
Abstract
Background
Prolonged sedentary behavior is associated with worse prognosis in patients with chronic obstructive pulmonary disease (COPD). Our previous study found that first-line dual therapy with tiotropium/olodaterol significantly reduces sedentary time compared to tiotropium monotherapy in Japanese patients with treatment-naïve COPD, although the characteristics of responders to dual-therapy versus monotherapy for COPD are still unclear.
Methods
Patients with treatment-naïve COPD were randomized to receive either tiotropium or tiotropium/olodaterol treatment for 12 weeks. Physical activity was assessed using a triaxle accelerometer for 2 weeks before and after treatment. This analysis focused on the change in sedentary time, indicated by physical activity of 1.0–1.5 metabolic equivalents (METs), with stratification for the following factors: age, body mass index (BMI), pulmonary function, COPD assessment test (CAT), the 6-minute walk distance (6MWD), and physical activity level at study entry.
Results
Thirty-five patients received tiotropium/olodaterol and 34 patients received tiotropium. In patients with lower inspiratory capacity at study entry, a significant reduction in sedentary time was observed in the tiotropium/olodaterol group compared with the tiotropium group (Tio: −12.8 ± 13.5 min, Tio/Olo: −65.1 ± 21.0 min, mean difference, −52.2 min, 95% CI −103.6 to 0.88, p = 0.046). In patients with a shorter duration of physical activity of ≥2 METs at study entry, a significant reduction of sedentary time was observed in the tiotropium/olodaterol group compared with the tiotropium group (Tio: −3.3 ± 17.5 min, Tio/Olo: −72.9 ± 23.1 min, mean difference, −69.7 min, 95% CI −128.7 to −10.6, p = 0.02). There were no differences in terms of age, BMI, CAT score, 6MWD, FEV1, FVC, VC, and physical activity of 1.0–1.5 METs and ≥3.0 METs.
Conclusion
This study showed that COPD patients with lower inspiratory capacity or shorter active time of ≥2.0 METs at study entry are likely to exhibit significantly greater reduction in sedentary time with tiotropium/olodaterol treatment.
Introduction
In patients with chronic obstructive pulmonary disease (COPD), airflow limitation causes dyspnea, decreasing quality of life (QOL) and physical activity.Citation1 Physical inactivity has been shown to be associated with increased risks of exacerbation of COPD and mortality.Citation2,Citation3 Long-acting bronchodilator therapy results in an improvement in lung function, along with reduction of symptoms and exacerbations.Citation4–Citation6 The dual bronchodilator combination of a long-acting muscarinic antagonist (LAMA) and a long-acting beta 2 agonist (LABA) reportedly provides greater improvement in pulmonary function and QOL compared with LAMA monotherapy.Citation7,Citation8
Physical activity is defined as any bodily movement produced by skeletal muscles that leads to energy expenditure.Citation9 Physical activity includes all activities in daily life, such as indoor activities, walking, and exercise.Citation10 A step count is one of the indicators of physical activity in daily life, while the tri-axial accelerometer is used to assess physical activity in clinical research.Citation11,Citation12 The intensity of physical activity is measured in terms of metabolic equivalents (METs).Citation13 Patients with COPD have been reported to have a decreased level of physical activity compared with healthy adults, even at an early stage of the disease.Citation14–Citation16
The global initiative for chronic obstructive lung disease (GOLD) has recommended regular physical activity for COPD patients.Citation17 A previous study showed that increasing not only high-intensity physical activity, but also low-intensity physical activity, including sedentary behavior, was essential as a COPD treatment strategy.Citation18 The Saga-naïve COPD Physical Activity Evaluation (SCOPE) Study reported that dual-therapy with tiotropium/olodaterol resulted in significantly greater improvement in forced expiratory volume in 1 s (FEV1) and dyspnea, and reduction in sedentary time as compared to tiotropium monotherapy, although the baseline clinical characteristics of the responders to such therapy among Japanese patients with treatment-naïve COPD receiving dual-therapy could not be investigated.Citation19 The aim of the present study was to clarify the baseline characteristics of responders to first-line dual-therapy as compared to monotherapy by performing a stratified analysis of data from the SCOPE study.
Materials and Methods
Study Subjects
This was a prospective, randomized, multicenter, open-labeled, and parallel intervention study that was conducted at 9 public hospitals located in Japan described in a previous report (UMIN; UMIN000027190).Citation19 In brief, 80 patients (age ≥40 and <85 years old) with treatment-naïve COPD were randomized 1:1, using electronic data capture system, according to 3 factors: %FEV1, age, and smoking history to receive either tiotropium alone or tiotropium/olodaterol treatment for 12 weeks. Entry period of this study was July 2017 to February 2019. Sixty-nine of the 80 patients were included in the study, among whom 34 received tiotropium monotherapy and 35 received dual-therapy with tiotropium and olodaterol (). A diagnosis of COPD was made based on a post-bronchodilator (short acting beta 2 agonist) forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio of less than 70% and presence of a smoking history of ≥10 pack years. However, current and ex-smokers with a post-bronchodilator less than 80% of predicted normal and FEV1 were accepted at the screening visit. Treatment-naïve COPD patients were defined as those who had not received inhaled corticosteroids (ICS), LABA and/or LAMA in the previous 12 months (the full study protocol is described in a previous report).Citation19
Table 1 Characteristics of the Patients at the Baseline
Ethics Approval
Written informed consent was obtained from all patients. This study was approved by the institutional review board of each participating center (approval number: 2016-12-01, Supplementary Table 1). The SCOPE study was conducted according to the principles of the International Conference on Harmonization and Good Clinical Practice, Declaration of Helsinki, and Japanese Good Clinical Practice, and complied with all relevant local regulatory, legal, and ethical requirements (the Japan Registry of Clinical Trials approval no.; jRCTs071180021). The inclusion criteria are described in full in the primary report.Citation19
Study Protocol
To clarify the baseline characteristics of responders to first-line dual-therapy (tiotropium/olodaterol group) versus those receiving monotherapy (tiotropium group) in terms of improvement in physical activity, analyses of the change in physical activity levels after 12 weeks treatments were performed in groups stratified according to age, body mass index (BMI), total COPD assessment test (CAT) scores, the 6-minute walk distance (6MWD), respiratory functions such as FEV1, FVC, vital capacity (VC), and inspiratory capacity (IC) at baseline, and the amount of baseline physical activity, assessed as the daily duration (in minutes) spent doing activity of ≥3, ≥2, and 1.0–1.5 metabolic equivalents (METs) intensity, using the data obtained in the SCOPE study.Citation20,Citation21 In each of the tiotropium/olodaterol and tiotropium treatment groups, patients were divided into two sub-groups based on the median values of each confounding factor, ie, age, BMI, total CAT scores, 6MWD and respiratory function, and longer and shorter duration of physical activity before treatment (baseline).
The average duration of daily physical activity from 8 a.m. to 8 p.m. of three valid days with evaluable data for 12 hours of the day was assessed before and after treatment using a tri-axis accelerometer (Active style PRO HJA-750C, OMRON, Kyoto, Japan).Citation20 Physical activity of 1.0–1.5 METs was considered representative of sedentary time and changes in sedentary time were compared before and after treatment.
Statistical Analysis
The data are presented as mean and standard deviation (SD). Differences between the two treatment groups and the two sub-groups stratified according to each characteristic in each treatment group were evaluated using the Student’s t-test or χ2 test.
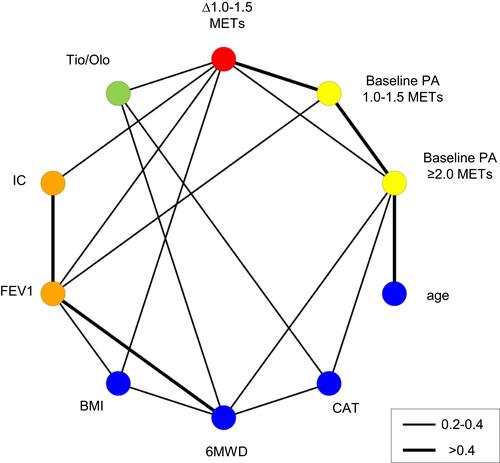
First, the correlation coefficient matrix was calculated to examine the correlation between each factor. shows a graphical representation of the correlation coefficient matrix using the graph theory. In the graph theory, connecting lines (edges) are used to show the relationship between factors (nodes). In this figure, factors with an absolute value of correlation coefficients of 0.2–0.4 are linked by thin lines, and those with correlation coefficients greater than 0.4 are linked by thick lines, thus graphically showing the strength of the correlation between each factor. The Plotly Python graphing library was used to create this figure.
Figure 1 Graphical representation of the factors related to reduction of sedentary time created using a graphical model. Factors with a direct link are connected by lines. The thickness of the line represents the strength of the relationship. The thick lines indicate an absolute value of the correlation coefficient of > 0.4, and the thin line represents a correlation coefficient of 0.2–0.4. The red circle stands for changes in physical activity of 1.0–1.5 METs. The green circle shows treatment with tiotropium/olodaterol, the Orange circles show pulmonary function, the blue circles show clinical characteristics, and the yellow circles represent baseline physical activities.
Next, mean changes in daily sedentary time after treatment were compared between tiotropium/olodaterol and tiotropium treatment groups stratified according to the median baseline value of each confounding factor (ie, higher and lower than the median value), or shorter and longer daily physical activity of ≥3, ≥2, and 1.0–1.5 METs at baseline using Welch’s t-tests. Confounding factors and duration of physical activity of different intensities in patients with a significant reduction of daily sedentary time following tiotropium/olodaterol treatment were identified as baseline characteristics possibly predictive of treatment responders in terms of improvement in sedentary time with dual-therapy compared to tiotropium monotherapy.
Finally, the decision tree method was used to identify baseline factors associated with changes in activity time for each treatment group. The classification and regression tree (CART) algorithm was used to create this decision tree, and mean squared error (MSE) was used as the loss function. The CART algorithm calculates the MSE when the data are divided by a certain factor and cut-off value, and then applies this operation to all candidate factors and cut-off values to find the pair of factors and cut-off values with the minimum MSE. This pair of factors and cut-off values divides the data into two sub-groups, and this operation is repeated recursively to generate further sub-groups. The results can be illustrated as a dendrogram, creating a profile for changes in activity time.
Statistical significance was indicated by a p-value of <0.05, and the missing values were excluded. Data were analyzed with R 3.6.1 software (The R Project for Statistical Computing).
Results
First, graphical representation of the correlation coefficient matrix was used to investigate the association between baseline patient characteristics, pulmonary function, physical activity, treatment, and reduction of sedentary time. Reduction of sedentary time was found to have a direct correlation with treatment with tiotropium/olodaterol, duration of physical activity at baseline of 1.0–1.5 METs and >2.0 METs, IC, FEV1, and BMI. Other factors also showed a correlation with reduction of sedentary time, although the correlation was indirect ().
Next, the effect of patient characteristics at study entry on the reduction of sedentary time with treatment was analyzed by subdividing the two treatment groups into two groups stratified by the median value of the characteristic (Supplemental Figure 1). Subgroup analyses found no correlation between age, BMI, CAT score, or 6MWD and reduction of sedentary time.
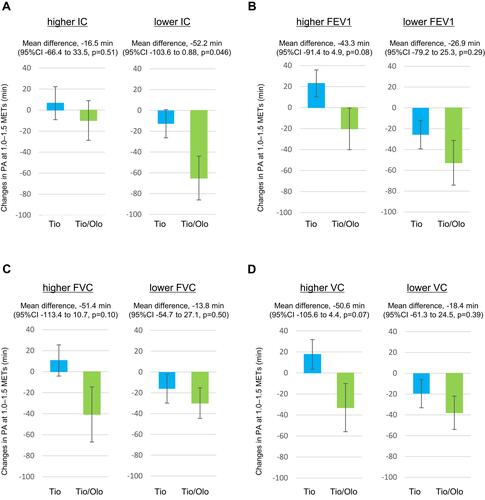
Changes in daily sedentary time following treatment in terms of pulmonary function parameters at baseline are shown in . In the subgroup of patients with lower baseline IC, but not those with higher IC, tiotropium/olodaterol treatment (−65.1 ± 21.0 min) significantly reduced daily sedentary time compared with tiotropium monotherapy (−12.8 ± 13.5 min) (Mean difference, −52.2 min [95% CI −103.6 to 0.88], p = 0.046) (). On the other hand, there were no significant differences in changes in sedentary time between tiotropium/olodaterol and tiotropium treatment groups in the sub-groups of patients with lower and higher baseline FEV1 (), FVC (), and VC ().
Figure 2 Changes in sedentary time before and after treatment stratified according to pulmonary function. Patients were stratified into two groups by a median IC of 1970 mL (A), FEV1 of 1510 mL (B), median FVC of 2840 mL (C), and median VC of 3010 mL (D), for stratified analysis of a reduction in sedentary time with Tio or Tio/Olo treatment. The error bars represent standard errors. p values show differences between two groups. In the subgroup of patients with lower baseline IC, Tio/Olo treatment significantly reduced sedentary time compared with Tio treatment.
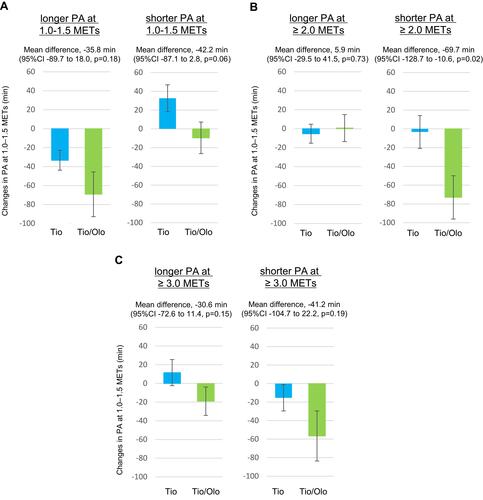
Comparison of reduction of sedentary time with treatment in terms of the intensity of physical activity at baseline () showed that a significant reduction of sedentary time was observed in the tiotropium/olodaterol treatment group (−72.9 ± 23.1 min) compared with the tiotropium treatment group (−3.3 ± 17.5 min) in patients with a shorter, but not longer, duration of baseline physical activity of ≥2 METs intensity (Mean difference −69.7 min [95% CI −128.7 to −10.6], p = 0.02) (). There were no significant differences in changes in sedentary time between tiotropium/olodaterol and tiotropium treatment groups in the subgroup of patients with shorter and longer baseline physical activity of 1.0–1.5 () and ≥3.0 METs ().
Figure 3 Changes in sedentary time before and after treatment stratified by the duration and intensity of physical activity at study entry. Patients were divided into two groups based on a median duration of PA of 1.0–1.5 METs intensity of 282.7 min (A), median duration of PA of ≥ 2.0 METs intensity of 125.1 min (B), and median duration of PA of ≥ 3.0 METs intensity of 31.1 min (C), for stratified analysis of reduction in sedentary time with Tio or Tio/Olo treatment. The error bars represent standard errors. p values show differences between two groups. In the subgroup of patients with a shorter duration of baseline physical activity of ≥2 METs, Tio/Olo treatment significantly reduced sedentary time compared with Tio treatment.
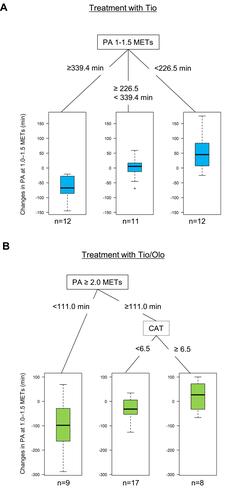
Decision tree analyses were performed to show the most influential factors among patient characteristics, pulmonary function, and physical activity at baseline for reduction of sedentary time with tiotropium () and tiotropium/olodaterol treatment (). Tiotropium monotherapy was found to be most effective for reduction of sedentary time in patients in whom the daily duration of physical activity of 1.0–1.5 METs at study entry was more than 339.4 min. On the other hand, tiotropium/olodaterol was most effective in patients in whom the duration of physical activity of ≥2.0 METs intensity at study entry was shorter than 111.0 min. Therapeutic efficacy was also observed in the group with baseline daily activity of ≥2.0 METs intensity for more than 111.0 min and in those with a CAT score of <6.5.
Figure 4 Decision tree about treatment with Tio or Tio/Olo in treatment-naïve COPD patients. The decision tree was obtained by statistical analysis including patient characteristics (age, BMI, CAT, and 6MWD), pulmonary functions (FEV1, FVC, VC, and IC), and baseline physical activity of 1.0–1.5 METs, PA ≥ 2.0 METs, and PA ≥ 3.0 METs intensity as confounding factors. The decision trees show treatment with Tio (A), and Tio/Olo (B). Tio treatment was most effective for reduction of sedentary time in patients in whom the daily duration of baseline PA of 1.0–1.5 METs was more than 339.4 min. Tio/Olo treatment was most effective in patients in whom the duration of baseline PA of ≥ 2.0 METs was shorter than 111.0 min.
Discussion
The SCOPE study demonstrated that tiotropium/olodaterol treatment improves physical activity, especially in terms of reduction of sedentary time, in treatment-naïve COPD patients. The present study showed that COPD patients with lower IC and shorter active time (≥2.0 METs) at study entry experience a significantly greater reduction of sedentary time with tiotropium/olodaterol treatment. This is the first report to show patient characteristics that are likely associated with reduced sedentary time following treatment with dual bronchodilator therapy. Elucidation of the characteristics of patients in whom tiotropium/olodaterol treatment is likely to be more effective will help tailor the pharmacological treatment strategy in patients with COPD.
Patients with COPD are known to have significantly lower levels of physical activity as compared with healthy subjects.Citation21 The duration of walking is significantly shorter in COPD patients compared with healthy, age-matched subjects.Citation22 Even if patients with mild COPD decreased a level of physical activity, since dyspnea is known to lead to diminished activity levels.Citation9,Citation14 Furthermore, physical inactivity is an essential predictor of mortality in chronic diseases, including diabetes mellitus and cardiovascular disease.Citation23,Citation24 In patients with COPD, physical activity is known to be the strongest prognostic factor for survival compared with pulmonary function.Citation3
Sedentary behavior represents physical activity of 1.0–1.5 METs intensity, standing or walking at a pace of less than 55 m/min is considered physical activity of 2 METs intensity, and walking faster than 55 m/min is considered physical activity of 3 METs intensity.Citation25 Sedentary behavior has also been reported to be an independent predictor of mortality in COPD, even adjusting for moderate-to-vigorous physical activity. Mortality was higher in patients with COPD who spend ≥8.5 h per day in activities requiring <1.5 METs.Citation26
The World Health Organization (WHO) published guidelines on physical activity and sedentary behavior in 2020.Citation27 The guidelines provide general recommendations to reduce sedentary time, which accords with the growing concern regarding the negative health effects of sedentary behavior.Citation28 The recommendations also state that older adults should limit the amount of sedentary time, since replacing sedentary time with physical activity of any intensity (including light intensity) provides health benefits.Citation27 Hence, improving physical activity levels is one of the management goals of COPD guidelines.Citation29 Further, pulmonary rehabilitation programs, including patient education, have been reported to be effective in improving physical activity.Citation30 In the SCOPE study, however, since only a simple leaflet was used to provide a basic explanation of COPD, reduction of sedentary time was considered to be the pure effect of tiotropium/olodaterol rather than patient education.
Stratified analysis showed significant reduction of sedentary time in the low IC group with tiotropium/olodaterol treatment. IC is an index of pulmonary hyperinflation, and the effect of reduction in sedentary time with treatment was probably because the low IC is related to dyspnea and decreased exercise tolerance.Citation31–Citation33 Dynamic hyperinflation is also reported to have an effect on physical activity, regardless of the severity of COPD.Citation34 In the VESUTO study of patients treated with tiotropium/olodaterol, a reduction of sedentary time was observed in the group with higher pulmonary function at baseline, which was contrary to the results observed in our study.Citation35,Citation36 However, baseline pulmonary function of patients in the VESUTO study (%FEV1 52.6%) was lower than in patients in the SCOPE study (%FEV1 62.9%), and the difference in the results could have been due to differences in patient characteristics and COPD treatment at the time of study entry. Furthermore, a significant reduction of sedentary time was observed in patients with a shorter duration of physical activity of above 2.0 METs with tiotropium/olodaterol treatment in the SCOPE study. These data show that tiotropium/olodaterol is more effective in COPD patients with reduced activity levels. These data suggest the efficacy of tiotropium/olodaterol treatment in reducing sedentary time in inactive COPD patients.
A decrease in physical activity time of above 2.5 METs has been reported even in mild COPD patients.Citation22 The previous study showed that replacing sedentary time with other physical activity leads to significant improvements in lung function in COPD patients, suggesting that physicians should pay more attention to the physical activity levels of patients with mild COPD.Citation37 The time spent watching television is also reportedly longer in patients with COPD as compared to healthy older subjects.Citation38 Our results suggest that patients might benefit from even low-intensity exercise, such as standing up during television commercials. Further, since LAMA monotherapy might not be enough to reduce sedentary time in patients with treatment-naïve COPD, treatment with dual-bronchodilator therapy should be considered in patients with low inspiratory capacity and shorter durations of physical activity.
The present study has certain limitations. First, this study included a small sample size and was limited to Japanese patients, which limits its generalizability to other populations. Second, since the duration of treatment was only 12 weeks, we could not show the effects of therapy for more than 12 weeks. Third, this study did not involve intensive patient education regarding COPD and the need for increased physical activity. In clinical settings, pulmonary rehabilitation might result in further behavior modification.
Conclusions
Dual bronchodilator therapy with tiotropium/olodaterol treatment reduced sedentary time in patients with treatment-naïve COPD. Patients with a lower inspiratory capacity and shorter active time of ≥2.0 METs intensity are more likely to benefit from dual tiotropium/olodaterol treatment rather than tiotropium monotherapy.
Data Sharing Statement
The data of this study are stored and managed at the Saga University Clinical Research Center. Any requests for sharing of this data should be addressed to the corresponding author.
Author Contributions
K.T. is the guarantor and takes responsibility for the content of this manuscript, including the data and analysis. H.T., M.U., G.K., Y. K., H.S., T.K., M.Y., and T.K. contributed to study conception and design, data acquisition, and interpretation of the data. R.T., A.T., and A.K. contributed to data acquisition, analysis and interpretation. S.K. and N.S-A. contributed to study conception and design and interpretation of the data. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Dr. Koichiro Takahashi received lecture fees from Nippon Boehringer Ingelheim and AstraZeneca. Dr. Takashi Kinoshita received grants from Daiichi Sankyo. Dr. Makoto Yoshida received lecture fees from AstraZeneca, GlaxoSmithKline, and Novartis Pharma. Dr. Tomotaka Kawayama received grants from Novartis, and lecture fees from AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Novartis Pharma, Teijin Pharma and Home Healthcare, Sanofi, Kyorin Pharmaceutical, and MeijiSeika Pharma. Dr. Hiroki Tashiro, Dr. Masaru Uchida, Dr. Go Kato, Dr. Yuki Kurihara, Dr. Ayako Takamori, Dr. Ryo Tajiri, Dr. Hironori Sadamatsu, Dr. Atsushi Kawaguchi, Dr. Shinya Kimura, and Dr. Naoko Sueoka-Aragane did not have any conflicts of interests.
Additional information
Funding
References
- Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. doi:10.1016/S0140-6736(17)31222-9
- Gimeno-Santos E, Frei A, Steurer-Stey C, et al. Determinants and outcomes of physical activity in patients with COPD: a systematic review. Thorax. 2014;69(8):731–739. doi:10.1136/thoraxjnl-2013-204763
- Waschki B, Kirsten A, Holz O, et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study. Chest. 2011;140(2):331–342. doi:10.1378/chest.10-2521
- Buhl R, Maltais F, Abrahams R, et al. Tiotropium and olodaterol fixed-dose combination versus mono-components in COPD (GOLD 2–4). Eur Respir J. 2015;45(4):969–979. doi:10.1183/09031936.00136014
- Blair HA. Tiotropium/olodaterol: a review in COPD. Drugs. 2019;79(9):997–1008. doi:10.1007/s40265-019-01133-w
- Calverley PMA, Anzueto AR, Carter K, et al. Tiotropium and olodaterol in the prevention of chronic obstructive pulmonary disease exacerbations (DYNAGITO): a double-blind, randomised, parallel-group, active-controlled trial. Lancet Respir Med. 2018;6(5):337–344. doi:10.1016/S2213-2600(18)30102-4
- Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. An official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2020;201(9):e56–e69. doi:10.1164/rccm.202003-0625ST
- Rabe KF, Chalmers JD, Miravitlles M, et al. Tiotropium/olodaterol delays clinically important deterioration compared with tiotropium monotherapy in patients with early COPD: a post hoc analysis of the TONADO((R)) trials. Adv Ther. 2021;38(1):579–593. doi:10.1007/s12325-020-01528-2
- Watz H, Pitta F, Rochester CL, et al. An official European respiratory society statement on physical activity in COPD. Eur Respir J. 2014;44(6):1521–1537. doi:10.1183/09031936.00046814
- Katz S. Assessing self-maintenance: activities of daily living, mobility, and instrumental activities of daily living. J Am Geriatr Soc. 1983;31(12):721–727. doi:10.1111/j.1532-5415.1983.tb03391.x
- Wan ES, Kantorowski A, Homsy D, et al. Self-reported task-oriented physical activity: a comparison with objective daily step count in COPD. Respir Med. 2018;140:63–70. doi:10.1016/j.rmed.2018.05.012
- Sugino A, Minakata Y, Kanda M, et al. Validation of a compact motion sensor for the measurement of physical activity in patients with chronic obstructive pulmonary disease. Respiration. 2012;83(4):300–307. doi:10.1159/000330046
- Ainsworth BE, Haskell WL, Herrmann SD, et al. 2011 compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43(8):1575–1581. doi:10.1249/MSS.0b013e31821ece12
- Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):972–977. doi:10.1164/rccm.200407-855OC
- Gouzi F, Prefaut C, Abdellaoui A, et al. Evidence of an early physical activity reduction in chronic obstructive pulmonary disease patients. Arch Phys Med Rehabil. 2011;92(10):1611–1617 e1612. doi:10.1016/j.apmr.2011.05.012
- Ichinose M, Minakata Y, Motegi T, et al. A non-interventional, Cross-Sectional Study to evaluate factors relating to daily step counts and physical activity in Japanese patients with chronic obstructive pulmonary disease: STEP COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:3385–3396. doi:10.2147/COPD.S277782
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
- Tremblay MS, Aubert S, Barnes JD, et al. Sedentary Behavior Research Network (SBRN) terminology consensus project process and outcome. Int J Behav Nutr Phys Act. 2017;14(1):75. doi:10.1186/s12966-017-0525-8
- Takahashi K, Uchida M, Kato G, et al. First-line treatment with tiotropium/olodaterol improves physical activity in patients with treatment-naive chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:2115–2126. doi:10.2147/COPD.S268905
- Minakata Y, Sasaki S. Data reproducibility and effectiveness of bronchodilators for improving physical activity in COPD patients. J Clin Med. 2020;9(11):3497. doi:10.3390/jcm9113497
- Watz H, Waschki B, Meyer T, Magnussen H. Physical activity in patients with COPD. Eur Respir J. 2009;33(2):262–272. doi:10.1183/09031936.00024608
- Troosters T, Sciurba F, Battaglia S, et al. Physical inactivity in patients with COPD, a controlled multi-center pilot-study. Respir Med. 2010;104(7):1005–1011. doi:10.1016/j.rmed.2010.01.012
- Wahid A, Manek N, Nichols M, et al. Quantifying the association between physical activity and cardiovascular disease and diabetes: a systematic review and meta-analysis. J Am Heart Assoc. 2016;5(9). doi:10.1161/JAHA.115.002495
- Biswas A, Oh PI, Faulkner GE, et al. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: a systematic review and meta-analysis. Ann Intern Med. 2015;162(2):123–132. doi:10.7326/M14-1651
- Park J, Ishikawa-Takata K, Tanaka S, Mekata Y, Tabata I. Effects of walking speed and step frequency on estimation of physical activity using accelerometers. J Physiol Anthropol. 2011;30(3):119–127. doi:10.2114/jpa2.30.119
- Furlanetto KC, Donaria L, Schneider LP, et al. Sedentary behavior is an independent predictor of mortality in subjects with COPD. Respir Care. 2017;62(5):579–587. doi:10.4187/respcare.05306
- Ding D, Mutrie N, Bauman A, Pratt M, Hallal PRC, Powell KE. Physical activity guidelines 2020: comprehensive and inclusive recommendations to activate populations. Lancet. 2020;396(10265):1780–1782. doi:10.1016/S0140-6736(20)32229-7
- Saunders TJ, McIsaac T, Douillette K, et al. Sedentary behaviour and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab. 2020;45(10 (Suppl. 2)):S197–S217. doi:10.1139/apnm-2020-0272
- Piercy KL, Troiano RP, Ballard RM, et al. The physical activity guidelines for Americans. JAMA. 2018;320(19):2020–2028. doi:10.1001/jama.2018.14854
- Troosters T, Maltais F, Leidy N, et al. Effect of bronchodilation, exercise training, and behavior modification on symptoms and physical activity in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(8):1021–1032. doi:10.1164/rccm.201706-1288OC
- O’Donnell DE, Webb KA. Exertional breathlessness in patients with chronic airflow limitation. The role of lung hyperinflation. Am Rev Respir Dis. 1993;148(5):1351–1357. doi:10.1164/ajrccm/148.5.1351
- O’Donnell DE, Revill SM, Webb KA. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(5):770–777. doi:10.1164/ajrccm.164.5.2012122
- O’Donnell DE, Elbehairy AF, Webb KA, Neder JA; Canadian Respiratory Research N. The link between reduced inspiratory capacity and exercise intolerance in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2017;14(Supplement_1):S30–S39. doi:10.1513/AnnalsATS.201610-834FR
- Garcia-Rio F, Lores V, Mediano O, et al. Daily physical activity in patients with chronic obstructive pulmonary disease is mainly associated with dynamic hyperinflation. Am J Respir Crit Care Med. 2009;180(6):506–512. doi:10.1164/rccm.200812-1873OC
- Ichinose M, Minakata Y, Motegi T, et al. Efficacy of tiotropium/olodaterol on lung volume, exercise capacity, and physical activity. Int J Chron Obstruct Pulmon Dis. 2018;13:1407–1419. doi:10.2147/COPD.S166023
- Minakata Y, Motegi T, Ueki J, et al. Effect of tiotropium/olodaterol on sedentary and active time in patients with COPD: post hoc analysis of the VESUTO((R)) study. Int J Chron Obstruct Pulmon Dis. 2019;14:1789–1801. doi:10.2147/COPD.S208081
- Dogra S, Good J, Gardiner PA, et al. Effects of replacing sitting time with physical activity on lung function: an analysis of the Canadian Longitudinal Study on aging. Health Rep. 2019;30(3):12–23. doi:10.25318/82-003-x201900300002-eng
- Lewis LK, Hunt T, Williams MT, English C, Olds TS. Sedentary behavior in people with and without a chronic health condition: how much, what and when? AIMS Public Health. 2016;3(3):503–519. doi:10.3934/publichealth.2016.3.503