

Abstract
Background
Recent studies report a lower mortality rate during treatment with long-acting muscarinic antagonist (LAMA)/long-acting β2-agonist (LABA)/inhaled corticosteroid (ICS) versus LAMA/LABA in patients with symptomatic chronic obstructive pulmonary disease (COPD) and a history of exacerbations.
Objective
We compared time to all-cause mortality with LAMA/LABA versus LAMA/LABA/ICS in patients with mild-to-very-severe COPD and a predominantly low exacerbation risk.
Methods
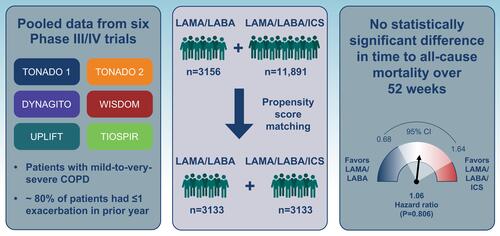
Data were pooled from six randomized controlled trials (TONADO 1/2, DYNAGITO, WISDOM, UPLIFT and TIOSPIR; LAMA/LABA: n = 3156, LAMA/LABA/ICS: n = 11,891). Analysis was on-treatment and data were censored at 52 weeks. Patients on LAMA/LABA/ICS received ICS prior to study entry, which was not withdrawn at randomization. Patients on LAMA/LABA/ICS were propensity score (PS)-matched to patients on LAMA/LABA who had not previously received ICS; covariates included age, sex, geographical region, smoking status, post-bronchodilator forced expiratory volume in 1 second percent predicted, exacerbation history in previous year, body mass index and time since diagnosis. Time to all-cause mortality was assessed using Cox proportional hazard regression models.
Results
After PS matching, 3133 patients on LAMA/LABA and 3133 patients on LAMA/LABA/ICS were analyzed. Fewer than 20% of patients reported ≥2 exacerbations in the prior year (LAMA/LABA: 19.1%; LAMA/LABA/ICS: 19.0%). There were 41 (1.3%) deaths on LAMA/LABA and 45 (1.4%) deaths on LAMA/LABA/ICS. No statistically significant difference in time to death was observed between treatment arms (hazard ratio for LAMA/LABA 1.06; 95% confidence intervals 0.68, 1.64; P = 0.806). Sensitivity analyses conducted using different covariates or in an intent-to-treat population showed similar results.
Conclusion
This pooled analysis of over 6000 patients with mild-to-very-severe COPD and predominantly low exacerbation risk showed no differences in mortality with LAMA/LABA versus LAMA/LABA/ICS, suggesting that the survival benefit of triple therapy seen in some recent studies may be specific to a high-risk population. This supports current Global Initiative for Chronic Obstructive Lung Disease recommendations that triple therapy should be reserved for the subpopulations of patients who need it the most (eg, those with an eosinophilic phenotype and a high risk of exacerbations) to avoid ICS overuse.
Graphical Abstract
Abbreviations
BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroids; ITT, intention to treat; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist.
Data Sharing Statement
To ensure independent interpretation of clinical study results and enable authors to fulfill their role and obligations under the ICMJE criteria, Boehringer Ingelheim grants all external authors access to relevant clinical study data. In adherence with the Boehringer Ingelheim Policy on Transparency and Publication of Clinical Study Data, scientific and medical researchers can request access to clinical study data after publication of the primary manuscript in a peer-reviewed journal, regulatory activities are complete and other criteria are met. Researchers should use the https://vivli.org/ link to request access to study data and visit https://www.mystudywindow.com/msw/datasharing for further information.
Ethics Approval and Informed Consent
The studies included in this pooled analysis were all performed in accordance with the Declaration of Helsinki, International Conference on Harmonisation Harmonised Tripartite Guideline for Good Clinical Practice and local regulations. The protocols were approved by the authorities and the ethics committees of the respective institutions, and signed informed consent was obtained from all patients, as described in the earlier publications.
Acknowledgments
Support for this project was provided by Boehringer Ingelheim International GmbH (BI). The authors did not receive payment related to the development of the manuscript. Medical writing assistance, in the form of the preparation and revision of the manuscript, was supported financially by BI and provided by Vicki Cronin of MediTech Media, under the authors’ conceptual direction and based on feedback from the authors. BI was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations. The authors would like to thank Wenqiong Xue for her contributions to the statistical analysis.
This manuscript includes some content that was previously presented at the 2021 American Thoracic Society International Conference as a poster presentation. The poster’s abstract was published in “Meeting Abstracts” in Am J Respir Crit: https://www.atsjournals.org/doi/10.1164/ajrccm-conference.2021.203.1_MeetingAbstracts.A2251.
Author Contributions
The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE). All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Marc Miravitlles has received speaker fees from AstraZeneca, Bial, Boehringer Ingelheim, Chiesi, Cipla, CSL Behring, GlaxoSmithKline, Grifols, Menarini, Novartis, Rovi, Sandoz and Zambon; consulting fees from AstraZeneca, Atriva Therapeutics, Bial, Boehringer Ingelheim, Chiesi, CSL Behring, Gebro Pharma, Ferrer, GlaxoSmithKline, Grifols, Kamada, Laboratorios Esteve, Mereo Biopharma, Novartis, ONO Pharma, pH Pharma, Sanofi, Palobiofarma SL, Spin Therapeutics, Takeda, TEVA and Verona Pharma; and research grants from Grifols. Peter M.A. Calverley has received grants from GlaxoSmithKline; advisory board fees from Boehringer Ingelheim; and speaker and advisory board fees from Phillips Respironics, Recipharm and Zambon. Katia Verhamme has received consultancy fees from Boehringer Ingelheim; payment for a lecture to the Department of Medical Informatics from AstraZeneca; and received unconditional research grants from Yamanouchi, Pfizer/Boehringer Ingelheim, Novartis, GlaxoSmithKline, Amgen, UCB and Chiesi. Michael Dreher has received speaker or advisory fees from Actelion, AstraZeneca, Bayer, Berlin-Chemie, Boehringer Ingelheim, Chiesi, Hamilton, Heinen und Löwenstein, Insmed, InterMune, Linde, Novartis, Pfizer, Philips Respironics, ResMed, Roche and Weinmann. Valentina Bayer, Asparuh Gardev and Alberto de la Hoz are employees of Boehringer Ingelheim. Jadwiga Wedzicha has received grants from AstraZeneca, Boehringer Ingelheim, Chiesi, Genentech, GlaxoSmithKline, Johnson and Johnson, and Novartis, and meeting expenses from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline and Novartis. David Price has board membership with AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme and Thermo Fisher; consultancy agreements with Airway Vista Secretariat, AstraZeneca, Boehringer Ingelheim, Chiesi, EPG Communication Holdings Ltd, FIECON Ltd, Fieldwork International, GlaxoSmithKline, Mylan, Mundipharma, Novartis, OM Pharma SA, PeerVoice, Phadia AB, Spirosure Inc, Strategic North Limited, Synapse Research Management Partners S.L., Talos Health Solutions, Theravance and WebMD Global LLC; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi Genzyme, Theravance and the UK National Health Service; payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mylan, Mundipharma, Novartis, Regeneron Pharmaceuticals and Sanofi Genzyme; payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Mundipharma, Mylan, Novartis and Thermo Fisher; stock/stock options from AKL Research and Development Ltd, which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia and UK) and 92.61% of Observational and Pragmatic Research Institute Pte Ltd (Singapore); 5% shareholding in Timestamp which develops adherence monitoring technology; is peer reviewer for grant committees of the UK Efficacy and Mechanism Evaluation programme and Health Technology Assessment; and was an expert witness for GlaxoSmithKline. The authors report no other conflicts of interest in this work.