

Abstract
There is now convincing evidence that the airway epithelium drives the pathogenesis of COPD. A major aspect of this is the disease-related reduction in barrier function that is potentiated by dysregulation of tight junction (TJ) protein complexes. However, a significant number of studies using in vitro smoke exposure models have not observed alterations in barrier permeability. We have previously shown that zinc (Zn) is an influential cytoprotective factor for the airway epithelium, and its depletion by cigarette smoke produces disease-related modifications consistent with inflammatory changes in COPD. We hypothesized that Zn deficiency is a significant co-stimulus with cigarette smoke extract (CSE) for potentiating the leaky barrier phenotype exhibited in COPD. We employed an ex vivo model of differentiated human airway epithelium exposed to Zn depletion and CSE to determine the contribution of Zn in maintaining normal epithelial permeability. Western blot analysis demonstrated a significant downregulation of the TJ proteins such as ZO-1 (−1.93-fold, P<0.05) and Claudin-1 (−3.37-fold, P<0.01) with the combination exposure. Assessment of barrier function via paracellular ionic conductance and tracer permeability also showed that Zn depletion was an important factor, which potentiated an increase in epithelial permeability (P<0.001 for both) compared to Zn depletion or CSE exposures in isolation. Visual inspection of the epithelium using transmission electron microscopy revealed a marked reduction in junction complexes between the adjacent airway epithelial cells treated with a combination of Zn depletion and CSE. These observations identify Zn deficiency as a significant codeterminant with CSE as a factor leading to an increase in airway epithelial permeability. Hence, as Zn dyshomeostasis has been reported in the airway epithelium exposed to chronic cigarette smoke and inflammation, targeting these phenomena may represent a promising strategy to ameliorate the leaky barrier phenotype that is synonymous with COPD.
Supplementary material
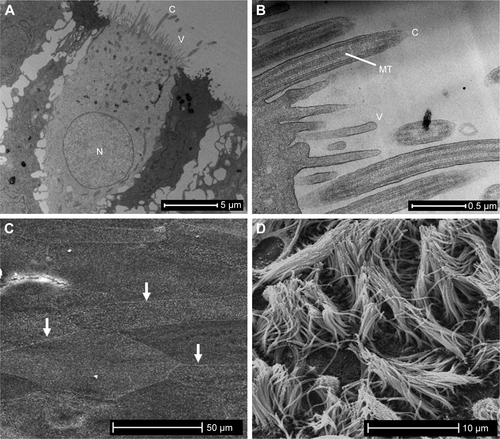
Figure S1 The ex vivo cultures of differentiated primary human AECs share phenotypic barrier structures observed in the airways in vivo.
Notes: An important requisite for assessing the epithelial barrier in the context of COPD is establishing a model that closely approximates the epithelium in the human airways. (A) A low-power TEM image of an AEC grown at an ALI exhibits the features of ciliated AECs found in the human airway with columnar morphology, a basally positioned nucleus, cilia, and villi projecting from the apical membrane, and interactions with adjacent cells at the apicolateral and lateral cell margins. Not shown is the mucus blanket produced by goblet cells that is lost during sample preparation. (B) High-magnification TEM of the apical membrane of an AEC depicting the MTs that are diagnostic features of cilium. The smaller plasma membrane projections are villi. (C) A SEM micrograph of AECs grown at an ALI before the production of cilia (6 days post air exposure), showing the defined apicolateral margins between adjacent cells formed by TJ complexes (three examples shown by arrows). (D) A SEM micrograph shows that cilia and villi formation 28 days after cultures are exposed to air which stimulates mucociliary differentiation. Not shown is high-speed live cell imaging of cilia beating at a frequency of ~10 Hz, and the directional movement of activated charcoal suspended in media on the epithelial layer, which is indicative of synchronous cell-to-cell coordination via GJs.
Abbreviations: AECs, airway epithelial cells; ALI, air–liquid interface; C, cilia; GJs, gap junctions; MTs, microtubules; N, nucleus; SEM, scanning electron microscopy; TEM, transmission electron microscopy; TJ, tight junction; V, villi.
Acknowledgments
We are grateful for the expertise and support of the University of Adelaide Microscopy Suite, the clinical staff and donors of the Royal Adelaide Hospital Thoracic Unit, and Mr Josh Woenig who provided technical support for the tracer assay. We acknowledge the funding provided by the National Health and Medical Research Council (APP1099040), the Thoracic Society of Australia and New Zealand, AstraZeneca Pty Ltd, and the Royal Adelaide Hospital Research Fund.
Disclosure
The authors report no conflicts of interest in this work.