
Abstract
Introduction
Acute exacerbations of chronic obstructive pulmonary disease (AECOPDs) are important clinical events, with many patients experiencing multiple AECOPDs annually. The terms used in the literature to define recurring AECOPD events are inconsistent and may impact the ability to describe the true burden of these events. We undertook a systematic review to identify and summarize terms and definitions used in observational studies to describe AECOPD-related events occurring after an initial AECOPD (hereafter “subsequent AECOPD”).
Methods
PubMed was searched (2000–2019) for observational studies on subsequent AECOPD events using broad search strings for “COPD”, “exacerbation”, and “subsequent exacerbation events”. Only English-language studies were included. Small studies (n<50) and studies focusing on hospital re-admission only were excluded. Extracted data were analyzed descriptively to generate a narrative summary, using a thematic approach to group studies utilizing similar terms for subsequent AECOPD.
Results
Forty-seven studies were included. No single, distinct terms or definitions were used to define and identify multiple occurrences of AECOPDs, though most (46) studies used one or more of four clustered terms and definitions: reapse (n = 13), recurrence/re-exacerbation (n = 11), treatment failure (n = 12) and non-recovery/time to recovery (n = 16). Heterogeneity was observed within and between the four clusters with respect to study setting, starting point for observing subsequent AECOPDs, time frame to identify a subsequent AECOPD (except for studies using “time to recovery”), and basis for identifying a subsequent exacerbation.
Conclusion
Our review demonstrates that subsequent AECOPDs (including events such as relapse, recurrence/re-exacerbation, treatment failure, non-recovery/time to recovery) are ill-defined in the observational study literature, emphasizing the need to reach consensus on precise and objective definitions (for example, when one AECOPD ends and another begins). Use of standardized terminology and definitions may aid comparability between, and synthesis of, studies, thus improving the understanding of the natural history and burden of exacerbations in COPD patients.
Introduction
Chronic obstructive pulmonary disease (COPD) is the 3rd leading cause of mortality worldwideCitation1 and a significant cause of morbidity.Citation2 Acute exacerbations of COPD (AECOPDs) are important clinical events and contribute significantly to overall disease burden and mortality.Citation3 AECOPDs are generally defined as an acute, and sustained, worsening of respiratory symptoms requiring additional treatment, including hospitalization when severe.Citation4–Citation6 Approximately 50% of COPD patients experience at least one AECOPD event each year, with exacerbations occurring across all stages of disease severity.Citation7,Citation8 Frequent AECOPD events may increase a patient’s risk of mortality,Citation9 and decrease their lung functionCitation10–Citation12 and quality of life.Citation13 Severe AECOPDs pose a financial burden, with AECOPD hospitalizations accounting for up to 70% of COPD-related healthcare expenditures.Citation14–Citation16
The European Respiratory Society/American Thoracic Society guidelines on COPD management of exacerbations proposed in 2017 state that exacerbations are defined as “episodes of increasing respiratory symptoms, particularly dyspnea, cough and sputum production, and increased sputum purulence”.Citation17 In clinical trials and observational studies, AECOPDs tend to be defined based on symptoms (eg, following the classic Anthonisen classification),Citation18 healthcare utilization (eg, prescriptions for AECOPD treatment, management in hospital), or both.Citation19 Identification of symptoms suggestive of AECOPDs may be prospectively recorded in patient daily diaries,Citation20 or retrospectively recalled in patient interviews. Alternatively, evidence of healthcare resource utilization (HCRU) for AECOPD may be identified using records in an electronic health records or administrative claims database. A prospective analysis of exacerbations identified by either symptoms or HCRU demonstrated a higher mean rate of exacerbations using the HCRU definition and showed limited agreement between HCRU and symptom-based exacerbations, thus complicating the evaluation of exacerbations in published studies.Citation21
Despite the existence of guidelines and efforts to clarify best practice, there is no international consensus or standardized definition of how the start and end dates for exacerbations should be defined. For example, discharge from hospital for treatment of an AECOPD is often used to define the end of an exacerbation in observational studies; however, patients are still likely to be experiencing exacerbation symptoms after discharge, with exacerbation symptoms typically lasting around a week and some lasting as long as 8 weeks or more.Citation22 Whilst algorithms have been defined and validated to identify AECOPD in electronic health records,Citation23 there remains, however, considerable heterogeneity amongst the definitions for AECOPD.Citation19
In addition to challenges that exist with defining when an AECOPD event starts and ends, there are further challenges in defining recurring AECOPD events (ie, when does the initial AECOPD event end and another start), as well as AECOPD recovery and treatment failure. Collectively, we refer to these AECOPD-related events occurring after an initial AECOPD as “subsequent AECOPD events”. Differences in study designs, definitions, and how AECOPD was ascertained yield different estimates of re-exacerbation risk within discrete time periods. There is recognition within the research community that a lack of standardized, consistently used definition for exacerbations hampers efforts to assess new therapeutic approaches for AECOPD treatment.Citation24,Citation25 As a first step in obtaining external consensus on how subsequent mild, moderate or severe AECOPD events should be defined, our primary objective was to conduct a systematic review to identify and critically summarize the terms and definitions used in observational studies to describe recurrence, treatment failure and recovery of AECOPD. In order to demonstrate the impact on potential inconsistency of definitions for subsequent AECOPD events, a secondary objective was to report the frequency of recurrent AECOPD events, in addition to non-recovery and treatment failure events.
Methods
We performed a systematic review of observational studies reported in the literature. PubMed was searched for relevant studies published between 1 January 2000 and 31 December 2019. Search strings for terms relating to “disease”, “exacerbation”, and “subsequent exacerbation events” were combined using an AND operator (see Supplement for details). The search was limited to articles with available abstracts and published in the English language; there was no restriction on the geographical scope.
Articles describing subsequent AECOPD events (eg, recurrence, treatment failure or recovery) in relation to an initial or index AECOPD event were included, with screening performed in two stages. In Stage 1, titles and abstracts were reviewed for the following exclusion criteria: study not presenting original observational research (clinical trials, randomized clinical trials, narrative reviews, letters, case reports); study reporting hospital readmission only; no outcomes of interest (ie, subsequent AECOPD); articles did not answer review objective. In Stage 2, the full text of articles identified in Stage 1 for potential inclusion were reviewed for all the exclusion criteria from Stage 1, plus the following additional exclusion criteria: study not describing subsequent AECOPD events in relation to an index AECOPD, no outcome of interest, hospital readmission only study including chronic bronchitis patients only, sample size <50, review article. Disagreements were resolved at both stages by consensus or arbitration with an additional reviewer. As a minimum, 1 person screened the titles/abstracts and performed the full text selection, with another extracting the data. Each step was cross-checked by an independent reviewer. Study investigators were not contacted.
Data from the included studies were extracted into evidence tables summarizing study design and population, definition and terminology for subsequent AECOPD event(s), time point from which subsequent AECOPD events were observed (eg, hospital discharge), and length of follow-up to observe subsequent AECOPD events. Where available, the proportion of patients experiencing a subsequent AECOPD event, or the mean time to subsequent AECOPD event was extracted. Data extraction was cross-checked by multiple researchers. Quality of the included studies was assessed broadly with a focus on the completeness of the subsequent AECOPD definition. No studies were excluded from the review based on quality assessment. Extracted data were analyzed descriptively to generate a narrative summary. A thematic approach was used to group studies utilizing similar terms for subsequent AECOPD.
This comprehensive review followed the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelinesCitation26 for systematic reviews except for two points: the review was not registered and no formal assessment of the risk of bias or quality of the evidence for included studies was performed, however, this was informally assessed.
Results
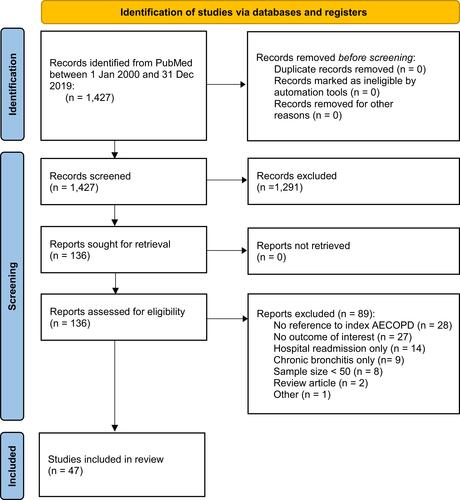
At Stage 1 (title and abstract review), 1291 articles (of 1427 identified) were excluded, with 136 articles proceeding to Stage 2 screening (full text review). At Stage 2, 89 articles were excluded, leaving 47 selected for data extraction. The number of articles identified, screened, assessed for eligibility and then included in the review are presented in . A description of 46 of the included articles is in – with further description of all 47 articles in the Supplement.
Table 1 Characteristics of Studies Observing Relapse Events Following an Exacerbation
Table 2 Characteristics of Studies Observing Recurrence or Re-Exacerbation Events Following an Exacerbation
Table 3 Characteristics of Studies Observing Treatment Failure Following an Exacerbation
Table 4 Characteristics of Studies Observing Non-Recovery or Time to Recovery Events Following an Exacerbation
Figure 1 PRISMA* flow diagram of included and excluded articles. *Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71.Citation26
Terminology
Terminology describing subsequent AECOPD was clustered into four broad groups: relapse, recurrence/re-exacerbation, treatment failure, non-recovery/time to recovery (–). The majority (46) of included studies used these terms and definitions, with some studies using two or more of the four terminology groups.Citation8,Citation27,Citation28 A single study (Matkovic [2012]) used the term adverse outcome, which had a definition similar to definitions for treatment failure in other studies, but was not grouped with the other studies on the basis that the term differed from the four common terms.Citation29
Table 5 Summary of the Four Terms Identified to Describe Subsequent AECOPD Events
Relapse
Exacerbation relapse was a term used by 13 articles and was typically defined as a return to the emergency department (ED) or another physician visit for worsening symptoms and typically not differentiated from recurrence or re-exacerbation ().Citation27,Citation28,Citation30–Citation40 Only relapses of moderate or severe exacerbations were reported. The most common study setting where the term relapse was used was the ED (n = 6), followed by outpatient clinics (n = 3), hospital (n = 2), and then primary care (n = 1). One study was set in both the hospital and ED.Citation38 Almost all studies calculated the proportion of patients with relapse using the number of patients as the denominator: four studies used exacerbations or patient visits as the denominator.Citation28,Citation31,Citation32,Citation40 The timeframe for observing relapse events ranged from five days to one month, with fourteen days being the most common (). The proportion of patients with exacerbation relapse during the timeframe ranged from 7.4% at/before 20 days to 34% at/before one month with no clear trend observed over time.
Figure 2 Reported proportions of patients with (A) relapse event, (B) recurrence/re-exacerbation event, (C) treatment/clinical failure, and (D) non-recovery, by starting point of observation time frame. (A) Includes estimates from 12 observational studies reporting outcomes using a relapse term and definition. Defined as a re-visit to the emergency department or physician for a worsening of symptoms but typically not differentiated from “recurrence” or “re-exacerbation”. One study used two definitions for relapse at 14 days and thus has two data points. Domenach (2013) is not plotted because the study did not report a timeframe. (B) Includes estimates from 10 observational studies reporting outcomes using a recurrence/re-exacerbation term and definition. Mostly defined as a “re-exacerbation” (n = 3), a prescription course of corticosteroids or antibiotics (n = 3), or as a composite outcome (n = 3) including death or AECOPD treatment and/or remission. Some studies (n = 4) required recovery of initial AECOPD prior to subsequent AECOPD. Two studies have data points at several time horizons (30, 90, 180, and 365 days from Wang et al [2012] and 30, 60, 90, and 180 days from Johannesdottir et al [2013]). Bartziokas et al (2014) reported proportion at 3 months and 6 months in “low uric acid” and “high uric acid” groups, but not overall, and therefore these data points are not presented in the figure. (C) Includes estimates from 12 observational studies reporting outcomes using a treatment failure term and definition with some definitions similar to relapse and non-recovery. Often included death (n = 7) and/or was related to in-hospital treatment failure (n = 6). (D) Includes estimates from seven observational studies reporting outcomes using a non-recovery term and definition. Some studies (n = 2) reported estimates at multiple time points and using different methods of measurement (eg, non-recovery ascertained daily symptom score reports or spirometry). Most were from the London COPD cohort. Two studies have multiple data points due to different measurement methods (symptom report and peak expiratory flow, Donaldson [2015] and Seemungal [2000]) over several time horizons (Seemungal [2000] at 35 days and 91 days).Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease; ED, emergency department.
![Figure 2 Reported proportions of patients with (A) relapse event, (B) recurrence/re-exacerbation event, (C) treatment/clinical failure, and (D) non-recovery, by starting point of observation time frame. (A) Includes estimates from 12 observational studies reporting outcomes using a relapse term and definition. Defined as a re-visit to the emergency department or physician for a worsening of symptoms but typically not differentiated from “recurrence” or “re-exacerbation”. One study used two definitions for relapse at 14 days and thus has two data points. Domenach (2013) is not plotted because the study did not report a timeframe. (B) Includes estimates from 10 observational studies reporting outcomes using a recurrence/re-exacerbation term and definition. Mostly defined as a “re-exacerbation” (n = 3), a prescription course of corticosteroids or antibiotics (n = 3), or as a composite outcome (n = 3) including death or AECOPD treatment and/or remission. Some studies (n = 4) required recovery of initial AECOPD prior to subsequent AECOPD. Two studies have data points at several time horizons (30, 90, 180, and 365 days from Wang et al [2012] and 30, 60, 90, and 180 days from Johannesdottir et al [2013]). Bartziokas et al (2014) reported proportion at 3 months and 6 months in “low uric acid” and “high uric acid” groups, but not overall, and therefore these data points are not presented in the figure. (C) Includes estimates from 12 observational studies reporting outcomes using a treatment failure term and definition with some definitions similar to relapse and non-recovery. Often included death (n = 7) and/or was related to in-hospital treatment failure (n = 6). (D) Includes estimates from seven observational studies reporting outcomes using a non-recovery term and definition. Some studies (n = 2) reported estimates at multiple time points and using different methods of measurement (eg, non-recovery ascertained daily symptom score reports or spirometry). Most were from the London COPD cohort. Two studies have multiple data points due to different measurement methods (symptom report and peak expiratory flow, Donaldson [2015] and Seemungal [2000]) over several time horizons (Seemungal [2000] at 35 days and 91 days).Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease; ED, emergency department.](/cms/asset/ecffc99b-7379-4c60-9e12-8b210b3dac8b/dcop_a_12164005_f0002_b.jpg)
Recurrence/Re-Exacerbation
The terms exacerbation recurrence or re-exacerbation were used in 11 articles ().Citation28,Citation41–Citation50 Most studies defined recurrence or re-exacerbation as a worsening of symptoms (n = 3), subsequent prescription of oral corticosteroids or antibiotics (n = 2), or as a composite outcome including treatment or readmission for AECOPD following an initial AECOPD (n = 3). Only four studies specified that recovery from initial AECOPD was required prior to subsequent AECOPD and only recurrence/re-exacerbation of moderate or severe exacerbations were reported. The most common study setting was the hospital (n = 7), followed by outpatient clinics (n = 2), and primary care (n = 1). One study included both hospital inpatient and outpatient participants.Citation50 The timeframe for recurrence or re-exacerbation definitions reporting proportions ranged from one month to 12 months, with either hospital discharge as the initial time point for follow-up (which may or may not be the point at which a patient has “recovered”) (n = 6) or measured following consecutive days free of recorded symptoms (n = 1). The proportion of patients with recurrence/re-exacerbation ranged from 7.4% at/before one month to 88.8% at/before one year, in the same study. shows a trend between length of follow-up and the proportion of patients with a recurrence/re-exacerbation event; however, variability is still seen among studies using the same starting point for follow-up (eg, by 90 days, the proportion of patients with an event following hospital discharge ranged from 25% to 49%).
Treatment Failure
Treatment failure was a term used by 12 articles and was defined as a composite of absence of symptom resolution (n = 2), antibiotic or oral corticosteroid prescription or change in medication (n = 3), hospital readmission (n = 7), increased mechanical ventilator support (n = 5), and/or death (n = 7).Citation51–Citation62 One study defined treatment failure as failure to return to baseline or need for a new treatment medication.Citation57 Treatment failure was a term only used for moderate or severe exacerbations. The most common study setting for treatment failure was the hospital (n = 7), with other studies set in outpatient clinics (n = 3), primary care (n = 1), and home care (n = 1). The timeframe for observing treatment failure ranged from two days from hospital admissionCitation60 to ninety days from hospital discharge.Citation54 The proportion of patients with treatment failure ranged from 14.5% at/before seven daysCitation51 to 36.8% at/before 90 days.Citation54 By 30 days (the most common timeframe), the proportion experiencing treatment failure ranged from 7.4% to 34.8%Citation55 – suggesting heterogeneity in the studies, potentially due to a range of definitions for treatment failure between studies.
Non-Recovery and Time to Recovery
The term non-recovery from an exacerbation was used as a definition for subsequent AECOPD events in 17 studies and was predominantly defined as either symptoms or peak expiratory flow not returning to baseline.Citation10,Citation27,Citation28,Citation36,Citation38,Citation48,Citation57,Citation63–Citation72 Eight studies using the term non-recovery were set within the London COPD cohort, which used patient diary cards to assess recovery. Four of the studies were conducted in outpatient clinics, and two in the ED. One study did not report setting. Four studies, three in the London COPD cohort and one in GIANT, reported both time to recovery and proportion of patients non-recovered by a certain number of days post index.Citation48,Citation63,Citation71,Citation72
Timeframes for non-recovery definitions ranged from eight days from an unclear start pointCitation62 to three months from start of exacerbation.Citation72 The proportion of patients who met the criteria for non-recovery ranged from 8.3% at 99 daysCitation72 to 25% at 35 days.Citation71 Thirteen articles reported mean or median time to recovery rather than (or in addition to) the proportion of patients recovering. Most of these studies were based in the London COPD cohort and conducted in an outpatient setting. Median time to recovery of symptoms in the London COPD studies ranged from 7 days (Q1, Q3: 4, 14 days)Citation71 to 10 days (Q1, Q3: 6, 18 days),Citation72 with similar median time to recovery of peak expiratory flow of 5 and 6 days (Q1, Q3: 0, 14 days and 1, 14 days).Citation71,Citation72 One study reported mean time to “early” recovery (≤4 days) and to “late” recovery (≥8 days) of 3.1 days (SD: 0.9 days) and 102 days (SD: 2.5 days), respectively.Citation63 Overall, median recovery time ranged from 5 daysCitation28 to 13 daysCitation30 and mean recovery time ranged from 3 daysCitation63 to 19 days.Citation66
Six studies reported “time to recovery” only (ie, no proportions) in either an outpatient (n = 5) or cohort (n = 1) study setting, with recovery defined as improvement in symptoms. Two studies measured time from the initial patient visit, three measured time from onset of exacerbation, and one measured time from the last COPD exacerbation. One study presented total recovery time and treated recovery time,Citation69 and one study presented time to recovery stratified by chronic bronchitis status.Citation66 Mean time to recovery ranged from 6.3 days (SD 3.1 days)Citation68 to 13.3 days (SD: 13.3 days).Citation69 Median time to recovery ranged from 7 days (Q1, Q3: 0, 12 days)Citation67 to 13 days (Q1, Q3: 7, 29 days).Citation73
Discussion
In our systematic review, we found no single, distinct terms or definitions were used to define subsequent AECOPD events in the observational study literature, though most studies used one of four clustered terms and definitions: relapse, recurrence/re-exacerbation, treatment failure and non-recovery/time to recovery. Both heterogeneity and similarities were observed among terminologies of subsequent AECOPD, and in the time frames and the settings used to assess these subsequent AECOPD events. Despite some similarities, the heterogeneity we observed may hamper comparability and synthesis of these studies.
In the literature, the distinction between the terms recurrence and re-exacerbation was unclear, and so these two terms were grouped in our analysis. Definitions for treatment failure and relapse often overlapped, such as a return to the ED or a hospital readmission. Definitions for non-recovery were generally distinct, with half of the studies using the term “non-recovery” set in the same cohort. Only one study elucidated the importance of the difference between the definitions of relapse and recurrence, where relapse is treatment failure of a first exacerbation and recurrence is a subsequent AECOPD after successful treatment.Citation28
Terms used to define subsequent AECOPD-related events seem to be chosen pragmatically rather than based on any existing standards, and may be driven by external considerations (eg, incentives/penalties associated with re-admissions for COPD within 30 days such as the Hospital Readmission Reduction Program in the US)Citation74 rather than event time course or disease phenotypes. These factors may contribute to the observed heterogeneity, making definitions of subsequent AECOPDs dependent on healthcare setting and partly explaining the large variation in estimates of subsequent AECOPD-related events defined using the four terminology and definition clusters. The available evidence suggests that the use of event- or symptom-based approaches may lead to substantially different conclusions regarding occurrence of exacerbations.Citation75
In general, the time frames for observing an AECOPD described as a relapse were shorter (up to 30 days) than those for recurrences/re-exacerbations (up to 365 days); time frames for treatment failure and non-recovery were similar (up to approximately 90 days). For all four “subsequent AECOPD” terminology groups, the defined “end” of an initial exacerbation (ie, starting point for observing subsequent events) was variable but frequently included start or end of hospital admission or an ED visit. Re-exacerbation/recurrence was commonly used in the studies with follow-up after hospital admission. The term “treatment failure” was also used frequently in the hospital setting. Non-recovery and relapse study settings were heterogenous.
We observed that the choice of the starting point for measuring subsequent AECOPD can have an important impact on estimates of the proportion of patients experiencing these subsequent events. For example, as a patient cannot experience a re-exacerbation whilst their index exacerbation is ongoing, the proportion of patients experiencing a relapse within 30 days of an index exacerbation will be higher when the 30-day timeframe begins after the exacerbation has ended than when the timeframe begins 5 days after the start of steroid treatment, for example. Exacerbation duration is variable and can be lengthy in some patients and may depend on severity, therefore estimates of subsequent AECOPD will be biased when looking for subsequent events before a patient has recovered or returned to baseline from their initial exacerbation.Citation22
Similarly, exacerbation recovery will appear longer when measured from the onset of symptoms than upon hospital admission. Most of the studies using the term non-recovery used onset of exacerbation as a starting point; however, all these studies were set in the London COPD cohort. The other two studies using non-recovery were also in the same cohort (Medication Adherence Research in COPD Patients cohort) and used presentation to the ED as the starting point. The starting point for re-exacerbation/recurrence in the hospital setting was primarily hospital discharge. Of note, one study set in the London COPD cohort used the term re-exacerbation/recurrence with a starting point as five days free of all recorded symptoms,Citation28 while another study also using re-exacerbation/recurrence and set in the London CODP cohort used onset of exacerbation, similar to the London COPD studies using non-recovery.Citation48
In addition to heterogeneity in the terms, timeframes and starting points for subsequent AECOPD events, we also observed heterogeneity in the study setting. Studies using the term relapse were often set in the ED, whilst most studies conducted in the hospital setting used the term treatment failure. Overall, this heterogeneity has driven variation in the proportion of patients experiencing subsequent events. For example, the proportion of patients with exacerbation relapse ranged from 7.4% at 20 daysCitation36 to 34% at one month,Citation38 with variability (due to differing starting point for follow-up) appearing to have a greater impact on the relapse estimate then the length of follow-up (intuitively, we would expect to see greater proportions of patients experiencing relapse when the length of follow-up for relapse is increased).
There are several potential explanations for our finding that no standard definitions exist. First, exacerbations are heterogenous in terms of symptoms, etiology (bacterial vs viral, specific pathogens vs common pollutants), and time course.Citation71,Citation76,Citation77 Second, there is variation in data sources, primary versus secondary data collection, and availability of specific data to define a re-exacerbation (eg, prescriptions for oral corticosteroids, self-reported symptoms). Finally, specific research questions often drive the type of data collected, and variability by definitions used in different guidelines and countries can contribute to heterogeneity.
Change begins with a recognition of the need for change, and this paper demonstrates that need by highlighting the large amount of heterogeneity between studies. Our finding of common core domains for each definition may be useful for developing an agreed consensus definition for classifying recurring exacerbations, treatment failure, and recovery from AECOPD. As a first step, we believe clear exacerbation definitions are requiredCitation19,Citation24 and that these should be determined by a consensus of experts (for example through a Delphi study) and cascaded via global guideline groups. Then, specific definitions are needed to enable differentiation between distinct AECOPD events. Without standard definitions, our ability to advance the understanding and natural history of AECOPD is impaired.
Strengths of this study include the systematic approach, and the comprehensive, international scope of the literature review. Additionally, studies were not excluded on the basis of quality which allowed us to describe the breadth of definitions currently in the literature. Nonetheless, there are limitations of our research which should be considered when interpreting our findings. First, studies where subsequent AECOPDs were defined as hospital readmission alone were excluded. Second, the included studies were not always explicit in definitions, particularly regarding the index date for recurrent AECOPD events which makes interpretation of the proportion of patients experiencing a subsequent AECOPD difficult. Third, subsequent AECOPD definitions may also differ to randomized clinical trials. This review focused on observational studies; however, a review of the terminology used in randomized clinical trials was presented previously and may better inform how terminology can be standardized to allow for better comparison of treatments.Citation78
Conclusion
In conclusion, our systematic review demonstrates that the concept of subsequent AECOPD is ill-defined in the observational study literature, thus emphasizing the need for rigorous attempts to reach a consensus on a more precise and objective definition for subsequent AECOPDs. Use of standardized terminology and definitions may aid comparability and synthesis of studies, thus improving the understanding of the natural history of AECOPD.
Author Contributions
VSB and HM contributed to the conception and design of the study, data acquisition, data analysis and interpretation. BMD contributed to the data acquisition, analysis and interpretation. WHM, BMD and WF contributed to the data analysis and interpretation. All authors made critical revisions to the draft versions of manuscript and approved the final manuscript, reviewed and agreed on all versions of the article before submission, during revisions, the final version accepted for publication, and any significant changes introduced at the proofing stage. All authors agreed on the journal to which the article would be submitted and agree to take responsibility and be accountable for the contents of the article.
Acknowledgments
We would like to thank Merike Verrijp, Jennifer Euewijk, and Judith van den Bosch (Pallas Health Research and Consulting, The Netherlands) for their part in conducting early literature searches and identifying articles meeting the inclusion criteria. We would also like to acknowledge Maggie Tabberer for her contribution to the project.
Disclosure
WAF and VSB are employees of, and hold shares in, GlaxoSmithKline plc. WHM and HM were employees of GlaxoSmithKline plc. at the time the study was conducted; WHM and HM are currently employees of AstraZeneca. BMD is a PhD candidate at University of North Carolina at Chapel Hill and works for GlaxoSmithKline plc. as a Research Assistant. The authors report no other conflicts of interest in this work.
Additional information
Funding
References
- World Health Organization. Global health estimates 2019: the top 10 causes of death, 2000–2019; 2020. Available from: https://www.who.int/data/global-health-estimates. Accessed November 24, 2021.
- Global Burden of Disease Project Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1151–1210. doi:10.1016/S0140-6736(17)32152-9
- Wedzichia JA, Brill SE, Allinson JP, Donaldson GC. Mechanisms and impact of the frequent exacerbator phenotype in chronic obstructive pulmonary disease. BMC Med. 2013;11:18. doi:10.1186/1741-7015-11-181
- Mathioudakis AG, Janssens W, Sivapalan P, et al. Acute exacerbations of chronic obstructive pulmonary disease: in search of diagnostic biomarkers and treatable traits. Thorax. 2020;75(6):520–527. doi:10.1136/thoraxjnl-2019-214484
- Wedzicha JA, Seemungal TA. COPD exacerbations: defining their cause and prevention. Lancet (London, England). 2007;370(9589):786–796. doi:10.1016/S0140-6736(07)61382-8
- National Institute for Health and Care Excellence. Chronic obstructive pulmonary disease in over 16s: diagnosis and management; 2018. Available from: https://www.nice.org.uk/guidance/ng115/chapter/Recommendations. Accessed November 24, 2021.
- Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471.
- Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363:1128–1138. doi:10.1056/NEJMoa0909883
- Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
- Donaldson GC, Seemungal TA, Patel IS, Lloyd-Owen SJ, Wilkinson TM, Wedzicha JA. Longitudinal changes in the nature, severity and frequency of COPD exacerbations. Eur Respir J. 2003;22(6):931–936. doi:10.1183/09031936.03.00038303
- Dransfield MT, Kunisaki KM, Strand MJ, et al. Acute exacerbations and lung function loss in smokers with and without chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(3):324–330. doi:10.1164/rccm.201605-1014OC
- Whittaker HR, Pimenta JM, Jarvis D, Kiddle SJ, Quint JK. Characteristics associated with accelerated lung function decline in a primary care population with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:3079–3091. doi:10.2147/COPD.S278981
- Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5 Pt 1):1418–1422. doi:10.1164/ajrccm.157.5.9709032
- Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;12:2891–2908. doi:10.2147/COPD.S139470
- Ramsey SD, Sullivan SD. The burden of illness and economic evaluation for COPD. Eur Respir J Suppl. 2003;21:29s–35s. doi:10.1183/09031936.03.00078203
- Strassels SA, Smith DH, Sullivan SD, Mahajan PS. The costs of treating COPD in the United States. Chest. 2001;119(2):344–352. doi:10.1378/chest.119.2.344
- Wedzicha C, Miravitlles M, Hurst JR, et al. Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49(3):1600791. doi:10.1183/13993003.00791-2016
- Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106(2):196–204. doi:10.7326/0003-4819-106-2-196
- Montes de Oca M, Laucho-Contreras ME. Is it time to change the definition of acute exacerbation of chronic obstructive pulmonary disease? What do we need to add? Med Sci. 2018;6(2):50. doi:10.3390/medsci6020050
- Leidy NK, Sexton CC, Jones PW, et al. Measuring respiratory symptoms in clinical trials of COPD: reliability and validity of a daily diary. Thorax. 2014;69(5):443–449. doi:10.1136/thoraxjnl-2013-204428
- O’Reilly JF, Williams AE, Holt K, Rice L. Defining COPD exacerbations: impact on estimation of incidence and burden in primary care. Prim Care Respir J. 2006;15(6):346–353. doi:10.1016/j.pcrj.2006.08.009
- Murray LT, Leidy NK. The short-term impact of symptom-defined COPD exacerbation recovery on health status and lung function. Chron Obstruct Pulmon Dis. 2018;5(1):27–37. doi:10.15326/jcopdf.5.1.2017.0166
- Rothnie KJ, Müllerová H, Hurst JR, et al. Validation of the recording of acute exacerbations of COPD in UK primary care electronic healthcare records. PLoS One. 2016;11(3):e0151357. doi:10.1371/journal.pone.0151357
- Pauwels R, Calverley P, Buist AS, et al. COPD exacerbations: the importance of a standard definition. Respir Med. 2004;98(2):99–107. doi:10.1016/j.rmed.2003.09.001
- Caramori G, Adcock IM, Papi A. Clinical definition of COPD exacerbations and classification of their severity. South Med J. 2009;102(3):277–282. doi:10.1097/SMJ.0b013e3181836b73
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
- Cydulka RK, Rowe BH, Clark S, Emerman CL, Camargo CA Jr. Emergency department management of acute exacerbations of chronic obstructive pulmonary disease in the elderly: the Multicenter Airway Research Collaboration. J Am Geriatr Soc. 2003;51(7):908–916. doi:10.1046/j.1365-2389.2003.51302.x
- Hurst JR, Donaldson GC, Quint JK, Goldring JJ, Baghai-Ravary R, Wedzicha JA. Temporal clustering of exacerbations in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2009;179(5):369–374. doi:10.1164/rccm.200807-1067OC
- Matkovic Z, Huerta A, Soler N, et al. Predictors of adverse outcome in patients hospitalised for exacerbation of chronic obstructive pulmonary disease. Respir Int Rev Thorac Dis. 2012;84(1):17–26. doi:10.1159/000335467
- Aaron SD, Vandemheen KL, Clinch JJ, et al. Measurement of short-term changes in dyspnea and disease-specific quality of life following an acute COPD exacerbation. Chest. 2002;121(3):688–696. doi:10.1378/chest.121.3.688
- Adams SG, Melo J, Luther M, Anzueto A. Antibiotics are associated with lower relapse rates in outpatients with acute exacerbations of COPD. Chest. 2000;117(5):1345–1352. doi:10.1378/chest.117.5.1345
- Domenech A, Ardanuy C, Pallares R, et al. Some pneumococcal serotypes are more frequently associated with relapses of acute exacerbations in COPD patients. PLoS One. 2013;8(3):e59027. doi:10.1371/journal.pone.0059027
- Durmaz D, Goksu E, Kilic T, Ozbudak O, Eray O. The role of nitric oxide in predicting revisit of patients with exacerbated chronic obstructive pulmonary disease. J Emerg Med. 2015;48(2):247–253. doi:10.1016/j.jemermed.2014.06.026
- Durmaz D, Goksu E, Yildiz G, et al. The factors influencing relapse in patients presenting to the emergency department with COPD exacerbation. Turk J Emerg Med. 2015;15(2):59–63. doi:10.5505/1304.7361.2014.37791
- Kim S, Emerman CL, Cydulka RK, Rowe BH, Clark S, Camargo CA. Prospective multicenter study of relapse following emergency department treatment of COPD exacerbation. Chest. 2004;125(2):473–481. doi:10.1378/chest.125.2.473
- Minov J, Stoleski S, Petrova T, Vasilevska K, Mijakoski D, Bislimovska-Karadzhinska J. Moxifloxacin in the outpatient treatment of moderate exacerbations of chronic obstructive pulmonary disease. Open Access Macedon J Med Sci. 2018;6(11):2017–2022. doi:10.3889/oamjms.2018.445
- Miravitlles M, Murio C, Guerrero T. Factors associated with relapse after ambulatory treatment of acute exacerbations of chronic bronchitis. DAFNE Study Group. Eur Respir J. 2001;17(5):928–933. doi:10.1183/09031936.01.17509280
- Miravitlles M, Zalacain R, Murio C, et al. Speed of recovery from acute exacerbations of chronic obstructive pulmonary disease after treatment with antimicrobials: results of a two-year study. Clin Drug Investig. 2003;23(7):439–450. doi:10.2165/00044011-200323070-00003
- Stiell IG, Perry JJ, Clement CM, et al. Clinical validation of a risk scale for serious outcomes among patients with chronic obstructive pulmonary disease managed in the emergency department. CMAJ. 2018;190(48):E1406–E1413. doi:10.1503/cmaj.180232
- Vondracek SF, Hemstreet BA. Retrospective evaluation of systemic corticosteroids for the management of acute exacerbations of chronic obstructive pulmonary disease. Am J Health Sys Pharm. 2006;63(7):645–652. doi:10.2146/ajhp050316
- Bartziokas K, Papaioannou AI, Loukides S, et al. Serum uric acid as a predictor of mortality and future exacerbations of COPD. Eur Respir J. 2014;43(1):43–53. doi:10.1183/09031936.00209212
- Bathoorn E, Groenhof F, Hendrix R, et al. Real-life data on antibiotic prescription and sputum culture diagnostics in acute exacerbations of COPD in primary care. Int J Chron Obstruct Pulmon Dis. 2017;12:285–290. doi:10.2147/COPD.S120510
- Chang C, Yao W. Time course of inflammation resolution in patients with frequent exacerbations of chronic obstructive pulmonary disease. Med Sci Monit. 2014;20:311–320. doi:10.12659/MSM.889828
- Cushen B, McCormack N, Hennigan K, Sulaiman I, Costello RW, Deering B. A pilot study to monitor changes in spirometry and lung volume, following an exacerbation of Chronic Obstructive Pulmonary Disease (COPD), as part of a supported discharge program. Respir Med. 2016;119:55–62. doi:10.1016/j.rmed.2016.08.019
- Hu WP, Lhamo T, Liu D, et al. Development of a nomogram to predict the risk of 30-day re-exacerbation for patients hospitalized for acute exacerbation of chronic obstructive pulmonary disease. COPD. 2019;16(2):160–167. doi:10.1080/15412555.2019.1606187
- Johannesdottir SA, Christiansen CF, Johansen MB, et al. Hospitalization with acute exacerbation of chronic obstructive pulmonary disease and associated health resource utilization: a population-based Danish cohort study. J Med Econ. 2013;16(7):897–906. doi:10.3111/13696998.2013.800525
- Liu D, Peng SH, Zhang J, Bai SH, Liu HX, Qu JM. Prediction of short term re-exacerbation in patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2015;10:1265–1273. doi:10.2147/COPD.S83378
- Perera WR, Hurst JR, Wilkinson TM, et al. Inflammatory changes, recovery and recurrence at COPD exacerbation. Eur Respir J. 2007;29(3):527–534. doi:10.1183/09031936.00092506
- Wang L, Zang XY, Zhang Q, Liu SY, Shen YH, Zhao Y. Study on factors influencing recrudescent time of postdischarge patients with chronic obstructive pulmonary disease. J Clin Nurs. 2012;21(11–12):1507–1514. doi:10.1111/j.1365-2702.2011.03899.x
- Yount SE, Atwood C, Donohue J, et al. Responsiveness of PROMIS(R) to change in chronic obstructive pulmonary disease. J Patient Rep Outcomes. 2019;3(1):65. doi:10.1186/s41687-019-0155-9
- Beauchesne MF, Julien M, Julien LA, et al. Antibiotics used in the ambulatory management of acute COPD exacerbations. Int J Chron Obstruct Pulmon Dis. 2008;3(2):319–322. doi:10.2147/COPD.S2624
- Crisafulli E, Torres A, Huerta A, et al. Predicting in-hospital treatment failure (</= 7 days) in patients with COPD exacerbation using antibiotics and systemic steroids. COPD. 2016;13(1):82–92. doi:10.3109/15412555.2015.1057276
- Dewan NA, Rafique S, Kanwar B, et al. Acute exacerbation of COPD: factors associated with poor treatment outcome. Chest. 2000;117(3):662–671. doi:10.1378/chest.117.3.662
- Garcia-Sidro P, Naval E, Martinez Rivera C, et al. The CAT (COPD Assessment Test) questionnaire as a predictor of the evolution of severe COPD exacerbations. Respir Med. 2015;109(12):1546–1552. doi:10.1016/j.rmed.2015.10.011
- Gaude GS, Rajesh BP, Chaudhury A, Hattiholi J. Outcomes associated with acute exacerbations of chronic obstructive pulmonary disorder requiring hospitalization. Lung India. 2015;32(5):465–472. doi:10.4103/0970-2113.164150
- Lindenauer PK, Pekow PS, Lahti MC, Lee Y, Benjamin EM, Rothberg MB. Association of corticosteroid dose and route of administration with risk of treatment failure in acute exacerbation of chronic obstructive pulmonary disease. JAMA. 2010;303(23):2359–2367. doi:10.1001/jama.2010.796
- Miravitlles M, Llor C, Naberan K, Cots JM, Molina J; EFEMAP study group. Group Es. Variables associated with recovery from acute exacerbations of chronic bronchitis and chronic obstructive pulmonary disease. Respir Med. 2005;99(8):955–965. doi:10.1016/j.rmed.2005.01.013
- Miravitlles M, Izquierdo I, Herrejon A, et al. COPD severity score as a predictor of failure in exacerbations of COPD. The ESFERA study. Respir Med. 2011;105(5):740–747. doi:10.1016/j.rmed.2010.12.020
- Miravitlles M, Garcia-Polo C, Domenech A, Villegas G, Conget F, de la Roza C. Clinical outcomes and cost analysis of exacerbations in chronic obstructive pulmonary disease. Lung. 2013;191(5):523–530. doi:10.1007/s00408-013-9487-z
- Planquette B, Peron J, Dubuisson E, et al. Antibiotics against Pseudomonas aeruginosa for COPD exacerbation in ICU: a 10-year retrospective study. Int J Chron Obstruct Pulmon Dis. 2015;10:379–388. doi:10.2147/COPD.S71413
- Rothberg MB, Pekow PS, Lahti M, Brody O, Skiest DJ, Lindenauer PK. Comparative effectiveness of macrolides and quinolones for patients hospitalized with acute exacerbations of chronic obstructive pulmonary disease (AECOPD). J Hosp Med. 2010;5(5):261–267. doi:10.1002/jhm.628
- Rothberg MB, Pekow PS, Lahti M, Brody O, Skiest DJ, Lindenauer PK. Antibiotic therapy and treatment failure in patients hospitalized for acute exacerbations of chronic obstructive pulmonary disease. JAMA. 2010;303(20):2035–2042. doi:10.1001/jama.2010.672
- Anzueto A, Miravitlles M, Ewig S, Legnani D, Heldner S, Stauch K. Identifying patients at risk of late recovery (>/= 8 days) from acute exacerbation of chronic bronchitis and COPD. Respir Med. 2012;106(9):1258–1267. doi:10.1016/j.rmed.2012.06.002
- Aaron SD, Whitmore GA, Hurst JR, Ramsay T, Wedzicha JA. Time course and pattern of COPD exacerbation onset. Thorax. 2012;67(3):238–243. doi:10.1136/thoraxjnl-2011-200768
- Wilkinson TM, Donaldson GC, Hurst JR, Seemungal TA, Wedzicha JA. Early therapy improves outcomes of exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;169(12):1298–1303. doi:10.1164/rccm.200310-1443OC
- Liang Y, Chen Y, Wu R, et al. Chronic bronchitis is associated with severe exacerbation and prolonged recovery period in Chinese patients with COPD: a multicenter cross-sectional study. J Thorac Dis. 2017;9(12):5120–5130. doi:10.21037/jtd.2017.11.54
- Mackay AJ, Donaldson GC, Patel AR, Singh R, Kowlessar B, Wedzicha JA. Detection and severity grading of COPD exacerbations using the exacerbations of chronic pulmonary disease tool (EXACT). Eur Respir J. 2014;43(3):735–744. doi:10.1183/09031936.00110913
- Miravitlles M, Anzueto A, Ewig S, Legnani D, Stauch K. Characterisation of exacerbations of chronic bronchitis and COPD in Europe: the GIANT study. Ther Adv Respir Dis. 2009;3(6):267–277. doi:10.1177/1753465809352791
- Farias R, Sedeno M, Beaucage D, et al. Innovating the treatment of COPD exacerbations: a phone interactive telesystem to increase COPD Action Plan adherence. BMJ Open Respir Res. 2019;6(1):e000379. doi:10.1136/bmjresp-2018-000379
- Tsai CL, Rowe BH, Camargo CA Jr. Factors associated with short-term recovery of health status among emergency department patients with acute exacerbations of chronic obstructive pulmonary disease. Qual Life Res. 2009;18(2):191–199. doi:10.1007/s11136-008-9437-z
- Seemungal TA, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(5):1608–1613. doi:10.1164/ajrccm.161.5.9908022
- Donaldson GC, Law M, Kowlessar B, et al. Impact of prolonged exacerbation recovery in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(8):943–950. doi:10.1164/rccm.201412-2269OC
- Aaron SD, Donaldson GC, Whitmore GA, Hurst JR, Ramsay T, Wedzicha JA. Time course and pattern of COPD exacerbation onset. Thorax. 2012;67(3):238–243. doi:10.1136/thoraxjnl-2011-200768
- McIlvennan CK, Eapen ZJ, Allen LA. Hospital readmissions reduction program. Circulation. 2015;131(20):1796–1803. doi:10.1161/CIRCULATIONAHA.114.010270
- Trappenburg JC, Schaap D, Monninkhof EM, et al. How do COPD patients respond to exacerbations? BMC Pulm Med. 2011;11:43. doi:10.1186/1471-2466-11-43
- Agusti A, Calverley PM, Decramer M, Stockley RA, Wedzicha JA. Prevention of exacerbations in chronic obstructive pulmonary disease: knowns and unknowns. COPD. 2014;1(2):166–184. doi:10.15326/jcopdf.1.2.2014.0134
- Wedzicha JA. Exacerbations: etiology and pathophysiologic mechanisms. Chest. 2002;121(5, Supplement):136S–141S. doi:10.1378/chest.121.5_suppl.136S
- Meeraus W, Mullerova H, Tabberer M, Fahy WA, Benson VS. Systematic review of COPD re-exacerbation and exacerbation treatment failure definitions used in randomised controlled trials (RCTs). Eur Respirat J. 2018;52(suppl 62):PA1171.