

Abstract
Background
Emphysema is a distinct feature for classifying COPD, and smoking history (≥10 pack-years) is one of several newly proposed criteria for asthma–COPD overlap (ACO). We studied whether or not a smoking history (≥10 pack-years) and emphysema are useful markers for classifying ACO and differentiating it from asthma with chronic airflow obstruction (CAO).
Methods
We retrospectively studied the mortalities and frequencies of exacerbation in 256 consecutive patients with ACO (161 with emphysema and 95 without emphysema) who had ≥10 pack-years smoking history, 64 asthma patients with CAO but less of a smoking history (<10 pack-years) and 537 consecutive patients with COPD (452 with emphysema and 85 without emphysema) from 2000 to 2016. In the patients with emergent admission, the causes were classified into COPD exacerbation, asthma attack, and others.
Results
No asthma patients with CAO had emphysema according to computed tomography findings. The prognoses were significantly better in patients with asthma and CAO than in those with ACO and COPD and better in those with ACO than in those with COPD. In both ACO and COPD patients, the prognoses were better in patients without emphysema than in those with it (P=0.027 and P=0.023, respectively). The frequencies of emergent admission were higher in COPD patients than in ACO patients, and higher in patients with emphysema than in patients without emphysema. ACO/emphysema (+) patients experienced more frequent admission due to COPD exacerbation (P<0.001), while ACO/emphysema (−) patients experienced more frequent admission due to asthma attack (P=0.014).
Conclusion
A smoking history (≥10 pack-years) was found to be a useful marker for differentiating ACO and asthma with CAO, and emphysema was a useful marker for classifying ACO. These markers are useful for predicting the overall survival and frequency of exacerbation.
Supplementary materials
Figure S1 Frequencies of total exacerbation events in the subgroups of COPD, ACO, and asthma/CAO.
Abbreviations: ACO, asthma–COPD overlap; asthma/CAO, asthma with CAO; CAO, chronic airflow obstruction.
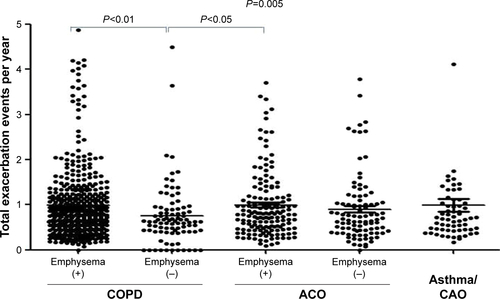
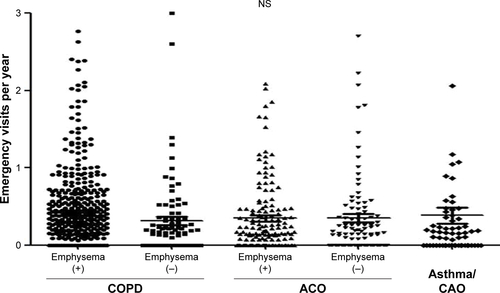
Figure S2 Frequencies of emergency visit in the subgroups of COPD, ACO, and asthma/CAO.
Abbreviations: ACO, asthma–COPD overlap; asthma/CAO, asthma with CAO; CAO, chronic airflow obstruction.
Acknowledgments
The authors wish to thank the medical staff of Saitama Cardiovascular and Respiratory Center who cared for the patients.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.