

Abstract
Purpose
Blood eosinophil (EOS) count can guide treatment decisions for chronic obstructive pulmonary disease (COPD). In the 52-week ETHOS study (NCT02465567), budesonide/glycopyrronium/formoterol fumarate dihydrate (BGF) triple therapy at two inhaled corticosteroid doses reduced moderate/severe exacerbation rates and improved lung function, symptoms, and disease-related quality of life (QoL) versus dual therapy with glycopyrronium/formoterol fumarate dihydrate (GFF) or budesonide/formoterol fumarate dihydrate (BFF) in patients with moderate-to-very severe COPD. This subgroup analysis evaluated treatment benefits in ETHOS by baseline EOS count.
Methods
Patients (40−80 years) with a COPD history were randomly assigned 1:1:1:1 to receive BGF 320/14.4/10 µg, BGF 160/14.4/10 µg, GFF 14.4/10 µg, or BFF 320/10 µg via a metered-dose inhaler. This post-hoc analysis assessed endpoints by baseline EOS count using Global Initiative for Obstructive Lung Disease thresholds (<100, ≥100, ≥100−<300, ≥300 cells/mm3), and investigated continuous relationships between treatment effects and EOS count on exacerbations, symptoms, disease-related QoL, lung function, and safety.
Results
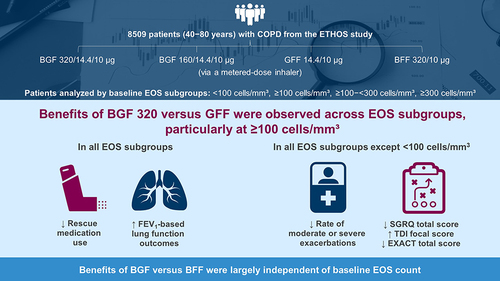
In the modified intention-to-treat population (n=8509), 82.6% had EOS counts ≥100 cells/mm3. BGF 320 reduced moderate/severe exacerbation rates versus GFF in the ≥100, ≥100−<300, and ≥300 subgroups; treatment differences increased with EOS count. BGF 320 improved rescue medication use and lung-function outcomes across all subgroups, and St George’s Respiratory Questionnaire total score, Transition Dyspnea Index focal score, and Exacerbations of Chronic Pulmonary Disease Tool total score in all except the <100 subgroup versus GFF. Benefits of BGF 320 versus BFF were generally consistent across subgroups. Safety data were comparable across subgroups.
Conclusion
Benefits of BGF versus GFF were observed across EOS counts, particularly at ≥100 cells/mm³; versus BFF, benefits were largely independent of EOS. These findings confirm that benefits of ICS-containing triple therapy are not restricted to EOS counts ≥300 cells/mm³, supporting recommendations to consider triple therapy in patients with an exacerbation history and EOS counts ≥100 cells/mm³.
Graphical Abstract
Abbreviations
AUC0–4, area under the concentration–time curve from 0−4 h; BFF, budesonide/formoterol fumarate dihydrate; BGF, budesonide/glycopyrronium/formoterol fumarate dihydrate; CAT, COPD Assessment Test; CI, confidence interval; COPD, chronic obstructive pulmonary disease; EOS, blood eosinophil; EXACT, Exacerbations of Chronic Pulmonary Disease Tool; FEV1, forced expiratory volume in 1 s; GFF, glycopyrronium/formoterol fumarate dihydrate; GOLD, Global Initiative for Obstructive Lung Disease; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist, LAMA, long-acting muscarinic antagonist; LSM, least square mean; MACE, major adverse cardiovascular event; mITT, modified intention-to-treat; QoL, quality of life; RR, rate ratio; SD, standard deviation; SGRQ, St George’s Respiratory Questionnaire; TDI, Transition Dyspnea Index; TEAE, treatment-emergent adverse event.
Data Sharing Statement
Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data-sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure.
Ethics Approval and Informed Consent
The study protocol and informed consent form were approved by the appropriate institutional review board, independent ethics committee, or health authority (Supporting Table S3), and written informed consent was obtained from all patients before screening.
Acknowledgments
Medical writing support, under the direction of the authors, was provided by Sara Cameron, MPhil, and Daniel Spindlow, MSc, CMC Connect, a division of IPG Health Medical Communications, funded by AstraZeneca in accordance with Good Publication Practice (GPP 2022) guidelines.Citation24 Dave Singh is supported by the National Institute for Health Research (NIHR) Manchester Biomedical Research Centre (BRC).
Author Contributions
All authors made a significant contribution to the work reported. MB and DS contributed to the study conception or design and the interpretation of data. KFR, FJM, PDa, and PDo contributed to the study conception or design, analysis of data and interpretation of data. MJ and MP contributed to the analysis of data and interpretation of data. MA contributed to the study conception or design, acquisition of data, and analysis of data. All authors took part in drafting, revising, or critically reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Disclosure
MB reports grants from AstraZeneca, and honoraria from AstraZeneca, Chiesi, and GlaxoSmithKline; and is on the scientific advisory board for Albus Health and ProAxsis. KFR reports grants and personal fees from AstraZeneca and Boehringer Ingelheim; and personal fees from Berlin Chemie, Chiesi Pharmaceuticals, GlaxoSmithKline, Novartis, Regeneron, Roche, and Sanofi, outside the submitted work. FJM reports grants, personal fees, and non-financial support from AstraZeneca during the conduct of the study; grants, personal fees, and non-financial support from AstraZeneca, Boehringer Ingelheim, Bioscale/Proterrix Bio, Chiesi, CSL Behring, Gala, GlaxoSmithKline, Metronic, Novartis, Polarean, Pulmatrix, Pulmonx, Sanofi/Regeneron, Sunovion, Teva, Theravance/Viatris, and Verona; grants and personal fees from AstraZeneca, Chiesi, GlaxoSmithKline, and Sanofi/Regeneron. He is also a COPD teleconsultant for Bayer. DS reports personal fees from AstraZeneca during the conduct of the study; and personal fees from Aerogen, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, CSL Behring, Epiendo, Genentech, GlaxoSmithKline, Glenmark, Gossamerbio, Kinaset, Menarini, Mundipharma, Novartis, Peptinnovate, Pfizer, Pulmatrix, Sanofi, Synairgen, Teva, Theravance, and Verona, outside the submitted work. PDa, MJ, MA, and MP are employees of AstraZeneca and hold stock and/or stock options in the company. PDo is a former employee of AstraZeneca and previously held stock and/or stock options in the company. The authors report no other conflicts of interest in this work.