95% confidence interval: 0.54, 0.93), an important result since the pMDI is not licensed for COPD in the UK, USA, or China. At 1,000 μg/d, we observed lower LAMA prescription for pMDI (adjusted odds ratio: 0.71; 95% confidence interval: 0.55, 0.91), but no difference in exacerbation rates, potentially due to higher dose of ICS overcoming low lung delivery from the DPI.
Supplementary material
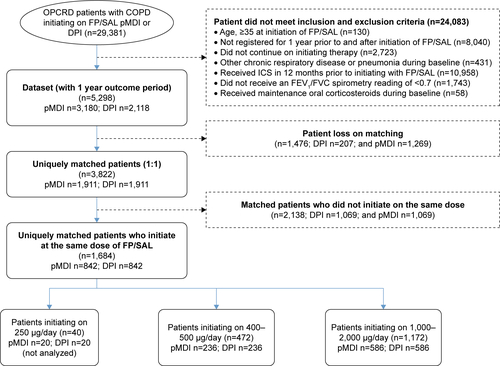
Figure S1 Patient flow diagram.
Abbreviations: COPD, chronic obstructive pulmonary disease; DPI, dry powdered inhaler; FEV1, forced expiratory volume in 1 second; FP/SAL, fluticasone propionate/salmeterol xinafoate; FVC, forced vital capacity; ICS, inhaled corticosteroids; OPCRD, Optimum Patient Care Research Database; pMDI, pressurized metered-dose inhaler.
Acknowledgments
The study was funded with institutional support from Mundipharma International Limited. Study design, analysis, and data interpretation were reviewed independently by all authors.
Disclosure
RJ has received personal fees from Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Pfizer, and Nutricia; grants, personal fees, and nonfinancial support from Novartis and Astra Zeneca; and personal fees and nonfinancial support from Mundipharma. J Martin is a former employee of Observational & Pragmatic Research Institute. VT is an employee of Cambridge Research Support. DS is an employee of Optimum Patient Care (OPC). J Marshall is an employee of Mundipharma International Limited. MSDA is an employee of the Observational & Pragmatic Research Institute (OPRI). Observational and Pragmatic Research Institute Pte Ltd conducted this study, with institutional support from Mundipharma and has conducted paid research in respiratory disease on behalf of the following organizations: UK National Health Service, British Lung Foundation, Aerocrine, AKL Research and Development Ltd, AstraZeneca, Boehringer Ingelheim, Chiesi, Meda, Mundipharma, Napp, Novartis, Pfizer, Respiratory Effectiveness Group, Takeda, Teva Pharmaceuticals, Theravance, and Zentiva. DP has board membership with Aerocrine, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Mundipharma, Napp, Novartis, and Teva Pharmaceuticals; consultancy agreements with Almirall, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Mylan, Mundipharma, Napp, Novartis, Pfizer, Teva Pharmaceuticals, and Theravance; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from Aerocrine, AKL Research and Development Ltd, AstraZeneca, Boehringer Ingelheim, British Lung Foundation, Chiesi, Mylan, Mundipharma, Napp, Novartis, Pfizer, Respiratory Effectiveness Group, Teva Pharmaceuticals, Theravance, UK National Health Service, Zentiva; payment for lectures/speaking engagements from Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mylan, Merck, Mundipharma, Novartis, Pfizer, Skyepharma, and Teva Pharmaceuticals; payment for manuscript preparation from Mundipharma and Teva Pharmaceuticals; payment for the development of educational materials from Mundipharma and Novartis; payment for travel/accommodation/meeting expenses from Aerocrine, AstraZeneca, Boehringer Ingelheim, Mundipharma, Napp, Novartis, and Teva Pharmaceuticals; funding for patient enrollment or completion of research from Chiesi, Novartis, Teva Pharmaceuticals, and Zentiva; stock/stock options from AKL Research and Development Ltd which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia, Singapore, and UK) and 74% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); and is peer reviewer for grant committees of the Efficacy and Mechanism Evaluation program, and Health Technology Assessment. Seretide®, Accuhaler®, Diskus®, and Evohaler® are registered trademarks of Glaxo Group Limited. The authors report no other conflicts of interest in this work.