
Abstract
Purpose
There is a lack of consensus on the most appropriate early diagnostic strategy, criteria for early access to treatment and follow-up approach for patients with COPD.
Materials and methods
A Delphi consensus project investigated the early management of COPD. We formulated two questionnaires for completion by pneumologists in Italy.
Results
A total of 207 specialists completed questionnaire 1 and 184 of them questionnaire 2, between November 2016 and October 2017. Early diagnosis of COPD was considered uncommon for 93.2% of the expert panel. Regardless of the definition of “early diagnosis” – a diagnosis made before the clinical manifestation of the disease for most responders (60.4%) – experts were confident of the positive effects of early disease management, which they consider is effective in modifying the natural history of the disease. Lack of awareness of the disease was considered the first limiting factor to early COPD management for 78% of respondents. The most effective steps to reduce functional decline were considered to be smoking cessation, followed by long-acting β2-agonist (LABA)/long-acting muscarinic antagonist (LAMA), LAMA, LABA, and finally inhaled corticosteroid/LABA (P<0.01 for each paired comparison). Specialists considered it “inappropriate” for general practitioners to perform both the early diagnosis and therapy of COPD without the involvement of a specialist.
Conclusion
Early management of COPD is uncommon, and although data on the effects of early disease management on long-term outcomes are limited, Italian experts are confident of the clinical efficacy of this approach.
Introduction
COPD is defined as a “preventable and treatable disease, which is characterised by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases.” It is a major cause of morbidity and mortality worldwide.Citation1 Total deaths from COPD are projected to increase by >30% in the next 10 years, and according to The Global Burden of Disease Study, in 2020 COPD will be the third leading cause of death worldwide.Citation2 Previously, COPD was more common in men, but because of increased tobacco use among women in high-income countries and the higher risk of exposure to indoor air pollution in low-income countries, the disease now affects men and women almost equally. In the International Burden of Obstructive Lung Diseases (BOLD) survey, the prevalence of spirometrically confirmed COPD in adults was estimated to be 10%.Citation3
In the majority of patients, COPD is a progressive condition, with deteriorating lung function over time in addition to the natural decline in pulmonary function that occurs with increasing age. This debilitating and chronic disease carries a significant economic burden on both individuals and society, with direct healthcare costs due primarily to exacerbation-related hospitalizations and indirect costs due to loss of productivity.Citation1,Citation4 The prognosis for COPD patients depends on the severity of disease, those with severe disease are more prone to severe exacerbations, hospitalizations, respiratory failure, and death. Patients with milder disease are at less risk of the above but have an increased risk of disease progression.Citation5 Moreover, patients with mild COPD have a reduced quality of life/exercise tolerance and increased healthcare resource utilization.
Early intervention in COPD, with smoking cessation, pharmacological therapy, and non-pharmacological treatment options such as rehabilitation, can reduce decline in lung function and the risk of exacerbations and improve quality of life, as demonstrated by a recent paper which showed the efficacy of the long-acting muscarinic antagonist (LAMA), tiotropium, on FEV1 decline in patients with early stage disease.Citation5,Citation6 Unfortunately, despite the rising prevalence and substantial socioeconomic impact of COPD, misdiagnosis and underdiagnosis continue to be a central problem in the management of this disease. Generally, many people with COPD, especially those with mild and moderate disease, remain underrecognized, underdiagnosed, and undertreated, even though it is now considered to be treatable.Citation7,Citation8 Undiagnosed early stage COPD, particularly in symptomatic patients, is therefore likely to progress to more severe stages of the disease.
Consensus group methods such the Delphi method have been used successfully in medicine to synthesize expert opinion when GOLD standard evidence is not available.Citation9,Citation10 We conducted a Delphi consensus project to investigate the opinions on the early management of COPD patients – needs, approach to diagnosis and treatment, as well as suggestions on how to improve the early management of COPD.
Materials and methods
The Delphi technique is a validated process to develop consensus and make group-based decisions.Citation11,Citation12 Our study was conducted in four phases: 1) development of the survey questionnaire by the scientific committee; 2) selection of the expert panel; 3) completion of the online survey in two rounds; and 4) analysis of results and discussion of conclusions at an onsite meeting with the scientific committee.
Delphi process
The study was undertaken between November 2016 and September 2017. An advisory board (comprised 13 specialists from Italian universities and public hospitals) reviewed the medical literature on the early management of COPD and developed a questionnaire (Q1) (Supplementary material) including a set of seven demographic and organizational items and a second set of 27 scientific items focusing on epidemiological, diagnostic, and therapeutic topics. Questionnaire Q1 was administered, according to the Delphi method, to an expert panel comprising pulmonologists from the Italian healthcare system recommended by the scientific committee according to the geographical area. For some items participants expressed their opinion on a Likert scale between 0 and 5, while for other items they ordered a set of options according to relevance matching their clinical experience. They also answered open questions. After the ratings from the first round were statistically analyzed, a second questionnaire (Q2) was drawn up and sent to the same professionals who responded to Q1 (Supplementary material). Q2, which included 22 items, was intended to better focus on some aspects and to solve certain ambiguities that emerged from Q1.
Research ethics, confidentially, informed consent, and data protection
Our Delphi study conformed to general ethical requirements aiming to assure “rigor, respect, and responsibility” in the conduct of research projects. The study as such was exempt from the need to obtain formal ethical board approval. Rights involved in the research study were explained at the outset, and by returning the questionnaires, the participants gave their consent to take part in the study. These measures support the ethical principles of respect and the right of self-determination and of obtaining an informed consent. No personal information was collected, and survey responses were collated anonymously. All responses received in the study were kept confidential, and identities of individual participants were not divulged. Survey responses were collected online using a secure Internet server and retained for the duration of the study.
Statistical analyses
To assess the agreement among the experts, the Delphi method uses a scale from 1 (maximal disagreement) to 9 (maximal agreement), with 5 corresponding to a neutral opinion about a given item. Thus, scores given by experts are statistically elaborated to obtain an appropriate “index of consensus.” Inter-percentile Range Adjusted for Symmetry (IPRAS) scores were employed as indicators of the extent of agreement for each item. Using the inter-percentile range/IPRAS computation, each statement can be classified with the appropriateness of a given diagnostic/therapeutic strategy in the following categories: appropriate (panel median of 7–9, without disagreement), uncertain (panel median of 4–6 or any median with disagreement), inappropriate (panel median of 1–3, without disagreement). When ranked in order of importance – 1 was an indicator of the most inappropriate/irrelevant and 5 the most appropriate/relevant. Total scores indicate experts’ level of preference with only those reaching 50% (of maximum) considered and reported. A two-sided significance level α of 0.05 was defined (mean ± SD). As a general rule, non-parametric tests were applied to assess the differences between groups (Kruskal–Wallis and Mann–Whitney) and between items (Friedman and Wilcoxon). Bonferroni adjustment was carried out for multiple comparisons.
Results
The scientific committee recommended that Q1 was sent to 515 pneumologists and allergists working in the Italian healthcare system. The expert panel was representative of the geographic distribution of the hospital and/or university respiratory units in Italy. Feedback was received from 207 clinicians (40% of those initially approached) with a geographical distribution as follows: North (39.1%), Central (29.9%), and South (30.9%). Q2 was dispatched to all those who had previously replied to Q1 (207 experts), and replies were received from 184 (90%). Most clinicians participating in the Delphi study were specialist pneumologists (92.8%).
The average age of all the 207 respondents of Q1 was 53.2±9.2 years. Fifty-two were women (25%) and 155 men (75%). In line with the demographics of medical doctors in Italy, there are more male doctors than female doctors, and female doctors tend to be younger than male doctors (47.4±9.7 and 55.1±8.1 years, respectively). About 21% of the respondents work in respiratory centers with beds reserved for rehabilitation, with spirometers available in 99% of cases. Diffusing capacity of the lungs for carbon monoxide measurement was available in 90%, body plethysmograph in 87%, dosimeter for methacholine in 80%, and cardiopulmonary exercise test in 63%. Waiting times for a spirometry was estimated to be <30 days for 56% of respondents, between 30 and 60 days for 30%, and >60 days for the remaining 14%. On average, 62% of patients were referred to specialists by their general practitioners (GPs) and the remaining 38% referred themselves.
Meaning and importance of “early diagnosis” of COPD
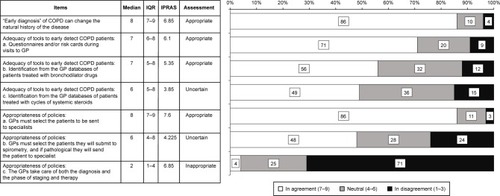
An “early diagnosis” of COPD was considered to be a diagnosis made before clinical manifestation of the disease by the majority of responders (60.4%) (ie, primary prevention); a diagnosis when COPD is mild (secondary prevention) for 33.8% of responders. Only 5.8% of the responders believe that early diagnosis is an approach aimed at reducing the complications of the disease (ie, tertiary prevention). As a general rule, responders were confident of the positive effect of early management of the disease, with a high level of consensus on the question “does an early diagnosis affect the natural history of the disease?” (median of 8.0/9.0 with an interquartile range [IQR] of 7–9, ). Furthermore, 95.7% of responders were convinced that early management of the disease can affect therapeutic success. Moreover, over 90% of the responders treat patients with mild obstruction (ie, FEV1 >80%) in all cases (20%) or in the presence of symptoms (70%).
Figure 1 Level of consensus on the early management of COPD.
Early diagnosis of COPD: fact or fiction?
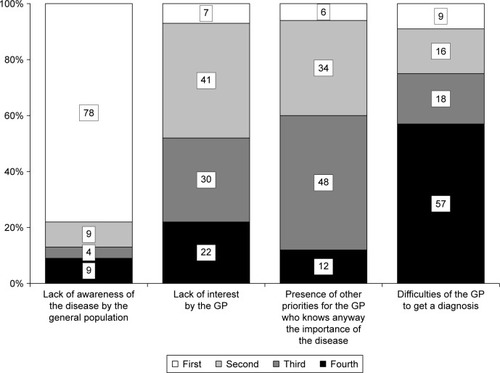
According to those who responded, early diagnosis of COPD is uncommon with only 6.8% of the expert panel stating that it occurs in real-life clinical practice. According to the expert panel, factors limiting early diagnosis and treatment of COPD are (in order to importance): lack of awareness about the disease (78% of respondents), “lack of interest” by GPs (41%), not a priority disease for GPs even if they understand its importance (48%), and difficulties in performing spirometry (57%) (). In total, 12% of the responders replied that on average, new patients report that they have symptoms for <1 year. Importantly, experts replied that only 15% of patients received a diagnosis when their disease was still mild according to spirometry (GOLD 1) and 15.8% were diagnosed according to symptoms/exacerbations (GOLD 1).
Figure 2 Relevance of factors limiting early diagnosis of COPD according to expert panel.
Abbreviation: GP, general practitioner.
Early diagnosis/screening: who should be evaluated?
In reply to the question which categories of smokers should have an early diagnosis, the Expert Panel gave the following importance scores (possible range: min =1, max =5): heavy smokers, 4.2; smokers with comorbidities, 4.0; and young smokers, 3.8. Each pairwise Wilcoxon paired comparison (following a significant overall Friedman’s test, P<0.001) resulted statistically significant (consistently, P<0.020).
Treating patients with mild COPD: the pharmacological approach
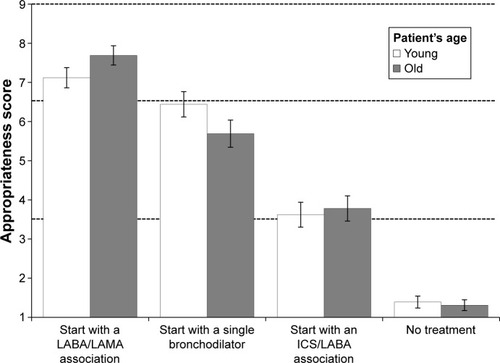
According to the expert panel, the role of patient preference in the choice of therapy is not affected by early diagnosis of the disease (4.0/5.0 in both cases, P=0.136). The level of confidence in the different approaches used to reduce the functional decline in mild COPD were stopping smoking (highest score), followed by a LAMA plus long-acting beta-agonist (LABA), a LAMA, a LABA, and finally inhaled corticosteroid (ICS) plus LABA (P<0.01) for each paired comparison (). In patients with MRC ≥2 dyspnea and a FEV1 between 50% and 80% (moderate obstruction), the level of consensus in different treatments in both younger and older patients is reported in (each paired comparison is significantly different, P<0.001). In terms of appropriateness, the order was 1) LABA/LAMA; 2) single bronchodilator; 3) ICS/LABA; 4) no treatment in both cases with age having a significant effect (P<0.001). The appropriateness of starting with a single bronchodilator (although lower than that of starting with LABA/LAMA) had a higher level of consensus when applied in young patients, whereas LABA/LAMA was assigned a higher level of appropriateness for older patients ().
Figure 3 Level of confidence in different approaches used in the early management of COPD to reduce the functional decline.
Note: Each pairwise comparison was significant (P<0.001).
Abbreviations: ICS, inhaled corticosteroid; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist.
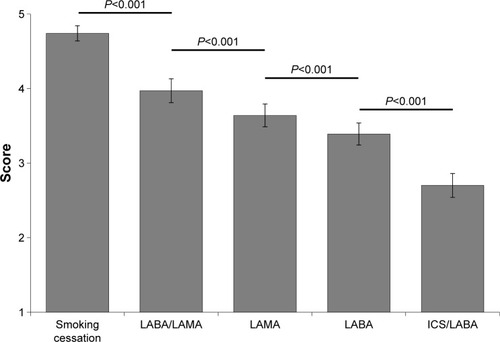
Figure 4 Level of consensus on different treatments in patients younger and older with moderate obstruction (mean ± 95% CI).
Improving early management of COPD patients
Over 50% said that they would be available to promote/be involved in a specific campaign aimed at increasing the level of early management in COPD and over 30% would be available to take part in such an initiative organized by a scientific society.
Subjects to be screened should be selected by GPs (approach considered “appropriate”: median =8, IQR =7–9), while experts are less certain about the role of GPs in spirometry (median =6, IQR =4–8). The involvement of a specialist in the field was considered crucial and respondents considered it “inappropriate” for GPs to perform both diagnosis and therapy of these patients (median =2, IQR =3–4) without the involvement of a specialist (). The tools considered “appropriate” to select subjects to be evaluated for early diagnosis are questionnaires carried out during clinical evaluation (median =7, IQR =6–8) and analysis of the GP database to identify patients treated with bronchodilators (median =7, IQR =5–8). Experts were less sure about a selection based on the use of systemic steroids and/or antibiotics (median =6, IQR =5–8). Experts considered that once early diagnosis was made, follow-up should be carried out by specialists rather than GPs (4.4 vs 2.8 in a 1–5 scale, P<0.001, ).
Discussion
Our Delphi-based study focused on open issues on the optimal strategy for the therapeutic management of patients with early stage COPD. A two-round Delphi consensus explored the opinions of a large number of pneumologists in Italy on the early diagnosis and treatment of COPD. This is one of the few studies to involve such a large cohort of pneumologists (515 experts received the first questionnaire, with 207 replying). Other recently reported study involved up to a maximum of 200 experts in respiratory medcine.Citation13–Citation18
Results of our study show that the majority of experts agreed on most of the proposed items and replies were in-line with the GOLD 2017 recommendations.Citation1 COPD is a progressive condition, and early diagnosis may allow a change in the natural history of COPD with significant savings both in terms of costs to health care systems as well as to patients.Citation19
Smoking cessation is vital to modify the natural history of COPD.Citation20,Citation21 Early pharmacological therapy has also been recognized as an important factor in slowing down the functional decline, reducing the exacerbations/long-term consequences, and improving the quality of life.Citation22–Citation26 Although it is generally accepted that pharmacological therapy should be considered a possible early intervention in COPD, the optimal maintenance therapy – single bronchodilator (short- or long-acting LAMA or LABA) vs LABA-LAMA vs ICS-LABA – is still being debated.Citation27
Our panel of experts addressed these issues and reached a series of outcomes. First, they agreed that an early diagnosis must include primary and secondary prevention (>95% of responders). They were confident that early management of COPD could affect its natural history and over 90% of panelists confirmed that starting long-acting bronchodilators in mildly obstructed both symptomatic and asymptomatic patients was appropriate. American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society guidelines state that available evidence is not sufficient to recommend the use of bronchodilators in asymptomatic individuals.Citation28 The results of our Delphi consensus are in general agreement with international guidelines as the majority of specialists stated they would treat “mild” disease only in the presence of symptoms (70%) and 20% of them sustained that they would treat asymptomatic patients. Nevertheless, there is some evidence that mild/moderate obstruction of airflow can present without actual symptoms and a number of studies report a cohort of patients as COPD patients who have so-called silent obstruction in the absence of symptoms (chronic cough, phlegm, and/or dyspnea) but with airflow limitation on spirometric examinations.Citation29–Citation32 This is not a completely unexpected finding given that the severity of symptoms and airway obstruction are weakly correlated.Citation33 It therefore follows that early intervention may delay or even avoid not just the manifestation of symptoms but also other clinical indicators, such as acute exacerbations, with their attendant long-term consequences. While there is some evidence to support this hypothesis, it needs to be evaluated in prospective clinical trials, as the impact of pharmacological therapy in comparison with smoking cessation is not yet known.Citation34
Our results are similar to those reported by another group of Italian specialists in COPD.Citation35 In our study, experts did not reach a consensus on the effectiveness of increasing the dosage of bronchodilators to better control COPD, but a substantial number considered this to be a fitting approach. In fact, in everyday life, a patient on monotherapy experiencing breathing difficulties will frequently increase the dosage of his/her bronchodilator in the hope of improving symptoms.Citation35,Citation36 Results of our study confirmed previous investigations and the majority of experts were in agreement that patients not fully controlled with a single bronchodilator should receive another bronchodilator preferably with a different mechanism of action.Citation35 It is now well accepted that the combination of a LABA and LAMA is the most appropriate treatment for early COPD, especially in older patients (P<0.001) (). Using multiple drugs in combination has a number of important advantages including decreasing the possibility of adverse effects, simplifying treatment regimens, and increasing adherence to therapy.Citation37
International guidelines (GOLD 2017, 2018) endorse the use of LABAs in combination with antimuscarinics if there is no adequate improvement in symptoms with monotherapy.Citation1 Dual therapy such as fixed combinations of LABA and LAMA has been shown to play an important role in obtaining maximum bronchodilator effects. Results of clinical trials suggest that fixed dose combination bronchodilator therapy provides significantly greater improvements in lung function compared with monotherapy although the precise mechanism has yet to be fully elucidated.Citation35,Citation38,Citation39 It should also be noted that combination therapy is well tolerated in patients with moderate-to-severe COPD.Citation1
Unfortunately, early diagnosis in real-life clinical practice is as yet uncommon not least because patients are referred to specialists when they have moderate to advanced disease. According to our group of experts, the main reason for this seems to a lack of awareness about the disease (77% of responders). It is therefore vital to find strategies to increase patient and physician awareness about COPD, especially in heavy smokers (score 4.2/5 in our expert panel) or when more comorbidities are present (score 4/5). Moreover, even when an early diagnosis is made, non-adherence to medication regimens is a significant problem in the management of COPD.Citation40 It is therefore vital, according to the panel, when faced with a situation where symptoms are not controlled, to first establish if the patient is actually taking the medication as prescribed before deciding to change to a different medication or to increase the dosage of an existing medication (median 7.5, IQR =7–8).
Conclusion
Early management of COPD is not common, and although there are limited data on the effects of early disease management on long-term outcomes, Italian experts are confident of the clinical efficacy of this approach. Smoking cessation should be the first step followed by pharmacological therapies. The expert panel was in agreement on the important role of fixed dosage LABA/LAMA on the natural history of the disease and in preventing/ameliorating functional decline. Finally, the expert panel considered that while GPs are crucial for early diagnosis, the role of specialist is vital in the early management of COPD patients.
The advantage of consensus panels in general and our Delphi study in particular is that they allow expert opinion on a wide variety of topics to be captured – in our case on the management of COPD. While results support the everyday decision-making process in the management of early COPD, they only mirror the Italian situation, and as such, we consider that a multinational survey is necessary to support the consensus scenario and to further investigate some of the issues not yet completely addressed by the current international guidelines.
Author contributions
FDM and MC acted as manuscript coordinators and Patrizio Pasqualetti carried out the statistical analysis. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
This study was supported by an unrestricted grant from AstraZeneca. The funding source had no role in the study design, data collection and analysis, decision to publish, or preparation of manuscript. The authors would like to thank ThinkTank, Milan, for support in implementing the Delphi Methodology.
Disclosure
Dr. Di Marco has received honoraria for lectures at national and international meetings from Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi Farmaceutici, Dompe, Guidotti/Malesci, GlaxoSmithKline, Menarini, Novartis, and Zambon. He has served as a consultant for AstraZeneca, Chiesi Farmaceutici, Novartis, and Zambon. He has received financial support for research from Novartis and Boehringer Ingelheim. Prof. Dr. de Blasio has served as a consultant for AstraZeneca, and Dr. Santus has served as a consultant for AstraZeneca, Boehringer Ingelheim, Zambon Italia, Guiodotti, GSK, and Chiesi Farmaceutici. The authors report no other conflicts of interest in this work.
References
- GOLD [homepage on the Internet]From the Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD)2017 Available from: http://goldcopd.orgAccessed June 2018
- World Health Statistics2008 Available from: http://www.who.int/whosis/whostat/EN_WHS08_Full.pdfAccessed June 2018
- BuistASVollmerWMMcBurnieMAWorldwide burden of COPD in high- and low-income countries. Part I. The burden of obstructive lung disease (BOLD) initiativeInt J Tuberc Lung Dis200812770370818544191
- AnzuetoAImpact of exacerbations on COPDEur Respir Rev20101911611311820956179
- WelteTVogelmeierCPapiACOPD: early diagnosis and treatment to slow disease progressionInt J Clin Pract201569333634925363328
- ZhouYZhongNSLiXTiotropium in early-stage chronic obstructive pulmonary diseaseN Engl J Med20173771092393528877027
- DecramerMMiravitllesMPriceDNew horizons in early stage COPD – improving knowledge, detection and treatmentRespir Med2011105111576158721239156
- British Lung Foundation [homepage on the Internet]Invisible livesChronic obstructive lung disease (COPD) – finding the missing millions2010 Available from: http://www.lunguk.orgAccessed April 2013
- MurphyMKBlackNALampingDLConsensus development methods, and their use in clinical guideline developmentHealth Technol Assess199823188
- FinkAKosecoffJChassinMBrookRHConsensus methods: characteristics and guidelines for useAm J Public Health19847499799836380323
- LinstoneHTuroffMThe Delphi Method Techniques and ApplicationsReading, MAAddison-Wesley Publishing Company19751616
- JonesJHunterDConsensus methods for medical and health services researchBMJ199531170013763807640549
- MiravitllesMSoler-CataluñaJJAlcázarBViejoJLGarcía-RíoFFactors affecting the selection of an inhaler device for COPD and the ideal device for different patient profiles. Results of EPOCA Delphi consensusPulm Pharmacol Ther2018489710329031616
- PadrãoEAraújoDTodo BomAAsthma-COPD overlap: a Portuguese surveyPulmonology2018243174181
- DapariRIsmailHIsmailRIsmailNHApplication of fuzzy Delphi in the selection of COPD risk factors among steel industry workersTanaffos2017161465228638424
- HillATHaworthCSAlibertiSPulmonary exacerbation in adults with bronchiectasis: a consensus definition for clinical researchEur Respir J2017496170005128596426
- PlazaVÁlvarezFCalleMConsensus on the Asthma-COPD Overlap Syndrome (ACOS) Between the Spanish COPD Guidelines (GesEPOC) and the Spanish Guidelines on the Management of Asthma (GEMA)Arch Bronconeumol2017538443449 English, Spanish28495077
- NinaneVCorhayJLGermonpréPInhaled treatment of COPD: a Delphi consensus statementInt J Chron Obstruct Pulmon Dis20171279380128293106
- RheeCKKimKYoonHKNatural course of early COPDInt J Chron Obstruct Pulmon Dis20171266366828255237
- FletcherCPetoRThe natural history of chronic airflow obstructionBr Med J19771607716451648871704
- AnthonisenNRSkeansMAWiseRALung Health Study Research GroupThe effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trialAnn Intern Med200514223323915710956
- Soler-CataluñaJJMartínez-GarcíaMARomán SánchezPSalcedoENavarroMOchandoRSevere acute exacerbations and mortality in patients with chronic obstructive pulmonary diseaseThorax2005601192593116055622
- DonaldsonGCSeemungalTABhowmikAWedzichaJARelationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary diseaseThorax2002571084785212324669
- DecramerMDahlRKornmannOKornSLawrenceDMcBryanDEffects of long-acting bronchodilators in COPD patients according to COPD severity and ICS useRespir Med2013107222323223219347
- WelteTChapmanKRMagnussenHMiravitllesMCurrent thinking and new paradigm for COPDRespir Med201611212612726895809
- ArielAAltrajaABelevskiyAInhaled therapies in patients with moderate COPD in clinical practice: current thinkingInt J Chron Obstruct Pulmon Dis201813455629317810
- MaltaisFDennisNChanCKRationale for earlier treatment in COPD: a systematic review of published literature in mild-to-moderate COPDCOPD20131017910323272663
- QaseemAWiltTJWeinbergerSEAmerican College of Physicians; American College of Chest Physicians; American Thoracic Society; European Respiratory SocietyDiagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory SocietyAnn Intern Med2011155317919121810710
- van den BoomGRutten-van MölkenMPTirimannaPRvan SchayckCPFolgeringHvan WeelCAssociation between health-related quality of life and consultation for respiratory symptoms: results from the DIMCA programmeEur Respir J199811167729543272
- d’AndiranGSchindlerCLeuenbergerPThe absence of dyspnoea cough and wheezing. A reason for undiagnosed airflow obstruction?Swiss Med Wkly200613642543316862462
- ShinCLeeSAbbottRDRespiratory symptoms and undiagnosed airflow obstruction in middle-aged adults: the Korean Health and Genome StudyChest200412641234124015486387
- LuMYaoWZZhongNSAsymptomatic patients of chronic obstructive pulmonary disease in ChinaChin Med J (Engl)2010123121494149920819499
- BrandPLRijckenBSchoutenJPKoëterGHWeissSTPostmaDSPerception of airway obstruction in a random population sample. Relationship to airway hyperresponsiveness in the absence of respiratory symptomsAm Rev Respir Dis199214623964011489130
- van der MolenTWillemseBWSchokkerSTen HackenNHPostmaDSJuniperEFDevelopment, validity and responsiveness of the Clinical COPD QuestionnaireHealth Qual Life Outcomes200311312773199
- CazzolaMBrusascoVCentanniSProject PriMo: sharing principles and practices of bronchodilator therapy monitoring in COPD: a consensus initiative for optimizing therapeutic appropriateness among Italian specialistsPulm Pharmacol Ther201326221822823147424
- CazzolaMSantusPCastagnaFAddition of an extra dose of salmeterol Diskus to conventional dose of salmeterol Diskus in patients with COPDRespir Med200296643944312117044
- MakGHananiaNANew bronchodilatorsCurr Opin Pharmacol201212323824522445544
- CazzolaMTashkinDPCombination of formoterol and tiotropium in the treatment of COPD: effects on lung functionCOPD20096540441519863370
- CazzolaMMolimardMThe scientific rationale for combining long-acting beta2-agonists and muscarinic antagonists in COPDPulm Pharmacol Ther201023425726720381630
- ÁghTInotaiAMészárosÁFactors associated with medication adherence in patients with chronic obstructive pulmonary diseaseRespiration201182432833421454953