
Abstract
Purpose
Home mechanical ventilation (HMV) use in chronic obstructive pulmonary disease (COPD) is becoming increasingly widespread. The aim of this study was to provide an accurate description of the current practices and clinical characteristics of COPD patients on HMV in Portugal.
Methods
The study was designed as a cross-sectional, multicenter real-life study of COPD patients established on HMV for at least 30 days. Data related to clinical characteristics, adaptation and ventilatory settings were collected.
Results
The study included 569 COPD patients on HMV from 15 centers. The majority were male, with a median age of 72 years and a high prevalence of obesity (43.2%) and sleep apnea (45.8%). A high treatment compliance was observed (median 8h/day), 48.7% with inspiratory positive airway pressure ≥20 cmH2O and oronasal masks were the preferred interface (91.7%). There was an equal distribution of patients starting HMV during chronic stable condition and following an exacerbation. Patients in stable condition were initiated in the outpatient setting in 92.3%. Despite the differences in criteria and setting of adaptation and a slightly lower BMI in patients starting HMV following an exacerbation, we found no significant differences regarding age, gender, ventilation pressures, time on HMV, usage, severity of airflow obstruction or current arterial blood gas analysis (ABGs) in relation to patients adapted in stable condition.
Conclusion
Patients were highly compliant with the therapy. In agreement with most recent studies and recommendations, there seems to be a move towards higher ventilation pressures, increased use of oronasal masks and an intent to obtain normocapnia. This study shows that chronic hypercapnic and post exacerbation patients do not differ significantly regarding patient characteristics, physiological parameters or ventilatory settings with one exception: chronic hypercapnic patients are more often obese and, subsequently, more frequently present OSA.
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a chronic lung disease characterized by nonreversible airflow obstruction and intermittent exacerbations that in the most advanced stages leads to chronic hypercapnic respiratory failure (CHRF), which adversely affects prognosis. COPD is a leading cause of morbidity and mortality and its burden is predicted to increase in the next decades.Citation1
Home mechanical ventilation (HMV) is indicated in patients with severe chronic respiratory insufficiency of different causes and its utilization in the last decades has been increasing both due to widening indications and to improved healthcare setting organization.Citation2,Citation3
However, the use of HMV in COPD has been subject of some controversy.Citation2,Citation4–Citation6
In Portugal, national recommendations for HMV in COPD have remained largely unchanged over the last two decades.Citation7,Citation8
Due to narrow selection criteria, patients enrolled in randomized controlled trials tend to be quite homogeneous regarding clinical characteristics, despite COPD being a highly heterogeneous disease with multiple phenotypes.Citation9 This might explain the differences between randomized controlled trials (RCTs) conclusions, guidelines and real-life HMV practices in COPD patients.
In the Eurovent survey, Portugal had one of the highest percentages of lung/airway disease patients receiving HMV in Europe – around 50% of an estimated 9.3 ventilated patients per 100,000 inhabitants.Citation10
The aim of this study was to provide an accurate description of the current practices regarding HMV prescription and clinical characteristics of COPD patients in Portugal, and to describe factors that may impact ventilation settings and outcomes.
Methods
Study Design
This study was designed as a cross-sectional multicenter real-life study conducted between October 1st 2019 and April 30th 2020. All forty Portuguese Pulmonology Departments registered in the Portuguese Respiratory Society were invited to participate. The participating centers were instructed to screen all patients with COPD and HMV and include all patients that met the inclusion/exclusion criteria during the study period.
Ethical Approval
Ethical approval was obtained from each center’s Ethics Committee, written consent was obtained from the included patients and data anonymity was guaranteed (Centro Hospitalar de Vila Nova de Gaia/Espinho Ethics Committee nr 75/2019).
Inclusion/Exclusion Criteria
Patients with COPD, as defined by international consensus and state-of-the-art practices,Citation1 established on HMV for at least 30 days were eligible for the study. Exclusion criteria were refusal to participate and use of a continuous positive airway pressure, automatic positive airway pressure or servo-ventilation devices.
Data Collected
A pre-study survey, answered by each investigator, was performed to characterize each center.
Data were recorded through a password-protected secure form with mostly mandatory fields in order to minimize missing values.
Data related to demographic and anthropometric characteristics, criteria and place of initiation of HMV, sleep study results (whenever available, either respiratory polygraphy or polysomnography), integration into rehabilitation programs and evaluation by palliative care teams were obtained from clinical records.
Patients’ autonomy was evaluated by the ability to perform basic daily life activities such as personal hygiene, dressing, going to the toilet, feeding and within house mobility. Patients were considered totally autonomous when they could perform all activities without help, totally dependent when they could perform none and partially dependent when they needed assistance with some of the activities.
Exacerbation was defined as an acute worsening of symptoms that led to a change in pharmacological treatment needing antibiotic and/or corticosteroid use and was recorded retrospectively based on patients’ self-report and hospital records.
Dyspnea was assessed based on the modified Medical Research Council’s (mMRC) dyspnea scale on the inclusion date.
Ventilation parameters and daily usage were recorded by the readout of the ventilators’ built-in software.
Pulmonary function test data was obtained from clinical records in the previous 12 months.
Daytime arterial blood gas (ABGs) analysis was reported without ventilation, under the current prescribed oxygen flow.
No additional investigation was performed.
Statistical Analysis
Descriptive data were expressed as count and percentage for categorical variables and as median and 1st and 3rd quartiles (1Q-3Q) for ordinal or quantitative variables. The chi-square test was used to compare proportions. Normality of quantitative variables was assessed by visual inspection of histograms, and since all variables deviated from normality, Mann–Whitney tests were used to compare distributions between two groups. Statistical computations were performed with IBM SPSS Statistics for Windows, Version 20.0 (Armonk, NY: IBM Corp.). P-values were assumed significant if less than 0.05.
Results
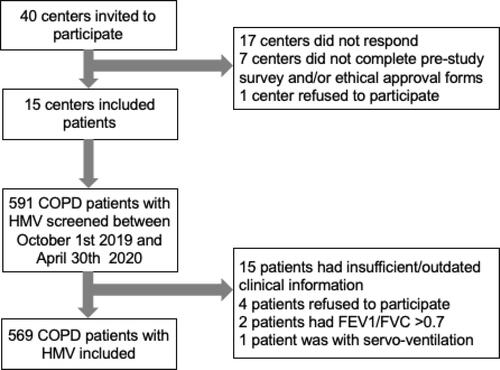
The study included 569 COPD patients established on HMV from 15 centers in Portugal. These centers were located in 5 of the 7 regions in Portugal, covering 90.9% of Portuguese residents according to 2018 data.Citation11 Centers´ characteristics are described in Supplementary Table S1.
There are no official data on the current population of COPD patients on HMV in Portugal. The size of the sample obtained is associated with a margin of error of 3.3% in the estimated proportions based on a recent prevalence study,Citation12 assuming a population of 1520 patients, a confidence of 95%, and an expected proportion of 0.5 (worst scenario) for the characteristic of interest.
Of the 591 patients identified as COPD on HMV during the data collection period, 569 patients were included in this analysis ().
Figure 1 Flow chart.
Study Population
We analyzed 569 COPD patients, 71.5% male, with a median age of 72 years [64–79], 82.9% being former or current smokers. The airway obstruction was very severe in 27.9% (post-bronchodilator FEV1 below 30%) and severe in 43.4% (FEV1 between 30 and 50%).
Patients’ characteristics are described in .
Table 1 Patients’ Characteristics (n=569)
Regarding smoking habits, we found that never smokers (17.1%) were significantly older, had higher body mass index (BMI), higher ventilation pressures and less severe airflow obstruction than ever smokers. Women were more often never smokers (50%) than men (3.9%) and represented 83.5% of the never smoker group. There was no significant difference in months on HMV, usage and current PaCO2 or HCO3 between ever and never smoker groups (supplementary Table S2). Within ever smokers, we found that current smokers were younger and had been established on HMV for a shorter duration.
We found a high prevalence of obesity, with 246 patients (43.2%) with body mass index over 30 kg/m2. In patients with severe or very severe airway obstruction, this prevalence was 31.8%.
When analyzing the differences concerning BMI, we observed that obese patients (BMI ≥ 30 kg/m2) had been longer on HMV, had less severe airflow obstruction, required a higher EPAP, and lower pressure support (PS) and had lower current PaCO2 and HCO3 (Supplementary Table S3).
Data from a diagnostic sleep study were available for 373 patients (65.6% of the entire group). Those with moderate to severe obstructive sleep apnea (n= 172) had a higher BMI, were managed with a higher EPAP and lower pressure support, had less severe airway obstruction and lower current PaCO2 and HCO3 (Supplementary Table S4).
Home Mechanical Ventilation Initiation
About half of the patients started HMV during or immediately after an exacerbation (49.6%), and the remaining in a stable condition. Differences in clinical characteristics, criteria for initiation and HMV adaptation setting between each group are presented in .
Table 2 Differences in Clinical Characteristics, Criteria for Initiation and Adaptation Settings in Patients Started in Stable and Post Exacerbation
When considering differences regarding timing of initiation, we found that patients that started HMV after an acute exacerbation had a slightly lower BMI with no significant differences regarding age, gender, ventilation pressures, time on HMV, current arterial blood gas analysis (ABGs) or severity of airflow obstruction. Never smokers started HMV more commonly after an exacerbation than ever smokers (58.8% vs 47.6%, p=0.02).
The most common criteria to start HMV after an exacerbation was daytime PaCO2 50–54 mmHg plus 2 exacerbations with hypercapnic respiratory failure (HRF) treated with noninvasive ventilation (NIV) in the previous 12 months in 40.4%, failure to wean from NIV in 30.1% and previous PaCO2 above 55 mmHg in 13.8%.
Sleep studies were available more commonly in patients that started HMV in stable condition (77.0 vs 53.9%) and these patients had a higher percentage of moderate to severe OSA (52.5 vs 36.8%). Patients in stable condition were initiated in the outpatient setting in 92.3%.
Ventilation Settings
The most common ventilatory mode was spontaneous-timed (92.3%) and the most common interface was oro-nasal mask (91.7%). Current ventilatory settings are described in .
Table 3 Current Oxygen Requirements and Ventilation Characteristics (n=569)
Regarding time on HMV, patients who had been on ventilation for longer than 6 months had higher ventilator usage, higher ventilation pressures and lower concurrent PaCO2 than patients with HMV for less than 6 months (Supplementary Table S5).
Two hundred and seventy-seven patients (48.7%) had IPAP ≥ 20 cmH2O. These patients had a higher usage of ventilation, were on HMV for a longer period, had more severe airflow obstruction, a higher current PaCO2 and HCO3 and significantly less exacerbations in the previous year (Supplementary Table S6).
Discussion
The study included more than a third of all pulmonology centers registered in the Portuguese Respiratory Society. Although the majority had a specialized HMV outpatient program, there is considerable heterogeneity among centers and geographic areas regarding the number of patients on HMV, the average hours dedicated to outpatient consultation and the percentage of obstructive lung disease patients.
As expected, most patients had current or previous smoking habits. Nevertheless, 17.1% were never smokers (83.5% of which were women). The prevalence of COPD in never smokers in Portugal was estimated to be 9.2% based on a previous study.Citation13 The CanCOLD study found that 27% of COPD patients were never smokers and that a history of hospitalization in childhood for respiratory illness was discriminative, while exposure to passive smoke and biomass fuel for heating were discriminative for women.Citation14 Never smokers in our study were older than ever smokers suggesting the impact of longer exposure to noxious agents other than first-hand smoke. Also, most often their timing of HMV initiation was related to an exacerbation.
A recent study reported that 47% of COPD patients using home NIV were obese with a median BMI of 28 kg/m2.Citation12 The same study also found that 29% of COPD patients had concomitant OSA, which is lower than in our study.Citation12 In patients who underwent a sleep study before initiating HMV (65.6%), we found a prevalence of OSA of 46.2% which is in-line with previous studies performed in Portugal.Citation15,Citation16 Soler et al also found a high prevalence of OSA (65.9%) in patients with moderate to severe COPD.Citation17 These results are considerably different from many RCTs in which presence of obesity or relevant OSA are exclusion criteria for enrolment of COPD patients in HMV studies.Citation4–Citation6
The most common criteria for starting HMV are concordant with current recommendations. Interestingly, criteria related to overlap (COPD+OSA) represent around a quarter of indications for HMV in this population, and these criteria are seldom referred in current guidelines.Citation2,Citation3
Although inpatient adaptation is considered the gold standard for HMV initiation, in our study it was mostly used for patients admitted as a result of exacerbation while stable patients were adapted mainly with daytime titration in outpatient clinics with limited monitoring. Even though around half of the patients were adapted to HMV during an exacerbation, the criteria mostly used was related to previous exacerbations needing NIV/previous stable hypercapnia and failure to wean. This suggests that prescribers often take advantage of the inpatient period and need for NIV in the acute setting in a significant proportion of patients, to adapt them to HMV when they met previous defined criteria. Because of that, this population is different from the Rescue Trial where commencing HMV immediately after an exacerbation needing NIV failed to improve outcomes, despite improving ABGs.Citation6 A recent study found that patients with obstructive airway disease were more likely to have their HMV set up following an acute admission (70%) than other diseases.Citation18
On the other hand, failure to wean from ventilation has also been ranked as second in the importance rating of decisions to start NIV in a European survey on prescribers.Citation19 Failure to wean from NIV was an exclusion criterion for the HOT-HMV trial, that provided the most recent evidence for initiation of HMV after an exacerbation.Citation4 Other studies have suggested it as an important initiation criterium.Citation19,Citation20
The widening indications for HMV in a resources-limited system made exclusive inpatient initiation impracticable in Portugal. Since 2007, some studies have suggested outpatient initiation as a feasible and cost-effective alternative in patients with CHRF.Citation21,Citation22 Recently, Duiverman et al found that home initiation of HMV in stable hypercapnic COPD patients, using telemedicine, was non-inferior to in-hospital initiation, safe and reduced costs by over 50%.Citation23
Our study demonstrates an evenly distributed population of stable chronic hypercapnic and post exacerbation patients. A German study analyzing the feasibility of outpatient follow-up of COPD patients with NIV had a greater proportion of post exacerbation (45%) plus weaning failure (11.2%) than stable elective adaptation.Citation20
Despite the differences in criteria and setting of adaptation and a slightly lower BMI in patients starting HMV following an exacerbation, we found no significant differences regarding age, gender, ventilation pressures, time on HMV, usage, severity of airflow obstruction or current arterial blood gas analysis (ABGs) in relation to patients adapted in stable condition.
Regarding the preferred interface, we found a huge shift from the Eurovent study where the vast majority of countries reported ventilation through a nasal mask in lung HMV users (especially Portugal).Citation10 These findings are in line with recent studies in COPD patients suggesting a change in practice in recent years and it is probably a consequence of the use of higher ventilation pressuresCitation12,Citation23–Citation25 and improved monitoring capacity due to ventilator software readouts.Citation26 In this study population, there were no patients with invasive ventilation via tracheostomy.
Our study demonstrates a high ventilator compliance, with a median of 8 hours a day and the vast majority using it over the 5 hour a day cut-off usually regarded as minimal for clinical impact. This compliance is higher than many relevant clinical trialsCitation4,Citation5 but is consistent with other national studies.Citation15,Citation16,Citation27 The fact that patients on HMV for longer periods of time had higher usage suggests that there might be an adaptation period allowing to minimize potential side effects and initial resistance, an increasing dependence on HMV with disease progression or a dropout of noncompliant patients in the first months of treatment. This increase of compliance over time has also been reported in other studies.Citation16,Citation23
About half of the patients are currently normocapnic with two thirds having PaCO2 below 48 mmHg. This PaCO2 threshold was suggested by Kohnlein et alCitation5 and shown in their large RCT to have a significant impact on mortality and quality of life in COPD patients.
Almost half of the patients are prescribed with IPAP≥20 cmH2O which is usually considered a cut-off value for “high pressure ventilation”.Citation28 High ventilation pressures were used most commonly in patients with more severe obstruction and in those established on HMV for a longer duration. Interestingly, it appears that these higher pressures were well tolerated by patients, with the group prescribed with higher pressures demonstrating a slightly higher (but statistically significant) ventilator usage. Despite the higher IPAP, these patients still have higher PaCO2 (although with a median below 48 mmHg), suggesting that physicians try to titrate pressures to obtain normocapnia, possibly limited by other factors such as patients´ tolerance. These data are consistent with recent guideline recommendations which supports the application of higher pressures to improve health outcomes by targeting a reduction paCO2 in COPD patients.Citation2
Although more than half of the patients were submitted to a respiratory rehabilitation program, only around a quarter participated in the program in the previous year. Very few patients (4%) were evaluated by a palliative care team, even though there is a high percentage of patients with significant dyspnea (36.4% with a mMRC ≥3), high ventilator dependency (10.2% with ventilator usage above 12h) and 13.9% with more than 2 exacerbations in the previous year. Despite efforts from societies, recommendations and evidence of the efficacy of palliative measures, it is admittedly underused in COPD patients.Citation1,Citation29
There might be some potential limitations to this study. Firstly, although it includes a high number of patients from 15 centers, it represents a cross-sectional real-life description of one country and its practices. Nevertheless, most results are in-line with international studies.
Secondly, by not selecting solely patients with very severe airway obstruction, there might be some other potential factors contributing to these patients’ CHRF. In order to reduce this potential contribution, patients with devices used strictly for sleep apnea were excluded as, in these patients, COPD would not be a significant contributor for the need for HMV and all patients met GOLD COPD diagnostic criteriaCitation1 and the authors feel that, instead of a limitation, this might prove to be a valuable asset by representing more accurately the real-life population of COPD patients that need HMV.
In spite of these potential limitations, to the best of our knowledge, this is the largest real-life study describing current practices and clinical characteristics of HMV in COPD patients and its results might be reproducible in other countries. Also, this study convincingly shows that chronic hypercapnic and post exacerbation patients do not differ significantly regarding patient characteristic and physiological parameters with one exception: chronic hypercapnic patients are more often obese and, subsequently, more frequently present OSA, suggesting that in COPD that develop CHRF, a sleep study might be relevant before the adaptation to HMV. The precise relative contribution of obesity on COPD with CHRF requiring HMV requires further study.
Conclusion
In this large cross-sectional study of HMV in COPD patients, the authors describe an heterogenous population with multiple criteria for HMV, half of whom started HMV during or immediately after an exacerbation. Although there are differences in initiation criteria and adaptation setting, these do not translate to significant differences in clinical characteristics, ventilation pressures, compliance, severity of airway obstruction and arterial blood gas analysis (ABGs) between these two groups.
Patients in stable condition were almost exclusively started in the outpatient setting.
We found a high prevalence of obesity and concurrent sleep apnea, especially in patients adapted to HMV in stable condition.
Patients were highly compliant with the therapy. It appears that smoking habits, obesity and sleep apnea impact clinical and ventilatory characteristics of COPD patients.
In agreement with most recent studies and recommendations, there seems to be a move towards higher ventilation pressures, increased use of oronasal masks and an intent to obtain normocapnia.
The authors believe that this work has several clinical and investigation implications. Firstly, a high prevalence of obesity and OSA in COPD patients established on HMV was found. As these patients are usually excluded from RCTs and guidelines, the authors believe that this high prevalence must be taken into consideration and addressed in future interventional studies.
Secondly, the vast majority of patients in stable condition were initiated on the outpatient setting. Since it was not designed as a prospective/interventional study and there was no controlled group, definite conclusions must not be drawn. Nevertheless, these data suggest that this approach may be safe and effective, albeit it needs to be confirmed in an RCT.
And finally, despite different criteria and setting, this study convincingly shows that chronic hypercapnic and post exacerbation patients do not differ significantly regarding patient characteristics and physiological parameters with one exception: chronic hypercapnic patients are more often obese and, subsequently, more frequently present OSA.
Acknowledgments
We would like to thank Daniela Ferreira, Carla Nogueira and Cláudia Freitas for their help in patient recruitment and Ana Oliveira for proof-reading the manuscript.
Disclosure
Dr Carla Ribeiro reports expert speaking fees and non-financial support from Nippon Gases and non-financial support from Vitalaire Portugal, Linde Saúde and Acail Gás, all outside the submitted work. Dr Paula Pamplona reports non-financial support from Linde Saúde, Nippon Gases and VitAlaire Portugal, all outside the submitted work. Dr Pedro Costa reports non-financial support from Linde Healthcare, VitalAire, and Vivisol, outside the submitted work. Dr Teresa Martin reports non-financial support from Linde, outside the submitted work. Prof Dr Wolfram Windisch reports grants and personal fees from companies dealing with mechanical ventilation, during the conduct of the study.
The authors confirm that they have no other potential conflicts of interest associated with this work/publication and that there has been no significant financial support for this work that could have influenced its outcome. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Halpin DMG, Criner GJ, Papi A, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2021;203(1):24–36. doi:10.1164/rccm.202009-3533SO
- Ergan B, Oczkowski S, Rochwerg B, et al. European Respiratory Society guidelines on long-term home non-invasive ventilation for management of COPD. Eur Respir J. 2019;54. doi:10.1183/13993003.01003-2019
- Windisch W, Geiseler J, Simon K, Walterspacher S, Dreher M, on behalf of the Guideline C. German national guideline for treating chronic respiratory failure with invasive and non-invasive ventilation - Revised Edition 2017: part 2. Respiration. 2018;96(2):171–203. doi:10.1159/000488667
- Murphy PB, Rehal S, Arbane G, et al. Effect of home noninvasive ventilation with oxygen therapy vs oxygen therapy alone on hospital readmission or death after an acute COPD exacerbation: a randomized clinical trial. JAMA. 2017;317(21):2177–2186. doi:10.1001/jama.2017.4451
- Köhnlein T, Windisch W, Köhler D, et al. Non-invasive positive pressure ventilation for the treatment of severe stable chronic obstructive pulmonary disease: a prospective, multicentre, randomised, controlled clinical trial. Lancet Respir Med. 2014;2(9):698–705. doi:10.1016/s2213-2600(14)70153-5
- Struik FM, Lacasse Y, Goldstein RS, Kerstjens HA, Wijkstra PJ. Nocturnal noninvasive positive pressure ventilation in stable COPD: a systematic review and individual patient data meta-analysis. Respir Med. 2014;108(2):329–337. doi:10.1016/j.rmed.2013.10.007
- Normas e Recomendações para a Ventiloterapia Domiciliária **Relatório do sub-grupo de Ventiloterapia Domiciliária da Comissão de Trabalho de Reabilitação Respiratória (Coordenação: joão Carlos Winck), aprovado em reunião de trabalho-Lisboa, Novembro 1997. Rev Port Pneumol. 1998;4(5):447–478. doi:10.1016/s0873-2159(15)31068-0
- Cuidados Respiratórios Domiciliários. Prescrição de Ventiloterapia e outros equipamentos. 2015. Available from: https://www.dgs.pt/directrizes-da-dgs/normas-e-circulares-normativas/norma-n-0222011-de-28092011-jpg.asp. Accessed January 10, 2021.
- Han MK, Agusti A, Calverley PM, et al. Chronic obstructive pulmonary disease phenotypes: the future of COPD. Am J Respir Crit Care Med. 2010;182(5):598–604. doi:10.1164/rccm.200912-1843CC
- Lloyd-Owen SJ, Donaldson GC, Ambrosino N, et al. Patterns of home mechanical ventilation use in Europe: results from the Eurovent survey. Eur Respir J. 2005;25(6):1025–1031. doi:10.1183/09031936.05.00066704
- PORDATA. Base de dados de Portugal comtemporâneo. Available from: https://www.pordata.pt/. Accessed January 12, 2021.
- Cantero C, Adler D, Pasquina P, et al. Long-term noninvasive ventilation in the Geneva Lake Area: indications, prevalence, and modalities. Chest. 2020;158(1):279–291. doi:10.1016/j.chest.2020.02.064
- Barbara C, Rodrigues F, Dias H, et al. Chronic obstructive pulmonary disease prevalence in Lisbon, Portugal: the burden of obstructive lung disease study. Rev Port Pneumol. 2013;19(3):96–105. doi:10.1016/j.rppneu.2012.11.004
- Tan WC, Sin DD, Bourbeau J, et al. Characteristics of COPD in never-smokers and ever-smokers in the general population: results from the CanCOLD study. Thorax. 2015;70(9):822–829. doi:10.1136/thoraxjnl-2015-206938
- Ribeiro C, Ferreira D, Conde S, Oliveira P, Windisch W. Validation of the Portuguese Severe Respiratory Insufficiency Questionnaire for home mechanically ventilated patients. Rev Port Pneumol. 2017;23(3):139–145. doi:10.1016/j.rppnen.2017.01.001
- Durao V, Grafino M, Pamplona P. Chronic respiratory failure in patients with chronic obstructive pulmonary disease under home noninvasive ventilation: real-life study. Pulmonology. 2018;24(5):280–288. doi:10.1016/j.pulmoe.2018.02.007
- Soler X, Gaio E, Powell FL, et al. High prevalence of obstructive sleep apnea in patients with moderate to severe chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2015;12(8):1219–1225. doi:10.1513/AnnalsATS.201407-336OC
- Patout M, Lhuillier E, Kaltsakas G, et al. Long-term survival following initiation of home non-invasive ventilation: a European study. Thorax. 2020;75(11):965–973. doi:10.1136/thoraxjnl-2019-214204
- Crimi C, Noto A, Princi P, et al. Domiciliary Non-invasive Ventilation in COPD: an International Survey of Indications and Practices. COPD. 2016;13(4):483–490. doi:10.3109/15412555.2015.1108960
- Schwarz SB, Callegari J, Hamm C, Windisch W, Magnet FS. Is outpatient control of long-term non-invasive ventilation feasible in chronic obstructive pulmonary disease patients? Respiration. 2018;95(3):154–160. doi:10.1159/000484569
- Lujan M, Moreno A, Veigas C, Monton C, Pomares X, Domingo C. Non-invasive home mechanical ventilation: effectiveness and efficiency of an outpatient initiation protocol compared with the standard in-hospital model. Respir Med. 2007;101(6):1177–1182. doi:10.1016/j.rmed.2006.11.006
- Chatwin M, Nickol AH, Morrell MJ, Polkey MI, Simonds AK. Randomised trial of inpatient versus outpatient initiation of home mechanical ventilation in patients with nocturnal hypoventilation. Respir Med. 2008;102(11):1528–1535. doi:10.1016/j.rmed.2008.07.019
- Duiverman ML, Vonk JM, Bladder G, et al. Home initiation of chronic non-invasive ventilation in COPD patients with chronic hypercapnic respiratory failure: a randomised controlled trial. Thorax. 2020;75(3):244–252. doi:10.1136/thoraxjnl-2019-213303
- Callegari J, Magnet FS, Taubner S, et al. Interfaces and ventilator settings for long-term noninvasive ventilation in COPD patients. Int J Chron Obstruct Pulmon Dis. 2017;12:1883–1889. doi:10.2147/COPD.S132170
- Yazar EE, Ozlu T, Sariaydin M, et al. Prospective cross-sectional multicenter study on domiciliary noninvasive ventilation in stable hypercapnic COPD patients. Int J Chron Obstruct Pulmon Dis. 2018;13:2367–2374. doi:10.2147/COPD.S164384
- Adler DE, Rabec C, Janssens J-P. Home monitoring and follow-up of long-term NIV. In: Simonds AK, editor. ERS Practical Handbook of Noninvasive Ventilation. European Respiratory Society; 2015:265–275.
- Ribeiro C, Conde S, Oliveira P, et al. Portuguese adaptation of the S3-non-invasive ventilation (S3-NIV) questionnaire for home mechanically ventilated patients. Pulmonology. 2020. doi:10.1016/j.pulmoe.2020.11.006
- Schwarz SB, Magnet FS, Windisch W. Why high-intensity NPPV is favourable to low-intensity NPPV: clinical and physiological reasons. COPD. 2017;14(4):389–395. doi:10.1080/15412555.2017.1318843
- Halpin DMG. Palliative care for people with COPD: effective but underused. Eur Respir J. 2018;51(2):Feb. doi:10.1183/13993003.02645-2017