Abstract
Chronic obstructive pulmonary disease (COPD) is a common disease in the general population and it places a considerable burden on patients, with the disease negatively affecting quality of life. In practice, patients with COPD generally seek medical attention because of symptoms, particularly breathlessness, and the resulting physical limitations, which affect the health-related quality of life (HR-QOL) in patients. The defining feature of COPD is airflow limitation that causes air trapping and increased hyperinflation as the ventilation rate increases during physical effort. Hyperinflation causes or worsens breathlessness as breathing becomes inefficient, with the end result being an avoidance of physical exertion and a cycle of increasing dyspnea caused by inactivity and deconditioning, with deleterious effects on HR-QOL. Current published guidelines for COPD state that the goals of pharmacologic therapy should be to control symptoms, improve health status and exercise tolerance, and reduce the frequency of COPD exacerbations. Effective and sustained bronchodilation has emerged as a key strategy for improving dyspnea and ability to exercise. As there is no cure for COPD, a major goal of treatment and of research into new therapies is to improve HR-QOL in COPD patients.
Conclusion
More recently, indacaterol, an inhaled ultra-long-acting β2-agonist (24-hour action), has been approved in many countries at different doses (between 75 and 300 μg once daily) for treatment of patients with stable but symptomatic COPD. The aim of this review was to explore once-daily indacaterol clinical data as related to improvement in HR-QOL in COPD. Indacaterol studies have shown significant improvements in lung function of COPD patients, and these improvements have also translated into clinically meaningful improvements in patient symptoms and HR-QOL.
Introduction
Subjective indicators (based on self-rating) of quality of life (QOL) and health-related quality of life (HR-QOL) are increasingly incorporated in chronic obstructive pulmonary disease (COPD) because of the recognition of the importance of patient satisfaction and how patients with chronic disease feel, rather than how statistics imply these patients ought to feel. An American Lung Association survey states that half (51%) of all COPD patients say their condition limits their ability to work. The condition also limits COPD patients in normal physical exertion (70%), household chores (56%), social activities (53%), sleeping (50%), and family activities (46%).Citation1
Although forced expiratory volume in 1 second (FEV1) is a measurement of lung function, because COPD is a progressively worsening disease, improvement in lung function can be transitory and not always indicative of symptoms improvement.Citation2 It appears that improvements in patient-centered outcomes such as dyspnea and health status may better reflect the effectiveness of the particular pharmacotherapy.Citation3,Citation4 The concept of HR-QOL and its determinants in clinical trials have evolved to encompass those aspects of QOL that can be clearly shown to affect health, either physical or mental.Citation5 In relation to health, health status is increasingly referred to as QOL, and, in order to narrow down the term’s operationalization in research studies, QOL is increasingly referred to as HR-QOL. Similar to subjective health status, HR-QOL is patient based; however, HR-QOL focuses more on the impact of a perceived health state on the patient’s ability to live a fulfilling life.Citation6
The traditional approach to the diagnosis, staging, and treatment of COPD was based primarily on the percentage of predicted FEV1 and the rate of decline in FEV1. Previous recommendations for management of COPD were based solely on spirometric category. FEV1, while an important marker, is far from being the only measure available to characterize patients with COPD. In light of considerable cumulative evidence that the level of FEV1 is a poor descriptor of the disease status, Global Initiative for Chronic Obstructive Lung Disease guidelinesCitation7 have incorporated a strategy that considers both disease impact (determined mainly by symptoms burden and activity limitations) and future risk of disease progression (especially of exacerbations).Citation7 Since the health status of patients with COPD is reported to be only weakly associated with spirometric values such as FEV1, measures of HR-QOL are increasingly used for evaluating the efficacy of bronchodilator medications in patients with COPD. Dyspnea, a key symptom in COPD, has been found to be strongly negatively associated with health status and to have the highest correlations with health status questionnaires.Citation8–Citation10 However, dyspnea is a subjective measure that poorly correlates with objective assessments of lung function, exercise capacity, and other outcomes. The other significant factors that determine QOL/health status in COPD patients are mood disorders (anxiety and depression) and exercise tolerance are all directly related to the disease – such as dyspnea and other symptoms – this will automatically result in these strong associations.Citation11
Comprehensive assessment of the effects of COPD requires a battery of instruments that tap not only the disease-specific effects but also the overall burden of the disease on everyday functioning and emotional well-being. Health status as a concept of high complexity is assessed indirectly and requires the application of specially designed questionnaires. The most widely used instruments in studies addressing effects of pharmacologic treatment of COPD on HR-QOL are the Baseline Dyspnea Index (BDI) and the Transitional Dyspnea Index (TDI) for measuring breathlessness and the St George Respiratory Questionnaire (SGRQ) to assess the effects of bronchodilators on health status in COPD.Citation12 The SGRQ is universally administered in COPD trials to measure improvements in HR-QOL. The use of an as-needed short-acting rescue inhaler (eg, salbutamol) has also become a quasi-standard measurement of symptom control in COPD trials. Additional outcomes of interest in clinical practice for management of COPD patients include mortality, hospitalizations, pneumonia, medication tolerability, and symptoms (especially exacerbations).
Indacaterol
The current standard of care for COPD patients is usually stepwise and is generally guided by disease severity. Current guidelines recommend treatment with one or more long-acting bronchodilators for patients with moderate or more severe disease.Citation7 In clinical practice, bronchodilators are used for symptomatic relief in COPD patients with all stages of severity and on the basis of long-term improvements that can be achieved in clinical outcomes such as dyspnea, health status, and exacerbations. Indacaterol is the first ultra-long-acting β2-agonist (LABA) approved that has a 24-hour bronchodilatory effect, allowing for once-daily administration.
Indacaterol was first introduced throughout the European Union in 2009 at doses of 150 and 300 μg doses. In July 2011, indacaterol was also approved for use in the United States, but at a lower once-daily dose of 75 μg. The US Food and Drug Administration (FDA) approval of indacaterol was based on six phase III, randomized, double-blind trials: INLIGHT 1, INLIGHT 2, INVOLVE, INHANCE, INTENSITY, INSIST, and INDORSE (an extension of INHANCE).Citation13–Citation19 The designs of the six studies, plus the extension, are summarized in . Inclusion criteria were similar through each trial; patients were over 40 years old, with moderate to severe COPD and with at least a 10-pack-year smoking history. Short-acting β2-agonist (SABA) rescue medication and inhaled corticosteroids were permitted throughout all trials. A new drug application for indacaterol was submitted to the FDA in 2009; however, the drug was not approved at that time because a meaningful difference in efficacy between the proposed doses of 150 and 300 μg and a lower dose of 75 μg could not be discerned and because of concerns regarding safety with higher doses. To better delineate dose response at a lower dosage, the FDA requested the study in patients with asthma, a condition that is more responsive to bronchodilators than COPD. In addition to dose-ranging studies in asthma, the sponsor provided a second dose-ranging trial in patients with COPD and separate 12-week confirmatory trials using the 75 and 150 μg doses. In both the asthma and the COPD dose-ranging studies, there was no clear separation between 75 and 150 μg doses in the FEV1 time profile. As for the noncomparative confirmatory trials, both 75 and 150 μg doses had significantly higher trough FEV1 values than placebo. Because these studies did not directly compare the two doses, it is difficult to conclude whether the 150 μg dose is more effective than the 75 μg dose.Citation20–Citation22 As a result, the FDA supported approval of the 75 μg dose, based on the FDA’s own overall risk-benefit assessment. The primary efficacy outcome reported in all six studies was the difference in least squares mean trough FEV1 at 24 hours after 12 weeks of treatment. FEV1 is an important measurement in diagnosing and staging COPD. It is also commonly used in COPD clinical trials because it is an objective, reproducible measurement of lung function.
Table 1 Pivotal trials of 12 weeks in duration or longer
The secondary outcome of interest to the FDA was the change from baseline in the SGRQ score. The FDA based approval of indacaterol on these two outcomes only. Because the FDA and the sponsor could not reach an agreement on the definition of “exacerbation,” this important outcome was not included in the FDA approval process.Citation22 Because dyspnea is the key symptom of COPD and the need for rescue medication use is driven by dyspnea episodes, the data from the clinical development of indacaterol (eg, comparisons with active controls or scores on the BDI and the TDI) may have been weighed differently by the European Medicines Agency.Citation21 Doses equal to or greater than 150 μg daily make up the majority of the available clinical data. Only 449 patients were exposed to the FDA-approved dose of 75 μg daily for up to 3 months.
Indacaterol data for health status/HR-QOL
The author has reviewed clinical evidence from the six indacaterol COPD studies mentioned earlier.Citation13–Citation19 The studies compared indacaterol with placebo, and inhaled tiotropium, salmeterol, or formoterol monotherapy. Indacaterol, along with all other bronchodilators, showed a statistically significant reduction in dyspnea compared with placebo. Importantly, improvements in lung function have translated into correspondingly beneficial effects on patient-reported outcomes, such as dyspnea, number of days with poor control, and clinically meaningful improvements in HR-QOL, particularly when comparisons are made with placebo.Citation23
Breathlessness
The TDI was used to assess relief of dyspnea. The BDI and the TDI are validated clinical ratings that describe symptoms at a single point in time (eg, baseline) and measure changes in breathlessness from this baseline state over time, using a seven-point scale from −3 (major deterioration) to +3 (major improvement). TDI ratings are obtained in the course of an interview conducted by an experienced observer, with the observer asking open-ended questions about the patient’s experience of breathlessness during everyday activities that are then translated into numerical values. A change of one point is considered to be the minimum clinically important difference (MCID).Citation24,Citation25
Interviewer blinding to patients’ clinical status is necessary to prevent assessment bias. Mahler et alCitation26 demonstrated for the first time that dyspnea ratings (including the TDI) were significantly related to the stage of disease severity based on the percentage of predicted FEV1. Indacaterol significantly improved dyspnea (measured by the TDI) compared with placebo.Citation14–Citation16 In general, indacaterol appeared to have greater effects on most COPD symptoms than open-label tiotropium, formoterol, or salmeterol, although differences between indacaterol and active comparators were not consistently statistically significant. Indacaterol subjects showed a 43% greater likelihood than tiotropium subjects of experiencing an MCID in the TDI of one point or higher (62% of indacaterol patients versus 52% of tiotropium patients).Citation27 Tiotropium was used as an open-label comparator, thus introducing bias and limiting results interpretation. Nevertheless, when indacaterol was compared with tiotropium in blinded fashion in a study published by Buhl et al,Citation17 indacaterol yielded greater improvements in TDI and SGRQ total scores than tiotropium.
Percentage of days with no rescue medication
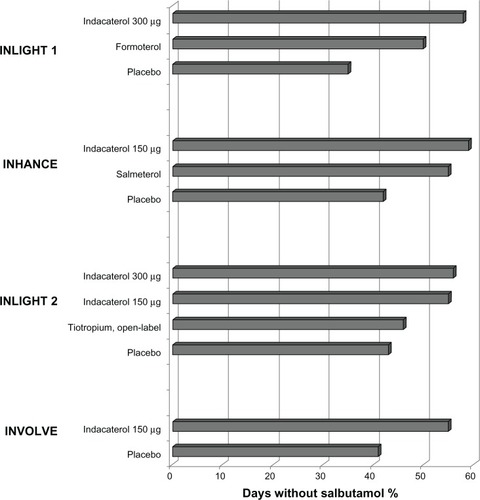
The use of salbutamol because of severity and/or frequency of COPD symptoms experienced by the patients serves as an indirect measure of how effective the study treatments are in controlling these symptoms. The percentage of days with no rescue medication was significantly higher in the indacaterol groups than in the active comparator groups in four studies ().Citation13–Citation16 Indacaterol (both 150 and 300 μg doses) and formoterol recipients had significantly more days with no use of rescue medication than open-label tiotropium recipients in pooled analyses of 3-monthCitation28 and 6-month data.Citation29 In addition to the four large (n > 400) placebo-controlled long-term indacaterol studies (), significantly more patients receiving indacaterol had less need for a rescue inhaler (salbutamol) than salmeterol recipients over 12 weeks in the INSIST (Indacaterol: investigating superiority vs salmeterol) study.Citation18
Figure 1 Effect of treatment on use of as-needed salbutamol, averaged over the period of the studies, as percentage of days without use of salbutamol.
Use of an as-needed rescue inhaler (salbutamol)
Use of an as-needed short-acting rescue inhaler (salbutamol) has become a standard measure of symptom control in COPD trials. Rodrigo et al have conducted post hoc analysis of the five pivotal indacaterol studies.Citation13–Citation16,Citation18 When compared with placebo, indacaterol significantly reduced the number of puffs per day of the rescue inhaler. Patients in the indacaterol group used less as-needed salbutamol, when compared with twice-daily LABA treatment, with a decrease of approximately one and a half puffs per day from baseline, although probably without clinical significance.Citation23 Although use of a SABA in COPD during treatment with a LABA is recommended as needed, its effectiveness is unclear. To the best of the author’s knowledge, no clinical data have been reported to date about the effects of acute SABA administration on top of regular use of indacaterol in COPD treatment. The design of all phase III indacaterol COPD studies has included only stable patients. La Piana et al’sCitation30 observational study, using a SABA on top of formoterol in patients with stable COPD, did not demonstrate improvement in FEV1 or peak expiratory flow after either acute or chronic treatment with formoterol. However, the authors concluded that the results of the study suggest a SABA was still effective in possibly reducing air trapping, as was demonstrated by the increase in forced vital capacity in the study.Citation30
HR-QOL
Health status as a concept of high complexity is assessed indirectly and requires the application of specially designed questionnaires. The SGRQ has been widely used in clinical trials as a secondary end point to assess the effects of bronchodilators on health status in COPD and it has been demonstrated to be valid, reliable, and responsive among patients with COPD.Citation31 The SGRQ is completed by the patient and has 50 questions covering three areas – symptoms, activity, and disease effects – summed to provide a total score of between zero (best) and 100 (worst). The instrument is time-consuming to implement and is therefore of limited applicability in day-to-day clinical practice. The SGRQ covers domains of symptoms (frequency and severity of respiratory symptoms), activity (effects on and adjustment of everyday activities), and psychosocial impact, from which a total score with a possible maximum of 100 points is calculated. A zero score indicates no impairment of QOL. The threshold for a MCID is a four-unit decrease in total SGRQ score. For example, a change of this size would occur in a patient who reports that he or she no longer takes so long to wash or dress, can walk up stairs without stopping, and is able to leave the house for shopping or entertainment.Citation32,Citation33 The SGRQ was used to assess HR-QOL in three studies.Citation14–Citation16 Significant improvements in HR-QOL were seen with indacaterol as compared with placebo, evidenced by statistically significantly lower (ie, better) mean SGRQ total scores at end-of-study assessments. Clinically important improvements (four points or greater) versus placebo were observed for indacaterol recipients.
Exercise endurance and lung hyperinflation
Limitation in exercise capacity represents an important feature of COPD and is one of the main factors that negatively affect the QOL in patients.Citation34 Reduced exercise capacity is considered to be a consequence of airflow obstruction primarily because of dynamic hyperinflation occurring during exercise.Citation35 Limited physical activity of patients with COPD, although a result of the disease, at the same time promotes worsening and progression of the disease and further decline in the patient’s HR-QOL. Consequently, exercise testing is increasingly being used in the functional and HR-QOL assessment of COPD patients and their response to bronchodilators. The possible methods of assessment of exercise capacity are field tests (6-minute and shuttle walking tests) and cardiopulmonary exercise testing (CPET).
CPET is considered the gold standard for studying a patient’s level of exercise limitation and its causes. O’Donnell et alCitation36 undertook a study designed to assess the effect of indacaterol 300 μg once daily (dose not approved in the United States) on exercise endurance in patients with moderate to severe COPD using CPET.Citation36 Indacaterol provided clinically meaningful improvements in exercise endurance with sustained reductions in lung hyperinflation both at rest and at the end of exercise. The authors postulated that the overall improvement in exercise capacity achieved with indacaterol at 300 μg once daily in the study may be an explanation for the improved health status (assessed using the SGRQ) seen with indacaterol in long-term studies.Citation15,Citation16
Mroz et al’sCitation37 study of 34 patients with COPD used the 6-minute walking distance test to assess the impact of indacaterol add-on therapy on lung function, exercise tolerance, and QOL. This 3-month study showed that the patients’ QOL changed favorably in the indacaterol treatment arm, even though the FEV1 did not change significantly in the indacaterol group.Citation37
Exacerbations of COPD
Exacerbations of COPD indicate clinical instability and progression of the disease and are associated with reduced health status, physical and physiologic deterioration, and an increased risk of morbidity and mortality.Citation38,Citation39 The prevention or reduction of exacerbations thus constitutes a major treatment goal. Although exacerbations are an important problem in COPD and a target of intervention, there is no universally standardized tool for assessing the frequency, severity, and duration of exacerbations. Health care databases and patient-based verification by interview, or prospectively from diary cards completed by patients, are the tools available for recording exacerbation rates during trials. Seasonal variations in exacerbation frequency usually require long-term studies of at least 1 year in duration.Citation40 Analysis of time to first COPD exacerbation at 6 months has shown a reduced risk relative to placebo for indacaterol 150 μg. Similarly, the rate of exacerbation relative to placebo has been shown to be lower for indacaterol 150 μg but not for indacaterol 300 μg or tiotropium.Citation16 Subjects with moderate to severe COPD who completed the 26-week INHANCE study were eligible for enrollment in an extension of the trial, during which double-blind treatment with indacaterol, 150 or 300 μg once daily, or placebo was continued for a further 26 weeks.Citation19 Indacaterol treatment over this 12-month extension was accompanied by significant reductions in COPD exacerbations. However, indacaterol trials were not designed to measure exacerbations as the primary outcome, and all studies have only included stable patients without history of frequent exacerbations.
Discussion
The understanding of the merits and limitations of current methods for assessing physiological and clinical outcomes of COPD is crucial for the interpretation and design of clinical trials. Unfortunately, in contrast to spirometric category, there is no gold standard for measuring health status/HR-QOL, physical capacity for activities of daily living, and exacerbations, as none of the available methods is optimal in all regards.Citation39 Nevertheless, there is considerable evidence that HR-QOL is a valid and important measure of the disease’s effect and activity.Citation11 Therefore, it is fundamental that the study question be answerable by the study design. Since the relationship between spirometry, symptoms, and health status appears to be poor, measures of lung physiology alone may not adequately describe both the social impact of COPD and the effectiveness of therapeutic interventions.Citation7
Indacaterol is a novel inhaled ultra-LABA providing 24-hour bronchodilation on once-daily dosing and is now approved in many countries for the management of patients with COPD. Indacaterol studies have shown significant improvements in lung function that, importantly, have translated into correspondingly beneficial effects on patient-reported outcomes such as dyspnea, number of days with poor control, and clinically meaningful improvements in HR-QOL as measured by the SGRQ, particularly when comparisons are made with placebo. Dyspnea is the primary reason for patients seeking medical care, and its measure may provide an insight into the practical effects of treatment on everyday life, reflecting whether or not patients perceive an improvement in this primary symptom of COPD. Results showed the sustained bronchodilator effect of indacaterol was accompanied by significant improvements in dyspnea and health status/HR-QOL when compared with placebo.Citation23 Indacaterol was statistically superior to twice-daily LABAs (salmeterol and formoterol) in terms of exceeding the MCID in dyspnea BDI and TDI measurements. Indacaterol was also shown to be at least as effective as tiotropium in improving dyspnea and health status scores in indacaterol studies that included patients with mostly moderate to severe COPD.Citation17,Citation23
An important finding in phase III studies is that treatment with indacaterol showed in disease control, since sustained bronchodilation provided by indacaterol was associated with a 40% increase in rescue-free days compared with placebo. This meaningful reduction in salbutamol use for symptom relief characterized all indacaterol studies, suggesting that patients were experiencing fewer symptoms.Citation41 The beneficial effects of indacaterol on breathlessness and health status suggest that the overall results of the indacaterol trials provide a useful guide to the level of efficacy that may be expected in milder patients who may be seen predominantly in a primary care patient population.Citation27
Additionally, a new pooled analysis from three randomized studies (INVOLVE, INHANCE, and INLIGHT 2) in the indacaterol clinical trial program, INERGIZE, presented at the annual 2012 European Respiratory Society Congress in Vienna, Austria, showed that indacaterol 300 μg was superior to tiotropium in improving breathlessness in COPD patients who had more severe breathlessness symptoms on entry to the studies.Citation42 Unfortunately, COPD is a progressive disease and often more therapies, with different mechanisms of action, are added in order to control symptoms and improve QOL. Recently, two studies investigating the approach of dual bronchodilation using indacaterol (150 μg) and tiotropium, compared with tiotropium alone, produced a significantly greater improvement in lung function than the tiotropium alone in patients with COPD.Citation43 Sponsor Novartis introduced indacaterol in 2009. Novartis also added an investigational long-acting muscarinic antagonist, glycopyrronium bromide (NVA237), developed as once-daily inhaled maintenance therapy for the treatment of COPD. The results of phase III IGNITE data presented at the 2012 European Respiratory Society Congress demonstrated the efficacy of dual bronchodilation with indacaterol and glycopyrronium bromide (QVA149) and showed a superior effect on lung function and patient-reported outcomes versus all comparators used as monotherapy (placebo, indacaterol alone, glycopyrronium bromide alone, and tiotropium). QVA149 improved breathlessness as measured by the TDI, increased HR-QOL as measured by the SGRQ, and reduced rescue medication use.Citation44 These results provide further support to current guidelines, which recommend use of one or more bronchodilators of different classes for treating moderate to severe disease.Citation7 Additional studies assessing the impact of indacaterol and/or combination therapies such as a long-acting muscarinic antagonist and a LABA on COPD exacerbations, using a standardized definition of an exacerbation, are clearly needed.
Conclusion
Indacaterol is the first ultra-long-acting β2-agonist (LABA) approved that has a 24-hour bronchodilatory effect. Indacaterol studies have shown significant improvements in lung function that, importantly, have translated into correspondingly beneficial effects on patient-reported outcomes such as dyspnea, number of days with poor control, and clinically meaningful improvements in HR-QOL. Recent studies also suggest that dual bronchodilation with indacaterol in combination with long-acting muscarinic antagonists provide an additive impact on improving HR-QOL in patients with moderate to severe COPD with important implication for COPD management.
Disclosure
The author reports no conflicts of interest in this work.
References
- Chronic obstructive pulmonary disease (COPD) fact sheet [webpage on the Internet]Washington DCAmerican Lung Association2011 Available from: http://www.lung.org/lung-disease/copd/resources/facts-figures/COPD-Fact-Sheet.htmlAccessed September 14, 2012
- National Clinical Guideline CenterChronic Obstructive Pulmonary Disease: Management of Chronic Obstructive Pulmonary Disease in Adults in Primary and Secondary CareLondonNational Clinical Guideline Center2010 Available from: http://guidance.nice.org.uk/CG101/Guidance/pdf/EnglishAccessed November 14, 2012
- JonesPWAgustiAGOutcomes and markers in the assessment of chronic obstructive pulmonary diseaseEur Respir J200627482283216585091
- CazzolaMMacNeeWMartinezFJAmerican Thoracic Society; European Respiratory Society Task Force on outcomes of COPDOutcomes for COPD pharmacological trials: from lung function to biomakersEur Respir J200831241646918238951
- Centers for Disease Control and PreventionMeasuring Healthy Days: Population Assessment of Health-Related Quality of LifeAtlanta, GACenters for Disease Control and Prevention2000 Available from: http://www.cdc.gov/hrqol/pdfs/mhd.pdfAccessed November 14, 2012
- BullingerMAndersonRCellaDAaronsonNDeveloping and evaluating cross-cultural instruments from minimum requirements to optimal modelsQual Life Res1993264514598161979
- Global Initiative for Chronic Obstructive Lung Disease (GOLD)Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary DiseaseGOLD; revised2011 Available from: http://www.Goldcopd.comAccessed September 14, 2012
- MahlerDAHow should health-related quality of life be assessed in patients with COPD?Chest2000117Suppl 2S54S57
- ReardonJZLareauSCZuWallackRFunctional status and quality of life in chronic obstructive pulmonary diseaseAm J Med200611910 Suppl 1323716996897
- Martín A, Rodríguez-González Moro JM, Izquierdo JL, Gobartt E, de Lucas P; VICE Study Group. Health-related quality of life in outpatients with COPD in daily practice: the VICE Spanish studyInt J Chron Obstruct Pulmon Dis20083468369219283915
- TsiligianniIKocksJTzanakisNSiafakasNvan der MolenTFactors that infuence disease-specific quality of life or health status in patients with COPD: a review and meta-analysis of Pearson correlationsPrim Care Respir J201120325726821472192
- JonesPWQuirkFHBaveystockCMLittlejohnsPA self-complete measure of health status for chronic airflow limitation: the St George’s Respiratory QuestionnaireAm Rev Respir Dis19921456132113271595997
- FeldmanGSilerTPrasadNINLIGHT-1study groupEfficacy and safety of indacaterol 150 microg once-daily in COPD: a double-blind, randomised, 12-week studyBMC Pulm Med2010101120211002
- KornmannODahlRCentanniSINLIGHT-2 study investigatorsOnce-daily indacaterol versus twice-daily salmeterol for COPD: a placebo-controlled comparisonEur Respir J201137227327920693243
- DahlRChungKFBuhlRINVOLVE study investigatorsEfficacy of a new once-daily long-acting inhaled beta2-agonist indacaterol versus twice-daily formoterol in COPDThorax201065647347920522841
- DonohueJFFogartyCLötvallJHANCE study investigatorsOnce-daily bronchodilators for chronic obstructive pulmonary disease: indacaterol versus tiotropiumAm J Respir Crit Care Med2010182215516220463178
- BuhlRDunnLJDisdierCINTENSITY study investigatorsBlinded 12-week comparison of once-daily indacaterol and tiotropium in COPDEur Respir J201138479780321622587
- KornSKerwinEAtisSAmosCOwenRLassenCINSIST study groupIndacaterol once-daily provides superior efficacy to salmeterol twice-daily in COPD: a 12-week studyRespir Med2011105571972621367594
- ChapmanKRRennardSIDograAOwenRLassenCKramerBINDORSE study investigatorsLong-term safety and efficacy of indacaterol, a long-acting β2-agonist, in subjects with COPD: a randomized, placebo-controlled studyChest20111401687521349928
- VA Pharmacy Benefits Management Services, Medical Advisory Panel, VISN Pharmacist ExecutivesIndacaterol (Arcapta™ Neohaler™): National Drug MonographWashington DCUS Department of Veterans Affairs2012 Available from: http://www.pbm.va.gov/Clinical%20Guidance/drug%20Monographs/Indacaterol.pdfAccessed November 14, 2012
- ChowdhuryBASeymourSMMicheleTMDurmowiczAGLiuDRosebraughCJThe risks and benefits of indacaterol: the FDA’s reviewN Engl J Med2011365242247224922168640
- US Food and Drug AdministrationIndacaterol FDA Summary Review Available from: http://www.accessdata.fda.gov/drugsatfda_docs/nda/2011/022383Orig1s000SumR.pdfAccessedFebuary 2 2013
- RodrigoGJNeffenHComparison of indacaterol with tiotropium or twice-daily long-acting beta-agonists for stable COPD: a systematic reviewCHEST201214251104111022383666
- MahlerDAWitekTJJrThe MCID of the transition dyspnea index is a total score of one unitCOPD2005219910317136969
- WitekTJJrMahlerDAMinimal important difference of the transition dyspnoea index in a multinational clinical trialEur Respir J200321226727212608440
- MahlerDAWardJWatermanLAMcCuskerCZuwallackRBairdJCPatient-reported dyspnea in COPD reliability and association with stage of diseaseChest200913661473147919696126
- JonesPWBarnesNVogelmeierCLawrenceDKramerBEfficacy of indacaterol in the treatment of patients with COPDPrim Care Respir J201120438038821785813
- SilerTMWilliamsJYegenUOwenRLassenCKramerBThe effect of once-daily indacaterol on health-related quality of life, rescue medication use, and exacerbation rates in patients with moderate-to-severe COPD: a pooled analysis of three months of treatmentAm J Respir Crit Care Med2010181A4430
- KleerupEWilliamsJYegenUOwenRLassenCKramerBThe effect of indacaterol once-daily on health-related quality of life, symptoms and rescue medication use in moderate-to-severe chronic obstructive pulmonary disease: pooled analysis of six monthAm J Respir Crit Care Med2010181A4429
- La PianaGECordaLBertellaETaranto MontemurroLPiniLTantucciCDose-responsive curve to salbutamol during acute and chronic treatment with formoterol in COPDInt J Chron Obstruct Pulmon Dis2011639940521857779
- JonesPWQuirkFHBaveystockCMThe St George’s Respiratory QuestionnaireRespir Med199185Suppl B25311759018
- JonesPWHealth status measurement in chronic obstructive pulmonary diseaseThorax2001561188088711641515
- JonesPWInterpreting thresholds for a clinically significant change in health status in asthma and COPDEur Respir J200219339840411936514
- EstebanCQuintanaJMAburtoMImpact of changes in physical activity on health-related quality of life among patients with COPDEur Respir J201036229230020075059
- PalangePWardSACarlsenKHERS Task ForceRecommendations on the use of exercise testing in clinical practiceEur Respir J200729118520917197484
- O’DonnellDECasaburiRVinckenWINABLE 1study groupEffect of indacaterol on exercise endurance and lung hyperinflation in COPDRespir Med201110571030103621498063
- MrozRMMinarowskiLChyczewskaEIndacaterol add-on therapy improves lung function, exercise capacity and life quality of COPD patientsAdv Exp Med Biol2013756232822836615
- GlaabTVogelmeierCBuhlROutcome measures in chronic obstructive pulmonary disease (COPD): strengths and limitationsRespir Res2010117920565728
- AnzuetoASethiSMartinezFJExacerbations of chronic obstructive pulmonary diseaseProc Am Thorac Soc20074755456417878469
- BurgeSWedzichaJACOPD exacerbations: definitions and classificationsEur Respir J Suppl200341S46S53
- PartridgeMRMiravitllesMStåhlEKarlssonNSvenssonKWelteTDevelopment and validation of the Capacity of Daily Living during the Morning questionnaire and the Global Chest Symptoms Questionnaire in COPDEur Respir J20103619610419897551
- MahlerDABuhlRLawrenceDMcBryanDEffectiveness of indacaterol and tiotropium in patients with severe dyspneaEuropean Respiratory Society CongressSeptember 1–5, 2012Vienna, Austria ERS abstract 850630, session 245
- MahlerDAD’UrzoAPeckittCLassenCKramerBFilcekSConcurrent Use of Indacaterol Plus Tiotropium in Patients with COPD Provides Superior Bronchodilation Compared with Tiotropium AloneThorax201267978178822544891
- BatemanEFergusonGTBarnesNBenefits of dual bronchodilation with QVA149 once daily versus placebo, indacaterol, NVA237 and tiotropium in patients with COPD: the SHINE studyEuropean Respiratory Society CongressSeptember 1–5, 2012Vienna, Austria ERS abstract 700179, session 306