

Abstract
Background
There is conflicting information regarding the effects of selective and nonselective beta-blocker treatment in patients with COPD.
Participants and methods
This nested case–control study used the Taiwan National Health Insurance Research Database. We included COPD patients who used inhalation steroid and beta-blockers between 1998 and 2010. From this cohort, there were 16,067 patients with severe exacerbations included in the analysis and 55,970 controls matched on age, sex, COPD diagnosis year, and beta-blockers treatment duration by risk set sampling.
Results
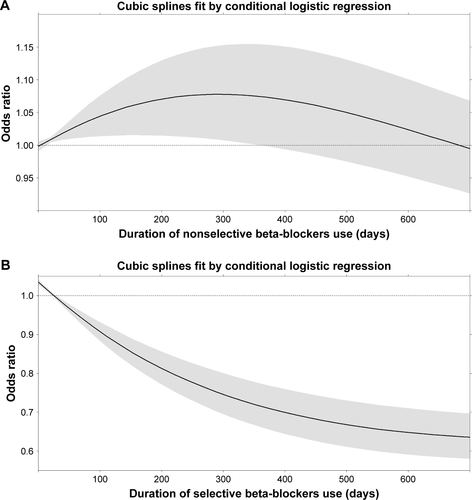
For the selective beta-blocker users, the current users had a lower risk of severe exacerbations than the nonusers (odds ratio [OR], 0.90; 95% confidence interval [CI], 0.85–0.96). In contrast, for the nonselective beta-blocker users, the current users had a higher risk of severe acute exacerbations than the nonusers (OR, 1.21; 95% CI, 1.14–1.27). A higher risk of severe exacerbation during increasing mean daily dose or within about the initial 300 days was found in nonselective beta-blockers, but not in selective beta-blockers. One selective beta-blocker, betaxolol, had a significantly lower risk of severe exacerbations (OR, 0.75; 95% CI, 0.60–0.95). Two nonselective beta-blockers (labetalol and propranolol) were associated with a significantly higher risk of exacerbations (OR, 1.49; 95% CI, 1.32–1.67 for labetalol; OR, 1.16; 95% CI, 1.10–1.23 for propranolol).
Conclusion
Selective beta-blockers can be cautiously prescribed for patients with COPD and cardiovascular disease (CVD), however, nonselective beta-blockers should not be prescribed for patients with COPD. Betaxolol may be the preferred choice of suitable selective beta-blocker for patients with COPD, however, labetalol and propranolol should be avoided for patients with COPD.
Keywords:
Supplementary materials
Figure S1 Study flow chart.
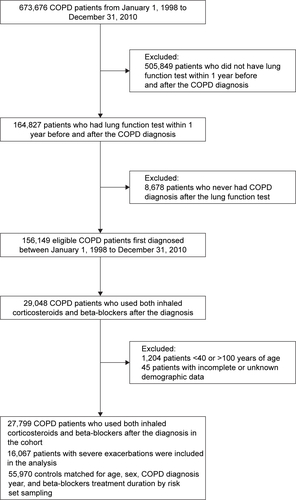
Figure S2 Occurrence of severe acute exacerbation vs mean daily dose (DDD) of (A) nonselective and (B) selective beta-blockers.
Abbreviation: DDD, defined daily dose.
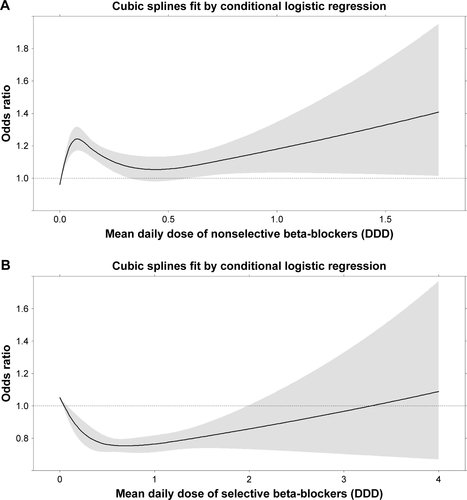
Figure S3 Occurrence of severe acute exacerbation vs duration (days) of (A) nonselective and (B) selective beta-blockers.
Acknowledgments
Taiwan Clinical Trial Consortium for Respiratory Diseases (TCORE) includes Chong-Jen Yu, MD, PhD (National Taiwan University Hospital [NTUH], Director of Coordinating Center and Core Principal Investigator [PI] of Committee); Hao-Chien Wang, MD, PhD (NTUH, PI of Committee); Diahn-Warng Perng, MD, PhD (Taipei Veterans General Hospital, PI of Committee); Shih-Lung Cheng, MD, PhD (Far Eastern Memorial Hospital, PI of Committee); Jeng-Yuan Hsu, MD, PhD (Taichung Veterans General Hospital, PI of Committee); Wu-Huei Hsu, MD, PhD (China Medical University Hospital, PI of Committee); Ying-Huang Tsai, MD, PhD (Chang Gung Memorial Hospital, Chiayi, PI of Committee); Tzuen-Ren Hsiue, MD, PhD (National Cheng Kung University Hospital, PI of Committee); Meng-Chih Lin, MD, PhD (Chang Gung Memorial Hospital, Kaohsiung, PI of Committee); Hen-I Lin, MD (Cardinal Tien Hospital and School of Medicine, PI of Committee); Cheng-Yi Wang, MD, PhD (Cardinal Tien Hospital and School of Medicine, PI of Committee); Yeun-Chung Chang, MD, PhD (NTUH, PI of Committee); Ueng-Cheng Yang, PhD (National Yang-Ming University, PI of Committee); Chung-Ming Chen, PhD (NTU, PI of Committee); Cing-Syong Lin, MD, PhD (Changhua Christian Hospital, PI of Committee); Likwang Chen, PhD (NHRI, PI of Committee); Yu-Feng Wei, MD (E-Da Hospital, PI of Committee); Inn-Wen Chong, MD (Kaohsiung Medical University Chung-Ho Memorial Hospital, PI of Committee); and Chung-Yu Chen (NTUH, Yun-Lin, PI of Committee). This study was supported by grants from the National Science Council (NSC 104-2314-B-002-185-MY2, 101-2325-B-002-064, 102-2325-B-002-087, 103-2325-B-002-027, 104-2325-B-002-035, 105-2325-B-002-030, 104-2314-B-567-002, and 105-2314-B-567-001), Cardinal Tien Hospital and School of Medicine (FU10007, CTH-102-1-2B12, and CTH-103-1-2B02), and NHRI (intra-mural funding).
Disclosure
The authors report no conflicts of interest in this work.