
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
After the institution of positive-pressure ventilation, the use of noninvasive ventilation (NIV) through an interface substantially increased. The first technique was continuous positive airway pressure; but, after the introduction of pressure support ventilation at the end of the 20th century, this became the main modality. Both techniques, and some others that have been recently introduced and which integrate some technological innovations, have extensively demonstrated a faster improvement of acute respiratory failure in different patient populations, avoiding endotracheal intubation and facilitating the release of conventional invasive mechanical ventilation. In acute settings, NIV is currently the first-line treatment for moderate-to-severe chronic obstructive pulmonary disease exacerbation as well as for acute cardiogenic pulmonary edema and should be considered in immunocompromised patients with acute respiratory insufficiency, in difficult weaning, and in the prevention of postextubation failure. Alternatively, it can also be used in the postoperative period and in cases of pneumonia and asthma or as a palliative treatment. NIV is currently used in a wide range of acute settings, such as critical care and emergency departments, hospital wards, palliative or pediatric units, and in pre-hospital care. It is also used as a home care therapy in patients with chronic pulmonary or sleep disorders. The appropriate selection of patients and the adaptation to the technique are the keys to success. This review essentially analyzes the evidence of benefits of NIV in different populations with acute respiratory failure and describes the main modalities, new devices, and some practical aspects of the use of this technique.
Introduction
Noninvasive ventilation (NIV) refers to the delivery of ventilatory support or positive pressure into the lungs without an invasive endotracheal airway,Citation1,Citation2 usually through a mask. This technique has been demonstrated to efficiently improve acute respiratory failure (ARF), avoiding the complications associated with endotracheal intubation (EI) and conventional invasive mechanical ventilation (IMV), especially ventilator-associated pneumonia.Citation3,Citation4
The main modality is noninvasive pressure support ventilation (NIPSV). Older modalities, such as continuous positive airway pressure (CPAP), as well as ones recently introduced into the market, have been successfully used in the setting of ARF.Citation5,Citation6 A recent survey carried out in USA showed that the use of NIV to treat acute exacerbations of chronic obstructive pulmonary disease (COPD) increased more than 400% in one decade (from 1% in 1998 to 4.5% in 2008) and was associated with a 42% reduction in IMV.Citation7 NIV is now a first-line therapy in emergency departments,Citation8 regular hospital wards,Citation9 palliativeCitation10 or pediatricCitation11 care units, and even in out-of-hospital patients.Citation12,Citation13
We performed a search in PubMed National Library with the key words “non-invasive-ventilation.” The search was limited to: “clinical trials”, “reviews”, “systematic reviews”, and “meta-analyses”. All randomized trials and meta-analyses were selected. Review articles were chosen according to their relevance, based on the author’s reputation and the quality of the journal. Nonrandomized trials were also selected from these reviews, according to the relevance of the results and applying similar criteria.
This review focuses on the following: clinical settings in which NIV can be used; modes of NIV; interfaces; ventilators; humidification; when to apply NIV; predictors of failure; practical aspects; monitoring NIV; the use of sedation; when to stop NIV; and conclusions.
Clinical settings in which NIV can be used (indications)
There is strong evidence that the addition of NIV to standard care improves outcomes in patients with COPD exacerbation and in those with acute cardiogenic pulmonary edema (ACPE);Citation14,Citation15 however, the technique is also used to support patients with ARF from other etiologies. There are several contraindications to the use of NIV () where common sense would normally prompt intubation and IMV.Citation16,Citation17
Table 1 Contraindications of noninvasive ventilation
COPD
Acute exacerbations
A significant number of randomized trials have shown an improvement in gas exchange and symptoms with the use of NIPSV compared to conventional oxygen therapy (COT) in patients with COPD exacerbation.Citation18–Citation23 In addition, some randomized trials and several meta-analyses or systematic reviews confirmed the superiority of NIPSV over COT, in that it reduced the EI rate, intensive care unit (ICU) or hospital length of stay, and mortality.Citation24–Citation29 Therefore, NIV should be considered a first-line treatment for these patients with COPD exacerbation,Citation30–Citation32 especially in those with moderate-to-severe decompensation (pH <7.35 and hypercapnia). To ensure better outcomes in terms of intubation and mortality, NIPSV should be initiated early, before severe acidosis occurs.Citation14 This is especially true in patients treated with NIPSV in general wards, as Plant et al demonstrated in a large randomized trial.Citation22 The benefit of NIPSV in cases less severe decompensation (pH ≥7.35) has not been well established.Citation23,Citation33,Citation34 Though pH is by far the most important determinant for deciding whether to institute NIPSV, other clinical factors, such as tachypnea, the severity of dyspnea, and the use of respiratory accessory muscles, should also be considered.Citation35
The rate of NIPSV failure requiring IMV in decompensated COPD patients is low, but, in critical patients, may be as high as 60% (5% to 60%).Citation36,Citation37 The short-term outcomes of these patients are uncertain. Although some authors did not find differences in mortality in patients who failed NIPSV compared to those who underwent IMV directly,Citation38 a registry of patients with COPD exacerbation treated with NIV in USA from 1998 to 2008Citation7 showed increased mortality among patients who failed NIPSV. Considering some of these variables, close monitoring and expertise is strongly recommended when NIPSV is started in patients with a high risk of failure.
COPD patients who survive an initial episode of exacerbation needing NIV are at high risk for recurrent admission and subsequent requirement of NIV.Citation39 In a recent retrospective analysis of 100 COPD patients with respiratory acidosis treated with NIV, Chung et alCitation40 described a median survival of 2.08 years, with a mean survival rate at 2 and 5 years of 52% and 26%, respectively, significantly higher than in some studies from the 1990sCitation41 and closer to that described recently by Titlestad et al.Citation42 The only strong predictors of 5-year mortality were age, body mass index, and domiciliary oxygen use. Surprisingly, the degree of acute physiological impairment when NIV was initiated was not described as a predictor of long-term survival.Citation40
Home mechanical ventilation
In patients with chronic hypercapnic respiratory failure, long-term NIV can theoretically provide benefits by compensating nighttime hypoventilation, allowing respiratory muscles to rest, improving nocturnal gas exchange, and resetting central respiratory control in response to arterial partial carbon dioxide pressure (PaCO2) concentration. Sleep quality improves, as daytime symptoms and patient survival often do as well;Citation43,Citation44 however, the long-term benefit from home NIV in chronic stable COPD patients remains uncertain, and current trials are focused on elucidating which patients may benefit from domiciliary NIV and what is the best ventilatory strategy.Citation45 A recent meta-analysis including individual data from 245 stable hypercapnic COPD patients did not find any benefit in 3 or 12 months of nocturnal NIPSV other than a slight improvement of PaCO2 at 3 months’ follow-up, which was more pronounced when NIPSV was applied with inspiratory positive airway pressure (IPAP) levels of 18 cm H2O or higher.Citation46
To date, COPD patients remaining chronically hypercapnic after an acute exacerbation, with a greater alteration of nighttime ventilation and high adherence to the therapy, seem to be the best candidates for home ventilation.Citation44,Citation47 Regarding ventilatory modes, trials using low pressure levels in stable COPD patients failed to demonstrate improvement in PaCO2 and outcomes.Citation43,Citation48 Conversely, the use of high inspiratory pressures (20 to 40 cmH2O, known as high-pressure NIPSV) in an assisted or controlled mode (high pressures plus a respiratory rate beyond the spontaneous rate, known as high-intensity NIPSV) could play a role in the future, as some trials have shown good results.Citation43–Citation50 The reduction in cardiac output is more pronounced in high-intensity NIPSV,Citation51 and the clinical significance of this effect in patients with preexisting cardiovascular disease remains unknown.
ACPE
Either CPAP or NIPSV are used in ACPE.Citation52 Since 1985, numerous studies have proved the superiority of CPAP (mostly set at 10 cmH2O) over standard oxygen therapy in patients with ACPE, improving gas exchange and symptoms and reducing the EI rate.Citation53–Citation61 Some trialsCitation62,Citation63 have shown a reduction in the EI rate with NIPSV compared to standard therapy, especially in hypercapnic patients.Citation64 No superiority of one technique over the other was shown in clinical trials designed to compare both techniquesCitation65–Citation72 or in meta-analyses,Citation15,Citation73–Citation77 although NIPSV tended to show a faster improvement in ARF in some studies.
Despite the beneficial effects of NIV in ACPE, the impact on mortality still remains unclear. Several meta-analyses conducted in the middle of the last decadeCitation73–Citation75 showed a reduction in mortality with the use of CPAP; however, the Three Interventions in Cardiogenic Pulmonary Oedema (3CPO) trial,Citation78 the largest clinical trial on NIV carried out to date, including more than 1,000 patients and published in 2008, did not show differences in 30-day mortality between conventional therapy and NIV, either CPAP, or NIPSV. Although a subsequent meta-analysis including the 3CPO trial still showed a significant reduction of mortality rate with CPAP (relative risk =0.75 [0.61–0.92]),Citation76 the conflicting results compared to the large trial makes it difficult to formulate a clear conclusion on this issue.
Asthma
Although a favorable response to NIPSV would be anticipated in acute asthma, little evidence supports this application.Citation79–Citation83 Recent reviews concluded that there is not enough evidence to support the use of NIPSV in acute asthma and that medical treatment alone may usually be effective.Citation84,Citation85 The use of NIPSV for asthmatic patients who decline intubation and for selected patients who are likely to cooperate with mask therapy has been suggested, but more data are needed to generally recommend this approach.Citation86
Community-acquired pneumonia
The utility of NIV in patients with community-acquired pneumonia (CAP) is controversial because some data suggested that delaying EI with NIV could increase mortality;Citation87 however, several randomized clinical trials have compared the efficacy of NIV over COT in patients with CAP,Citation88–Citation90 reporting a significant reduction in EI rate, shorter ICU stay, and lower mortality, mainly in patients with COPD. Therefore, a trial of NIV may be recommended in these patients.
Weaning and postextubation respiratory failure
NIV has been used in patients with persistent weaning failure (patients in whom the spontaneous breathing trial failed during three consecutive attempts)Citation91 as adjunct to early liberation from IMV by shortening the time of IMV and the length of stay and lowering the incidence of complications (ventilator-associated pneumonia or septic shock).Citation92–Citation99 Early extubation and immediate application of NIV when patients meet weaning criteria can be a useful approach to increase weaning success rates and may reduce mortality in COPD patients, but it should be used with caution, as there is no strong evidence in terms of avoiding reintubation, even in the subgroup of patients with COPD.Citation100
NIPSV can also be used after planned extubation in patients at high risk of deterioration () as it could prevent postextubation ARF and reintubation.Citation93–Citation95,Citation101 Recently, Ornico et alCitation102 showed a reduction of reintubation rates when nasal NIV was applied immediately after planned extubation (in contrast to oxygen mask) in a small group of nonselected patients with more than 3 days with ARF needing IMV. The reintubation rate in the oxygen group was high (39%), a fact that could be explained by the particular weaning protocol used in this study. More relevant was the finding that patients weaned by using NIV had a significantly lower hospital mortality compared with patients weaned by using COT. These promising results should be confirmed in larger, multicenter, randomized trials.
Table 2 Risk factors for postextubation respiratory failure
Regarding the role of NIV in treating established ARF during the postextubation period (generally 48–72 hours after extubation), no trial has reported benefits.Citation103,Citation104 One multicenter studyCitation104 even found slightly higher mortality in the NIV group, which was attributed to delayed reintubation (12 hours versus 2.5 hours). This is the main argument as to why current guidelines suggest that NIV should not be routinely used in patients who have postextubation ARF.Citation105
Other indications
Acute lung injury/acute respiratory distress syndrome
Clinical studies and meta-analyses have shown negative results with the use of NIV or CPAP in acute lung injury (ALI)/acute respiratory distress syndrome (ARDS).Citation106–Citation108 The delay in EI may be associated with major complications. However, patients with initial ALI/ARDS (no multiple organ failure or hemodynamic instability) may be treated with NIV, avoiding EI in nearly 50% of cases.Citation109
Immunocompromised patients
The use of NIV in ARF of different etiologies in immunocompromised patients (patients receiving immunosuppressive therapy for solid organ or bone marrow transplantCitation110,Citation111) is well supported in terms of significant reduction of EI and in-hospital mortality rates. The benefits of NIV compared with other ventilatory approaches in patients who have hematological malignancies is controversial, and further research is needed to clarify the role of NIV as respiratory support in ARF in hematologic patients.Citation112–Citation116
Postoperative respiratory failure
NIV may be used in the postoperative setting to either prevent or treat ARF. Although it is not clear whether NIV and CPAP may be useful in preventing ARF after low- and high-risk surgical procedures,Citation105,Citation117–Citation119 it has been successfully used in patients with ARF, presented after abdominal or lung-resection surgery and reducing EI rate.Citation120,Citation121
Palliative NIV
Palliative NIV can either be administered to offer a chance for survival or to alleviate the symptoms of respiratory distress in terminal patients.Citation122 Among patients given NIV for ARF related to reversible causes, nearly one-half survived and returned home.Citation122,Citation123 The use of NIV in patients with dyspnea in terminal states is controversial, but it is effective in reducing dyspnea and in decreasing the dose of morphine in palliative use in patients with end-stage cancer.Citation124 The preservation of communication between the patient and the family is considered one of the main benefits of NIV in this setting. The technique is widely used in patients with ARF and a do-not-intubate order, with frequent use (between 25% and 100% of cases) reported by 50% of European physicians.Citation125
Chest trauma
A recent meta-analysis including ten studies with patients with chest trauma found that NIV significantly improved oxygenation and reduced EI, length of ICU stay, and mortality (3% deaths in the NIV group compared to 22.9% in the control group). In seven of the studies, NIV was used to treat ARF, while in the others it was used for ARF prevention.Citation126
Chest wall and neuromuscular disorders
Home NIV can be used in conditions that can lead to chronic ventilatory failure such as scoliosis, kyphosis, thoracoplasty, muscular dystrophy (Duchenne muscular dystrophy, myotonic dystrophy, or poliomyelitis), and motor neuron diseases (amyotrophic lateral sclerosis). NIV may improve symptom control and quality of life in some of these patients. If bulbar function is impaired, tracheostomy ventilation may be required, but, in other cases, NIV is preferable.Citation127 Its use in rapid progressive neurological disease is, however, controversial, as it could simply protract the dying process rather than extend good quality of life.Citation127 In the acute setting, NIV should be used with caution in patients with rapidly progressive neuromuscular disease syndromes such as myasthenia gravis or Guillain–Barré syndrome, especially when bulbar muscles are involved,Citation128 but it can be used to treat acute decompensation of chronic respiratory failure (ie, respiratory infection).
During bronchoscopy
Although successful experiences in selected centers have been reported, the feasibility and safety of diagnostic and therapeutic bronchoscopy in NIV is not well known and further studies are needed to clarify its impact on intubation rates and mortality in high-risk, critically ill patients.Citation129
Obesity hypoventilation syndrome
NIV is considered a significant treatment option for patients with obesity hypoventilation syndrome (OHS). Some studies have suggested that treatment of OHS with NIV restores sleep quality and daytime vigilance and reduces cardiovascular morbidity,Citation130 although it is not clear which is the best choice of equipment and ventilator settings.Citation130–Citation132 On the other hand, patients with OHS often present exacerbations of respiratory symptoms that, like COPD with progressive hypercapnia, require hospitalization and ventilatory support. By using NIV in a similar protocol to that in patients with severe COPD exacerbation, it is effective in reducing respiratory acidosis and improving respiratory rate.Citation132,Citation133
Obstructive sleep apnea
CPAP is the first-line treatment for moderate-to-severe obstructive sleep apnea (OSA) because it eliminates obstructive apneic/hypopneic events, resulting in improved daytime symptoms and possibly reducing adverse cardiovascular outcomes.Citation132 On the other hand, it has been reported that nearly 50% of patients with chronic heart failure have sleep-disordered breathing, which consists of OSA caused by upper airway obstruction during sleep and Cheyne–Stokes respiration with central sleep apnea caused by respiratory control system instability. In these patients, the use of NIV (adaptive servoventilation) to compensate both abnormalities has been proposed.Citation134
Modes of NIV
As previously mentioned, there are two major modes of NIV: CPAP and NIPSV, but many other modes have been used and some of them may have a relevant role in the future. An epidemiologic survey that included patients who received NIPSV for ARF found that pressure support with or without positive end-expiratory pressure (PEEP) was used in 67% of cases and CPAP was used in 18%.Citation135
CPAP
Although it was introduced earlier in medical practice, it is not essentially a “true” ventilation mode because it does not provide any inspiratory support.Citation136 CPAP can be generated with a simple oxygen source through a hermetical mask with a PEEP valve or a Boussignac® (Vygon SA., Ecouen, France) mask, which hold a quantity of air in the lungs on expiration. The continuous positive intrathoracic pressure recruits collapsed alveolar units and increases functional residual capacity and lung compliance, improving oxygenation and the work of breathing.Citation52 Control of fraction of inspired oxygen (FiO2) can be difficult, however, unless a mixer or a ventilator is used.
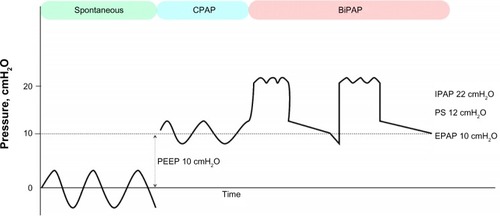
NIPSV
Unlike CPAP, this modality requires a ventilator. It is usually programmed with two levels of pressure: expiratory pressure (expiratory positive airway pressure [EPAP] or PEEP, similar to CPAP) and IPAP (). When the patient starts the inspiratory effort, the ventilator delivers inspiratory assistance with pressure support using a decelerated flow, which keeps IPAP constant. When the patient finishes the inspiratory effort or the inspiratory flow descends below a preset percentage of its maximum value (usually 25%–30%), the pressure support is discontinued and the pressure drops down to the predetermined EPAP. In the vast majority of NIV studies in the acute setting, the modality used is NIPSV, and this is, by far, the most used modality in acute exacerbations of COPD.
Figure 1 Pressure-time curves.
Abbreviations: BiPAP, bilevel positive airway pressure; CPAP, continuous positive airway pressure; EPAP, expiratory positive airway pressure; IPAP, inspiratory positive airway pressure; PEEP, positive end-expiratory pressure; PS, pressure support.
Other modalities
Assist-control pressure ventilation
Two levels of pressure (EPAP or PEEP and IPAP) are delivered as in NIPSV but at a preset respiratory rate. This is the modality used in high-intensity NIV.
Proportional assist ventilation
The inspiratory support is regulated by analyzing the elasticity and resistance of the patient, delivering an assisted ventilation proportional to the patient’s effort. Target volume or pressure are not preset. Although this modality has demonstrated a better patient–ventilator synchrony,Citation136,Citation137 this advantage has not been translated into clinical outcomes.Citation138–Citation140
High-flow nasal cannula
Like CPAP, HFNC does not provide inspiratory support. The system delivers an oxygen–gas mixture that may meet or exceed patients’ spontaneous inspiratory demand, which may be up to 35 liters in adult patients with ARF. The main difference between high-flow nasal cannula (HFNC) and NIPSV is that HFNC maintains a fixed flow and generates variable pressures depending on the patient’s respiratory pattern, while NIPSV provides a variable flow to generate a fixed pressure. Three action mechanisms of HFNC are postulated: first, a washout effect in nasopharyngeal dead space, simulating the benefits of tracheal gas insufflation; second, a reduction of upper airway resistance, which constitutes nearly 50% of total airway resistance; and third, a low level of positive intrathoracic pressure.Citation141 HFNC can be effectively and safely applied in neonates with respiratory distress, children with bronchiolitis, and adults with mild-to-moderate hypoxemic respiratory failure. However, no definitive data support that HFNC is equivalent or superior to CPAP and the utility of HFNC as an alternative to CPAP requires further randomized trials.
Neurally adjusted ventilatory assist
This modality is implemented in some ventilators and is generally used to facilitate weaning in intubated patients; however, it has also been used as a form of NIV. The device uses a neural signal, the electrical diaphragm activity, to trigger and cycle off the ventilator, as well as to adapt the amount of pressure delivered. This signal occurs earlier than any flow or pressure variation,Citation142,Citation143 and pressure is cycled off when diaphragm activity ends.Citation144 Neurally adjusted ventilatory assist (NAVA) improves patient– ventilation synchrony and has been shown to be superior to NIPSV by decreasing ineffective efforts and premature and delayed cyclings.Citation142,Citation144 The impact in relevant outcomes remains unclear, however, and the mode has important limitations: first, the system needs the insertion of an esophageal catheter; second, changes in patient position can deteriorate the signal; third, the neural drive may be affected in some diseases or with sedation; and fourth, high NAVA gains may cause an irregular respiratory pattern.
Adaptive pressure control
Adaptive pressure control, or average volume-assured pressure support, consists of an adaptive targeting scheme to adjust the inspiratory pressure to deliver at least a minimum target tidal volume.Citation145 The ventilator provides progressively higher or lower pressure support ventilation, according to the patient’s inspiratory effort and tidal volume. Depending on the ventilator, this modality has different names (AutoFlow [Evita® XL; Dräger, Lübeck, Germany]; VC+ [Puritan Bennett™ 840; Covidien plc, Dublin, Ireland]; APV [GALILEO; Hamilton Medical AG, Bonaduz, Switzerland]; PRVC [Servo-i and Servo 300; Maquet, Bridgewater, NJ, USA]; and average volume-assured pressure support [BiPAP Synchrony; Philips Medical Systems, Cleveland, OH, USA]), with little differences in their algorithms.Citation145,Citation146 In the acute setting, adaptive pressure control has been used in adults with COPD and severe hypercapnic encephalopathy (Glasgow Coma Scale score <10), showing better clinical and gasometrical improvement than NIPSV.Citation146
Adaptive servoventilation
Some modern home ventilators have the capability to compensate central apneas with periodic breathing by regulation of the inspiratory and expiratory pressure, treating upper airway obstruction by auto-adjustment of the end-EPAP.Citation147 This modality has been successfully used to improve sleep disturbances in patients with chronic heart failure in whom central and peripheral apneas are frequent,Citation148 and in patients with complex sleep apnea syndrome, characterized by the development of frequent central apneas or a Cheyne–Stokes respiratory pattern after initial application of CPAP.Citation147
Negative pressure ventilation
There are few groups still using this modality, usually with a cuirass or jacket (poncho), to support patients with chest wall disorders.Citation127
Interfaces
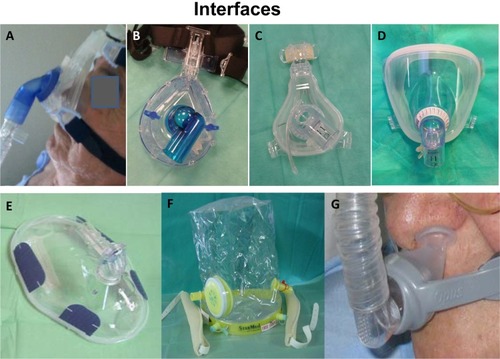
Whatever NIV technique is used, an interface is needed to connect the patient to a ventilator or to an air/oxygen source (). Interfaces are devices that connect the ventilator tubing to the patient’s face and facilitate the entry of pressurized gas into the upper airway. Interface-related problems are, by far, the most common reason for NIV intolerance. Patient comfort and synchrony are essential when choosing an interface, as internal volume is not related to effective dead space when NIPSV is delivered.Citation149
Figure 2 Interfaces for noninvasive ventilation.
Nasal interface
It has been the most commonly used interface in chronic respiratory failure (73%), followed by nasal pillow, facial masks, and mouth pieces,Citation150 this trend is changing with the application of new modes of home NIV, which are usually applied with a face mask.Citation47,Citation51 Nasal masks are less useful in acute critical situations, generating more resistanceCitation151,Citation152 and massive leakage through the mouth, often requiring mask change.Citation153 On the other hand, they permit speech, feeding, coughing, and expectoration, reducing the risk of vomiting.Citation150 Nasal pillows are a variant that are inserted into the nostrils; these are commonly used in pediatric patients.
Face masks
Face masks are the most common interface in clinical practice in Europe, used in over 70% of all patients requiring NIV.Citation154 Disadvantages include lack of protection from vomiting, nasal skin injuries, nasal congestion, mouth dryness, eye irritation, speaking difficulty, and possible claustrophobia.Citation153 There are two types of face masks.
Oronasal masks
An oronasal mask covers the mouth and nose. It increases minute ventilation and reduces PaCO2 more effectively than nasal masks in COPD patients.Citation151 It is the most frequently used interface in Europe,Citation154 being indicated specifically in mouth-breathing patients with dyspnea. Different sizes and models are necessary to ensure a correct adaptation to the patient.
Total/full-face masks
A total/full-face mask covers the mouth, nose, and eyes. In general, little cooperation is required to achieve a correct adaptation, with easy fitting and application, and this type of mask provokes fewer skin injuries compared to oronasal masks.Citation155,Citation156 They may be more comfortable than oronasal masks in longer treatments,Citation157,Citation158 although their superiority has not been demonstrated.Citation147,Citation159 As total face masks are probably the best tolerated, they may become an alternative in cases in which mask intolerance is the primary reason for failing NIV and should be available in units where NIV is routinely applied.Citation157
Helmet
A helmet covers the whole head and part of the neck. It seems to provide some advantages over other interfaces: it is well tolerated by patients, allows acceptable interaction with the environment, and can be used in difficult anatomic situations, such as in patients who are edentulous or have facial trauma. In contrast to facial masks, helmets do not make contact with the patient’s face and therefore do not cause skin lesions.Citation17 The helmet allows more patient autonomy (speaking, reading, and eating), but the noise can be annoying.Citation160 The use of the helmet is not recommended with traditional ventilators, as a fresh gas flow high enough to minimize rebreathing is necessary.Citation160 It is more appropriate for CPAP because the increased dead space may generate asynchrony when NIPSV is applied.Citation43,Citation161,Citation162
Other
Mouthpieces placed between lips and held in place by lip seals are less effective due to higher leakage and asynchrony rates and greater patient discomfort.Citation163,Citation164 Mouth pieces and nasal pillows can be applied as a rotating strategy with other interfaces.
Ventilators
There are three types of ventilators for NIPSV: portable ventilators designed specifically for NIV; transport ventilators; and ICU ventilators. Classical ICU ventilators (connected to air and oxygen gas sources) and transport ventilators (connected to an oxygen source) were primarily configured to be used with EI, and provided different levels of monitoring and security alarm systems, but often failed during NIPSV when leaks were present. Modern ICU ventilators and some transport ventilators have solved this drawback by incorporating NIV algorithms.
In contrast with ICU ventilators, NIV ventilators are more economical, easily portable, and do not need an airflow source. A wide range of portable ventilators is currently on the market, from the most simple (only pressure is modifiable) to the latest generation of high-tech ventilators (monitoring, alarm setting, leakage compensation, different triggers, cycling and flow ramp control, etc),Citation165 which allow better synchrony than ICU and transport ventilators, including even those with adapted NIV algorithms.Citation165
The most important attribute of the equipment is leakage compensation by means of an increase of airflow (up to 120–180 L/minute), which maintains tidal volume, producing better patient–ventilator synchrony and higher system efficacy. Since pressure cycling can increase auto-PEEP, trigger is usually activated with airflow.Citation166
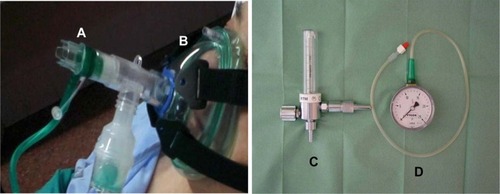
All the ventilators have particular settings for CPAP. Furthermore, CPAP can be applied without a ventilator using the Boussignac mask. The oxygen flows through small-diameter channels in cylinder walls and is injected at high speed into the cylinder through angled side channels. The resulting turbulence, together with air friction, creates pressure on the patient’s side cylinder opening, acting as a flow barrier or virtual PEEP valve. This is a very simple technique that may be used in areas with little equipment ().Citation167
Figure 3 Equipment needed for continuous positive airway pressure Boussignac technique.
Humidification
NIV is often applied without humidifying devices, because inspired gases are heated and humidified on the way to the alveoli; however, dry gas provokes dryness of the mouth, nose, and respiratory tract, resulting in nasal congestion and an increase of airway resistance during NIV. Up to 60% of patients with sleep apnea syndrome using nasal CPAP experience nasal congestion and dryness of the nose, mouth, and throat.Citation168 Consensus statements and guidelines for NIV contain conflicting recommendations concerning humidification.Citation169 When it is applied, heat humidification is recommended because it seems to facilitate NIVCitation170,Citation171 by reducing nasal resistance, aiding expectoration, and improving adherence and comfort,Citation168 especially in patients with respiratory secretions. Heat and moisture exchangers are not indicated when using NIV, since they may increase circuit dead space (increased PaCO2) and the work of breathing.Citation172,Citation173
Where to apply NIV
The clinical benefits of NIV are so relevant in treating some patients with ARF that its use has been extended out of the ICU and into patient location.
Numerous experiences have been reported in studies showing the feasibility and lack of complications using CPAP to treat ACPE in out-of-hospital emergencies,Citation11,Citation174,Citation175 with improvement in short-term outcomes.Citation175
Predictors of failure and complications
Before starting NIV, it is crucial to identify if the patient is a good candidate. There is a therapeutic window in which NIV should be used, avoiding those patients with mild ARF that would easily respond to COT or, conversely, those who present very severe ARF needing EI.Citation171 It is necessary to consider predictors of failure () that warrant closer monitoring, paying attention to possible complications like hypotension, pneumothorax, gastric insufflation, and vomiting, with the risk of aspiration pneumonia. Intubation may be preferred if the likelihood of NIV failure is very high. Subjects who have a pH <7.25, an Acute Physiology and Chronic Health Evaluation (APACHE) II score >29, and a Glasgow Coma Scale score <11 have failure rates ranging from 64% to 82%.Citation170,Citation171,Citation180 Patients with excessive respiratory secretions or without improvement after 60 minutes of NIV may also be at high risk of failure.Citation29,Citation181–Citation183 Clinical signs that are only equivocal on presentation become more definitively predictive of failure if they persist after 2 hours of NIV.Citation180
Table 3 Predictors of failure of noninvasive ventilation therapy in acute respiratory failure
In our experience, there are three levels that may influence NIV success: the patient (cause of ARF, patient condition, adaptation to NIV); the physician (concomitant therapy, expertise in the use of NIV, team attitude); and the device (ventilator sets, adequate interface, monitoring equipment).
Practical aspects
Clear instructions and frequent encouraging stimuli should be given to all patients at the beginning of treatment, often while fitting the mask manually.
Ventilator settings
Although clinical guidelines and reviews recommend starting with low levels of pressure (IPAP: 8–10 cmH2O; EPAP: 3–4 cmH2O) and increasing pressure support progressively according to patient adaptation, ensuring expired tidal volumes >4–6 mL/kg (it can be lower in COPD patients), there are no clinical trials that address the best way to start and continue NIPSV. In our experience, these initial parameters are well tolerated at the onset; later, with a pressure support of 12–18 cmH2O above PEEP, a tidal volume of 400–500 mL is commonly reached. Elevated pressures may cause excessive air leakage, asynchrony (especially when the patient is tachypneic), and discomfort. On the other hand, a PEEP over 4 cmH2O is necessary to avoid rebreathing when using portable ventilators, which may not include an expiratory valve or double inspiratory/expiratory circuit.Citation184 FiO2 should be titrated to achieve the desired oxygen saturation by pulse oximetry (>95% in general).
Monitoring NIV
Visualization of flow and pressure waveforms on the display is strongly recommended. In a recent study, physicians obtained a more rapid pH normalization in patients needing NIV for COPD exacerbation, with a faster PaCO2 reduction in the first 6 hours of ventilation, than just controlling numerical variables on the display, although the NIV success rate was not affected by this ventilatory approach.Citation185
To ensure the success of NIV, close monitoring is necessary, especially of respiratory rate (patient’s effort), oxygen saturation (to adjust FiO2), and pH and PaCO2 (to assess efficacy). In addition to continuous observation, overall reassessments are usually performed at 60 and/or 90–120 minutes. One of the key factors determining tolerance to NIV (and its success) is optimal synchrony between the patient’s spontaneous breathing activity and the ventilator’s set parameters, known as “patient–ventilator interaction”. The modality of pressure support ventilation unavoidably induces a certain degree of asynchrony, even in intubated patients.Citation186 Asynchrony Index (AI) is calculated as follows:
An AI >10% is considered severe, leading to an increase in the work of breathing and patient discomfort.Citation186 Although several mechanisms may be responsible for asynchrony, air leakage is involved in many of them. In general, a leak of <0.4 L/second (,25 L/minute) is well tolerated. Asynchrony is usually manifested in different forms that each require specific approaches.
Trigger asynchrony
Trigger asynchrony is manifested in the form of ineffective efforts, double triggering, and auto-triggering. These asynchronies should be managed by tuning the trigger, adjusting the level of pressure support, and reducing the leakage.
Flow asynchrony
Flow asynchrony is manifested when rising time and flow cycle are not in accordance with patient’s demand. A shorter rise time and higher flow cycle should be considered in patients with tachypnea, while slower rise time may be more comfortable in patients with low respiratory drive.
Cycle asynchrony
Short cycle (premature cycling off)
Many ventilators have cycling off set at 25%–30% of the peak inspiratory flow. By titrating the expiratory trigger, the duration of the cycle may be regulated. In COPD patients, it is often set at 50%.Citation185
Prolonged cycle (delayed cycling off)
A prolonged cycle is a cycle with a mechanical inspiratory time greater than the patient’s inspiratory time. The reduction of air leaks and/or titration of expiratory trigger, as well as setting of maximal inspiratory time, are actions that may compensate this asynchrony.
Auto-PEEP
In auto-PEEP, the flow curve does not reach 0 at the end of expiration and titration of PEEP (at least until 85% in COPD patients) is required to compensate this.
As a general rule, measures to reduce asynchrony should be taken by changing pressure support by steps of 2 cmH2O, and inspiratory and expiratory triggers by steps of 5% to 10%.Citation185
The use of sedation
Although sedation can play a role in preventing intolerance to NIV, it is also potentially dangerous because of the risk of oversedation. The sedation and analgesic regimens that physicians prefer to use during NIV are quite varied. Benzodiazepines (33%) and opiates (29%) are reported to be the most often selected sedative agents for NIV.Citation125 Morphine, remifentanil, dexmedetomidine, propofol, and midazolam-based regimens have all been used with no serious complications in experienced units.Citation187,Citation188 The new α2 adrenoreceptor agonist dexmedetomidine showed similar clinical results to midazolam in decompensated COPD with fewer adjustments in its dose,Citation189 and it was superior to midazolam in patients with ACPE intolerant to NIV.Citation187
When to stop
NIV is usually stopped when a satisfactory recovery has been achieved or, conversely, when there are signs of NIV failure. If NIV has been successful, the next step depends on the cause and duration of NIV. In mid- or long-term use, a weaning period is often carried out, which involves decreasing PEEP and ventilatory settings progressively. The application of a protocol-directed weaning has shown clear advantages in this context.Citation190 This approach does not seem to be necessary in short-term use. If the patient deteriorates when NIV is interrupted, the therapy is resumed, but, otherwise, NIV may be discontinued.Citation180
Conclusion
NIV is the first option for ventilatory support in ARF of COPD exacerbations or ACPE and should be considered in immunocompromised patients, difficult weaning, and the prevention of postextubation failure. It can also be used in the postoperative period and in cases of pneumonia and asthma or as a palliative treatment. NIV is currently used in a wide range of settings, from the ICU to home care. The appropriate selection of patients and the capacity of the team and the patients to achieve a proper adaptation to the technique are the bottom line for success. Despite no significant technological discoveries in the area of ARF in recent years, new ventilatory modes and interfaces have recently been introduced and others are under development to optimize hospital care, home ventilation, and the control of sleep disorders, further expanding the role of NIV in the health system. In conclusion, NIV should currently be considered in the treatment of the majority of patients with ARF failure.
Disclosure
The authors report no conflicts of interest in this work.
References
- HillbergREJohnsonDCNoninvasive ventilationN Engl J Med1997337174617529392701
- MehtaSHillNSNoninvasive ventilationAm J Resp Crit Care Med200116354057711179136
- GirouEBrun-BuissonCTailléSLemaireFBrochardLSecular trends in nosocomial infections and mortality associated with noninvasive ventilation in patients with exacerbation of COPD and pulmonary edemaJAMA20032902985299114665660
- GirouESchortgenFDelclauxCAssociation of noninvasive ventilation with nosocomial infections and survival in critically ill patientsJAMA20002842361236711066187
- BrochardLIsabeyDPiquetJReversal of acute exacerbations of chronic obstructive lung disease by inspiratory assistance with a face maskN Eng J Med199032315231530
- MeduriGUConoscentiCCMenashePNairSNoninvasive face mask ventilation in patients with acute respiratory ventilationChest1989958658702924616
- ChandraDStammJATaylorBOutcomes of noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease in the United States, 1998–2008Am J Respir Crit Care Med2012185215215922016446
- Jois-BilowichPDiercksDEmergency department stabilization of heart failureHeart Fail Clin20095374219026384
- FarhaSGhamraZHoisingtonERButlerRSStollerJKUse of noninvasive positive-pressure ventilation on the regular hospital ward: experience and correlates of successRespir Care2006511237124317067405
- CuomoADelmastroMCerianaPNoninvasive mechanical ventilation as a palliative treatment of acute respiratory failure in patients with end-stage solid cancerPalliat Med20041860261015540668
- DeisJNAbramoTJCrawleyLNoninvasive respiratory supportPediatr Emerg Care20082433133818496121
- WeitzGStruckJZonakABalnusSPerrasBDodtCPrehospital noninvasive pressure support ventilation for acute cardiogenic pulmonary edemaEur J Emerg Med20071427627917823565
- PlaisancePPirracchioRBertonCVicautEPayenDA randomized study of out-of-hospital continuous positive airway pressure for acute cardiogenic pulmonary oedema: physiological and clinical effectsEur Heart J2007282895290117967821
- LightowlerJVWedzichaJAElliottMWRamFSNoninvasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysisBMJ200332618518912543832
- MasipJRoqueMSánchezBFernándezRSubiranaMExpósitoJNoninvasive ventilation in acute cardiogenic pulmonary edema. Systematic review and meta-analysisJAMA20052943124313016380593
- NavaSHillNNon-invasive ventilation in acute respiratory failureLancet200937425025919616722
- PeñuelasOFrutos-VivarFEstebanANoninvasive positive-pressure ventilation in acute respiratory failureCMAJ2007177101211121817984471
- BottJCarrollMPConwayJHRandomized controlled trial of nasal ventilation in acute ventilatory failure due to chronic obstructive airways diseaseLancet1993341155515578099639
- BrochardLManceboJWysockiMNoninvasive ventilation for acute exacerbations of chronic obstructive pulmonary diseaseN Engl J Med19953338178227651472
- AngusRMAhmedAAFenwickLJPeacockAJComparison of the acute effects on gas exchange of nasal ventilation and doxapram in exacerbation of chronic obstructive pulmonary diseaseThorax199651104810508977608
- CelikelTSungurMCeyhanBKarakurtSComparison of noninvasive positive pressure ventilation with standard medical therapy in hypercapnic acute respiratory failureChest1998114163616429872200
- PlantPKOwenJLElliottMWEarly use of non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards: a multicentre randomised controlled trialLancet20003551931193510859037
- Collaborative Research Group of Noninvasive Mechanical Ventilation for Chronic Obstructive Pulmonary DiseaseEarly use of non-invasive positive pressure ventilation for acute exacerbations of chronic obstructive pulmonary disease: a multicentre randomized controlled trialChin Med J (Engl)20051182034204016438899
- KeenanSPSinuffTCookDJHillNSWhich patients with acute exacerbation of chronic obstructive pulmonary disease benefit from noninvasive positive-pressure ventilation? A systematic review of the literatureAnn Intern Med200313886187012779296
- CaplesSGayPCNoninvasive positive pressure ventilation in the intensive care unit: a concise reviewCrit Care Med2005332651265816276193
- KeenanSPKernermanPDCookDJMartinCMMcCormackDSibbaldWJEffect of noninvasive positive pressure ventilation on mortality in patients admitted with acute respiratory failure: a meta-analysisCrit Care Med199725168516929377883
- PeterJVMoranJLPhillips-HughesJWarnDNoninvasive ventilation in acute respiratory failure: a meta-analysis updateCrit Care Med20023055556211990914
- RamFSPicotJLightowlerJWedzichaJANon-invasive positive pressure ventilation for treatment of respiratory failure due to exacerbations of chronic obstructive pulmonary diseaseCochrane Database Syst Rev20043CD004104
- AntónAGüellRGómezJPredicting the result of noninvasive ventilation in severe acute exacerbations of patients with chronic airflow limitationChest200011782883310713013
- EvansTWInternational Consensus Conferences in Intensive Care Medicine: non-invasive positive-pressure ventilation in acute respiratory failure. Organised jointly by the American Thoracic Society, the European Respiratory Society, the European Society of Intensive Care Medicine, and the Société de Réanimation de Langue Française, and approved by the ATS Board of Directors, Dec 2000Intensive Care Med20012716617811280630
- British Thoracic Society Standards of Care CommitteeNon-invasive ventilation in acute respiratory failureThorax20025719221111867822
- Organized jointly by the American Thoracic Society, the European Respiratory Society, the European Society of Intensive Care Medicine, and the Société de Réanimation de Langue Française, and approved by ATS Board of Directors, December 2000International Consensus Conferences in Intensive Care Medicine: noninvasive positive pressure ventilation in acute respiratory failureAm J Respir Crit Care Med200116328329111208659
- BarbéFTogoresBRubiMPonsSMaimóAAgustíAGNoninvasive ventilatory support does not facilitate recovery from acute respiratory failure in chronic obstructive pulmonary diseaseEur Respir J19969124012458804944
- KeenanSPPowersCEMcCormackDGNoninvasive positive-pressure ventilation in patients with milder chronic obstructive pulmonary disease exacerbations: a randomized controlled trialRespir Care20055061061615871754
- NavaSNavalesiPContiGTime of non-invasive ventilationIntensive Care Med20063236137016477416
- SquadroneEFrigerioPFogliatiCNoninvasive vs invasive ventilation in COPD patients with severe acute respiratory failure deemed to require ventilatory assistanceIntensive Care Med2004301303131015197438
- SchettinoGAltobelliNKacmarekRMNoninvasive positive-pressure ventilation in acute respiratory failure outside clinical trials: Experience at the Massachusetts General HospitalCrit Care Med20083644144718091540
- DemouleAGirouERichardJCTailléSBrochardLIncreased use of noninvasive ventilation in French intensive care unitsIntensive Care Med2006321747175516799775
- DwarakanathAElliottMWNoninvasive ventilation in the management of acute hypercapnic respiratory failureBreathe201395338348
- ChungLPWinshipPPhungSLakeFWatererGFive-year outcome in COPD patients after their first episode of acute exacerbation treated with non-invasive ventilationRespirology2010151084109120573056
- VitaccaMCliniERubiniFNavaSFoglioKAmbrosinoNNon-invasive mechanical ventilation in severe chronic obstructive lung disease and acute respiratory failure: short- and long-term prognosisIntensive Care Med199622941008857115
- TitlestadLLassenATVestboJLong-term survival for COPD patients receiving noninvasive ventilation for acute respiratory failureInt J Chron Obstruct Pulmon Dis2013821521923650445
- WindischWNoninvasive positive pressure ventilation in COPDBreathe20118114123
- AntónAGüellRHome mechanical ventilation in COPD: do we know when and how to use it?Chest200011861525152611115429
- EsquinasAMSiscaroGCliniEMNoninvasive mechanical ventilation with high pressure strategy remains a “double edged sword”?Int J Chron Obstruct Pulmon Dis2013825525623818774
- StruikFMLacasseYGoldsteinRSKerstjensHAWijkstraPJNocturnal nonninvasive positive pressure ventilation in stable COPD: A systematic review and individual patient data meta-analysisRespiratory Medicine201410832933724157199
- BudweiserSHitzlAPJörresAImpact of noninvasive home ventilation on long-term survival in chronic hypercapnic COPD: a prospective observational studyInt J Clin Pract2007611516152217686094
- CasanovaCCelliBRTostLLong-term controlled trial of nocturnal nasal positive pressure ventilation in patients with severe COPDChest200011861582159011115443
- MurphyPBBrignallKMoxhamJPolkeyMIDavidsonACHartNHigh pressure versus high intensity noninvasive ventilation in stable hypercapnic chronic obstructive pulmonary disease: a randomized crossover trialInt J Chron Obstruct Pulmon Dis2012781181823271905
- FunkGCBreyerMKBurghuberOCLong-term non-invasive ventilation in COPD after acute-on-chronic respiratory failureRespir Med201110542743421111590
- LukácsovitsJCarlucciAHillNPhysiological changes during low- and high-intensity noninvasive ventilationEur Respir J20123986987521885393
- MasipJPlanasKNoninvasive ventilationTubaroMDanchinNFilippatosGGoldsteinPVranckxPZahgerDThe ESC Textbook of Intensive and Acute Cardiac CareOxfordOxford University Press2011215226
- LinMYangYFChiangHTChangMSChiangBNCheitlinMDReappraisal of continuous positive airway pressure therapy in acute cardiogenic pulmonary edema. Short-term results and long-term follow-upChest1995107137913867750335
- KellyCANewbyDEMcDonaghTARandomised controlled trial of continuous positive airway pressure and standard oxygen therapy in acute pulmonary oedema; effects on plasma brain natriuretic peptide concentrationsEur Heart J2002231379138612191749
- MoritzFBenichouJVanhesteMBoussignac continuous positive airway pressure device in emergency care of acute cardiogenic pulmonary oedema: a randomized pilot studyEur J Emerg Med20031020420812972896
- CraneSDElliottMWGilliganPRichardsKGrayAJRandomised controlled comparison of continuous positive airways pressure, bilevel noninvasive ventilation, and standard treatment in emergency department in patients with acute cardiogenic oedemaEmerg Med J20042115516114988338
- RäsänenJHeikkläJDownsJNikkiPVäisänenIViitanenAContinuous positive airway pressure by face mask in acute cardiogenic pulmonary edemaAm J Cardiol1985552963003881920
- BerstenADHoltAWVedigAESkowronskiGABaggoleyCJTreatment of severe cardiogenic pulmonary edema with continuous positive airway pressure delivered by face maskN Engl J Med1991325182518301961221
- TakedaSNejimaJTakanoTEffect of nasal continuous positive airway pressure on pulmonary edema complicating acute myocardial infarctionJpn Circ J1998625535589741730
- L’HerEDuquesneFGirouENoninvasive continuous positive airway pressure in elderly cardiogenic pulmonary edema patientsIntensive Care Med20043088288814991092
- ParkMSangeanMCVolpe MdeSRandomized, prospective trial of oxygen, continuous positive airway pressure, and bilevel positive airway pressure by face mask in acute cardiogenic pulmonary edemaCrit Care Med2004322407241515599144
- MasipJBetbeséAJPáezJNon-invasive pressure support ventilation versus conventional oxygen therapy in acute cardiogenic pulmonary oedema: a randomised trialLancet20003562126213211191538
- LevittMAA prospective, randomized trial of BiPAP in severe acute congestive heart failureJ Emerg Med20012136336911728761
- NavaSCarboneGDiBattistaNNoninvasive ventilation in cardiogenic pulmonary edema: a multicenter randomized trialAm J Respir Crit Care Med20031681432143712958051
- MehtaSJayGDWoolardRHRandomized, prospective trial of bilevel versus continuous positive airway pressure in acute pulmonary edemaCrit Care Med1997256206289142026
- MoritzFBrousseBGelléeBContinuous positive airway pressure versus bilevel noninvasive ventilation in acute cardiogenic pulmonary edema: a randomized multicenter trialAnn Emerg Med20075066667517764785
- LieschingTNelsonDCormierKLRandomized Trial of Bilevel versus Continuous Positive Airway Pressure for Acute Pulmonary EdemaJ Emerg Med201446113014024071031
- BelloneAMonaniACortellaroFVettorelloMArlatiSCoenDMyocardial infarction rate in acute pulmonary edema: noninvasive pressure support ventilation versus continuous positive airway pressureCrit Care Med2004321860186515343013
- BelloneAVettorelloMMonariACortellaroFCoenDNoninvasive pressure support ventilation vs continuous positive airway pressure in acute hypercapnic pulmonary edemaIntensive Care Med20053180781115871011
- RusterholtzTBollaertPEFeisselMContinuous positive airway pressure vs proportional assist ventilation for noninvasive ventilation in acute cardiogenic pulmonary edemaIntensive Care Med20083484084618214425
- HoKMWongKA comparison of continuous and bi-level positive airway pressure non-invasive ventilation in patients with acute cardiogenic pulmonary oedema: a meta-analysisCrit Care200610R4916569254
- NouiraSBoukefRBouidaWNon-invasive pressure support ventilation and CPAP in cardiogenic pulmonary edema: a multicenter randomized study in the emergency departmentIntensive Care Med20113724925621136039
- PeterJVMoranJLPhillips-HughesJGrahamPBerstenADEffect of non-invasive positive pressure ventilation (NIPPV) on mortality in patients with acute cardiogenic pulmonary oedema: a meta-analysisLancet20063671155116316616558
- WinckJAzevedoLFCosta-PereiraAAntonelliMWyattJCEfficacy and safety of non-invasive ventilation in the treatment of acute cardiogenic pulmonary edema: a systematic review and meta-analysisCrit Care200610R6916646987
- CollinsSPMielniczukLMWhittinghamHABoseleyMESchrammDRStorrowABThe use of noninvasive ventilation in emergency department patients with acute cardiogenic pulmonary edema: a systematic reviewAnn Emerg Med20064826026916934647
- WengCLZhaoYTLiuQHMeta-analysis: noninvasive ventilation in acute cardiogenic pulmonary edemaAnn Intern Med201015259060020439577
- VitalFMRSaconatoHLadeiraMTNon-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary edema (review)Cochrane Database of Systematic Reviews 20083 Art. No:CD005351
- GrayAGoodacreSNewbyDEMassonMSampsonFNichollJ3CPO TrialistsNoninvasive ventilation in acute cardiogenic pulmonary edemaN Engl J Med200835914215118614781
- MeduriGUCookTRTurnerRECohenMLeeperKVNoninvasive positive pressure ventilation in status asthmaticusChest19961107677748797425
- MedoffBDInvasive and noninvasive ventilation in patients with asthmaRespiratory care20085374074818501028
- FernandezMMVillagraABlanchLFernandezRNon-invasive ven- tilation in status asthmaticusIntensive Care Med20012748649211355116
- SorokskyAStavDShpirerIA pilot prospective, randomized, placebo-controlled trial of bilevel positive airway pressure in acute asthmatic attackChest20031231018102512684289
- GuptaDNathAAgarwalRBeheraDA prospective randomized controlled trial on the efficacy of noninvasive ventilation in severe acute asthmaRespir Care20105553654320420722
- LimWJAkramMRCarsonKVNon-invasive positive pressure ventilation for treatment of respiratory failure due to severe acute exacerbations of asthmaCochrane Database of Systematic Reviews 201212 Art. No: CD004360
- WenzelSSevere asthma in adultsAm J Respir Crit Care Med200517214916015849323
- LazarusSCEmergency treatment of asthmaN Engl J Med201036375576420818877
- HonrubiaTGarcía LópezFJFrancoNNoninvasive vs conventional mechanical ventilation for acute respiratory failure: a multicenter, randomized controlled trialChest20051283916392416354864
- JollietPAbajoBPasquinaPChevroletJCNon-invasive pressure support ventilation in severe community-acquired pneumoniaIntensive Care Med20012781282111430536
- ConfalonieriMPotenaACarboneGPortaRDTolleyEAUmberto MeduriGAcute respiratory failure in patients with severe community-acquired pneumonia. A prospective randomized evaluation of noninvasive ventilationAm J Respir Crit Care Med19991601585159110556125
- FerrerMEsquinasALeónMGonzálezGAlarconATorresANoninvasive ventilation in severe hypoxemic respiratory failure: a randomized clinical trialAm J Respir Crit Care Med20031681438144414500259
- FerrerMEsquinasAArancibiaFNoninvasive ventilation during persistent weaning failure. A randomized controlled trialAm J Respir Crit Care Med2003168707612689847
- JiangJSKaoSJWangSNEffect of early application of biphasic positive airway pressure on the outcome of extubation in ventilator weaningRespirology1999416116510382235
- NavaSGregorettiCFanfullaFNoninvasive ventilation to prevent respiratory failure after extubation in high-risk patientsCrit Care Med2005332465247016276167
- FerrerMValenciaMNicolasJMBernadichOBadiaJRTorresAEarly noninvasive ventilation averts extubation failure in patients at riskAm J Respir Crit Care Med200617316417016224108
- FerrerMSellarésJValenciaMNon-invasive ventilation after extubation in hypercapnic patients with chronic respiratory disorders: randomised controlled trialLancet20093741082108819682735
- BurnsKEAdhikariNKKeenanSPMeadeMUse of non-invasive ventilation to wean critically ill adults off invasive ventilation: meta-analysis and systemic reviewBMJ2009338b157419460803
- BurnsKEAMeadeMOPremjiAAdhikariNKJNoninvasive positive-pressure ventilation as a weaning strategy for intubated adults with respiratory failureCochrane Database of Systematic Reviews 2013Issue 12 Art. No: CD00412710.1002/14651858.CD004127.pub3
- GiraultCBubenheimMAbrougFVENISE Trial GroupNoninvasive ventilation and weaning in patients with chronic hypercapnic respiratory failure patients: a randomized multicenter trialAm J Respir Crit Care Med201118467267921680944
- VaschettoRTuruczEDellapiazzaFNoninvasive ventilation after early extubation in patients recovering from hypoxemic acute respiratory failure: a single-centre feasibility studyIntensive Care Med2012381599160622825283
- ZhuFLiuZLLongXEffect of noninvasive positive pressure ventilation on weaning success in patients receiving invasive mechanical ventilation: a meta-analysisChin Med J (Engl)201312671337134323557568
- SuCLChiangLLYangSHPreventive use of noninvasive ventilation after extubation: a prospective, multicenter randomized controlled trialRespir Care20125720421021762554
- OrnicoSRLoboSMSanchesHSNoninvasive ventilation immediately after extubation improves weaning outcome after acute respiratory failure: a randomized controlled trialCrit Care201317R3923497557
- KeenanSPPowersCMcCormackDGBlockGNoninvasive positive-pressure ventilation for postextubation respiratory distress: a randomized controlled trialJAMA20022873238324412076220
- EstebanAFrutos-VivarFFergusonNDNoninvasive positive-pressure ventilation for respiratory failure after extubationN Engl J Med20043502452246015190137
- KeenanSPSinuffTBurnsKCanadian Critical Care Trials Group/Canadian Critical Care Society Noninvasive Ventilation Guidelines GroupClinical practice guidelines for the use of noninvasive positive-pressure ventilation and noninvasive continuous positive airway pressure in the acute care settingCMAJ20111833E195E21421324867
- AgarwalRReddyCAggarwalANGuptaDIs there a role for noninvasive ventilation in acute respiratory distress syndrome? A meta-analysisRespir Med10061002235223816678394
- RanaSJenadHGayPCBuckCFHubmayrRDGajicOFailure of non-invasive ventilation in patients with acute lung injury: Observational cohort studyCrit Care200610R7916696863
- DelclauxCL’HerEAlbertiCTreatment of acute hypoxemic nonhypercapnic respiratory insufficiency with continuous positive airway pressure delivered by a face mask: a randomized controlled trialJAMA20002842352236011066186
- AntonelliMContiGEsquinasAA multiple-center survey on the use in clinical practice of noninvasive ventilation as a first-line intervention for acute respiratory distress syndromeCrit Care Med200735182517133177
- HilbertGGrusonDVargasFNoninvasive ventilation in immunocompromised patients with pulmonary infiltrates, fever, and acute respiratory failureN Engl J Med200134448148711172189
- AntonelliMContiGBufiMNoninvasive ventilation for treatment of acute respiratory failure in patients undergoing solid organ transplantation: a randomized trialJAMA200028323524110634340
- DepuydtPOBenoitDDVandewoudeKHDecruyenaereJMColardynFAOutcome in noninvasively and invasively ventilated hematologic patients with acute respiratory failureChest20041261299130615486396
- Belenguer-MuncharazAAlbert-RodrigoLFerrandiz-SellésACebrián-GraulleraGEvolución de 10 años de aplicación de la ventilación mecánica en la insuficiencia respiratoria aguda del paciente hematológico ingresado en la unidad de cuidados intensivosMed Intensiva20133745246023890541
- GristinaGRAntonelliMContiGGiViTI (Italian Group for the Evaluation of Interventions in Intensive Care Medicine)Noninvasive versus invasive ventilation for acute respiratory failure in patients with hematologic malignancies: a 5-year multicenter observational surveyCrit Care Med201139102232223921666446
- DepuydtPOBenoitDDRoosensCDOffnerFCNoensLADecruyenaereJMThe impact of the initial ventilatory strategy on survival inhematological patients with acute hypoxemic respiratory failureJ Crit Care201025303619682849
- BarbasCSVCoutoLPKawano-DouradoLBNoninvasive ventilation for acute respiratory failure in patients with hematologic malignancies: what an Italian 5-year multicenter survey tells usCrit Care Med201139102358235921926491
- Kingden-MillesDMüllerEBuhlRNasal-continuous positive airway pressure reduces pulmonary morbidity and length of hospital stay following thoracoabdominal aortic surgeryChest200512882182816100174
- AltmayEKaracaPYurtsevenNContinuous positive airway pressure does not improve lung function after cardiac surgeryCan J Anaesth20065391992516960270
- GaszynskiTTokarzAPiotrowskiDMachalaWBoussignac CPAP in the postoperative period in morbidly obese patientsObes Surg20071745245617608255
- AuriantIJallotAHervéPNoninvasive ventilation reduces mortality in acute respiratory failure following lung resectionAm J Respir Crit Care Med20011641231123511673215
- SquadroneVCohaMCerrutiEPiedmont Intensive Care Units Network (PICUN)Continuous positive airway pressure for treatment of postoperative hypoxemia. a randomized controlled trialJAMA200529358959515687314
- AzoulayEDemouleAJaberAPalliative noninvasive ventilation in patients with acute respiratory failureIntensive Care Med2011371250125721656292
- LevyMTaniosMANelsonDOutcomes of patients with do-not-intubate orders treated with noninvasive ventilationCrit Care Med2004322002200715483407
- NavaSFerrerMEsquinasAPalliative use of non-invasive ventilation in end-of-life patients with solid tumors: a randomised feasibility trialLancet Oncol20131421921723406914
- DevlinJWNavaSFongJJBahhadyIHillNHSurvey of sedation practices during noninvasive positive-pressure ventilation to treat acute respiratory failureCrit Care Med2007352298230217717491
- ChiumelloDCoppolaSFroioSGregorettiCConsonniDNoninvasive ventilation in chest trauma: systematic review and meta-analysisIntensive Care Med2013391171118023571872
- ShneersonJMSimondsKNoninvasive ventilation for chest wall and neuromuscular disordersEur Respir J20022048048712212984
- HillNGarpestadEBrennanJResponse [letter]Chest2008133131431518187764
- MurguSDPecsonJColtHBronchoscopy during noninvasive ventilation: indications and techniqueRespir Care201055559560020420731
- ContalOAdlerDBorelJCImpact of different backup respiratory rates on the efficacy of noninvasive positive pressure ventilation in obesity hypoventilation syndrome: a randomized trialChest20131431374622556317
- JanssensJPMetzgerMSforzaEImpact of volume targeting on efficacy of bi-level non-invasive ventilation and sleep in obesity-hypoventilationRespir Med200910316517218579368
- BakkerJPMarshallNSFlexible pressure delivery modification of continuous positive airway pressure for obstructive sleep apnea does not improve compliance with therapy: systematic review and meta-analysisChest20111391322133021193533
- CarrilloAFerrerMGonzalez-DiazGNoninvasive ventilation in acute hypercapnic respiratory failure caused by obesity hypoventilation syndrome and chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20121861279128523103736
- KasaiTUsuiYYoshiokaTJASV InvestigatorsEffect of flow-triggered adaptive servo-ventilation compared with continuous positive airway pressure in patients with chronic heart failure with coexisting obstructive sleep apnea and Cheyne-stokes RespirationCirc Heart Fail2010314014819933407
- CarlucciARichardJCWysockiMLepageEBrochardLSRLF Collaborative Group on Mechanical VentilationNoninvasive versus conventional mechanical ventilation. An epidemiologic surveyAm J Respir Crit Care Med200116387488011282759
- GarpestadEBrennanJHillNSNoninvasive ventilation for critical careChest200713271172017699147
- LelloucheFBrochardLAdvanced closed loops during mechanical ventilation (PAV, NAVA, ASV, SmartCare)Best Pract Res Clin Anaesthesiol200923819319449618
- Fernández-VivasMCaturla-SuchJGonzález de la RosaJAcosta-EscribanoJAlvarez-SánchezBCánovas-RoblesJNoninvasive pressure support versus proportional assist ventilation in acute respiratory failureIntensive Care Med2003291126113312802487
- GayPCHessDRHillNSNoninvasive proportional assist ventilation for acute respiratory insufficiency: comparison with pressure support ventilationAm J Respir Crit Care Med20011641606161111719297
- WysockiMRichardJCMeshakaPNoninvasive proportional assist ventilation compared with noninvasive pressure support ventilation in hypercapnic acute respiratory failureCrit Care Med20023032332911889302
- LeeJHRehderKJWillifordLCheifetzIMTurnerDAUse of high flow nasal cannula in critically ill infants, children, and adults: a critical review of the literatureIntensive Care Med20133924725723143331
- PiquilloudLTassauxDBialaisENeurally adjusted ventilatory assist (NAVA) improves patient-ventilator interaction during noninvasive ventilation delivered by face maskIntensive Care Med2012381624163122885649
- Gama de AbreuMBeldaFJNeurally adjusted ventilatory assist: letting the respiratory center take over control of ventilationIntensive Care Med2013391481148323793885
- BertrandPMFutierECosielYMeteckiSJaberSConstantinJMNeurally adjusted ventilatory assist vs pressure support ventilation for noninvasive ventilation during acute respiratory failureChest2013143303622661448
- Mireles-CabodevilaEChatburnRLWork of breathing in adaptive pressure control continuous mandatory ventilationRespir Care2009541467147219863830
- Briones ClaudettKHBriones ClaudettMChung Sang WongMNoninvasive mechanical ventilation with average volume assured pressure support (AVAPS) in patients with chronic obstructive pulmonary disease and hypercapnic encephalopathyBMC Pulm Med2013131223497021
- DellwegDKerlJHoehnEWenzelMKoehlerDRandomized controlled trial of noninvasive positive pressure ventilation (NPPV) versus servoventilation in patients with CPAP-induced central sleep apnea (complex sleep apnea)Sleep20133681163117123904676
- SharmaBKBakkerJPMcSharryDGDesaiASJavaheriSMalhotraAAdaptive servoventilation for treatment of sleep-disordered breathing in heart failure: a systematic review and meta-analysisChest201214251211122122722232
- FodilRLelloucheFManceboJComparison of patient-ventilator interfaces based on their computerized effective dead spaceIntensive Care Med20113725726221063677
- PravinkumarSEA face that matters in distress: interface selection for acute noninvasive ventilationCrit Care Med20093734434519112296
- NavalesiPFanfullaFFrigerioPGregorettiCNavaSPhysiologic evaluation of noninvasive mechanical ventilation delivered with three types of masks in patients with chronic hypercapnic respiratory failureCrit Care Med2000281785179010890620
- WillingSSan PedroMDriverHSMuntPFitzpatrickMFThe acute impact of continuous positive airway pressure on nasal resistance: a ran-domized controlled comparisonJ Appl Physiol20071021214121917158250
- GiraultCBrielABenichouJInterface strategy during noninvasive positive pressure ventilation for hypercapnic acute respiratory failureCrit Care Med20093712413119050635
- CrimiCNotoAPrinciPEsquinasANavaSA European survey of noninvasive ventilation practicesEur Respir J20103636236920075052
- KwokHMcCormackJCeceRHoutchensJHillNSControlled trial of oronasal versus nasal mask ventilation in the treatment of acute respiratory failureCrit Care Med20033146847312576953
- GerardJCrinerGTravalinaJBrennanKKreimerDEfficacy of a new full face mask for non-invasive positive pressure ventilationChest1994106110911157924481
- ChacurFHVilella FelipeLMFernandesCGLazzariniLCThe total face mask is more comfortable than the oronasal mask in noninvasive ventilation but is not associated with improved outcomeRespiration20118242643021846957
- LemyzeMMallatJNigeonORescue therapy by switching to total face mask after failure of face mask-delivered noninvasive ventilation in do-not-intubate patients in acute respiratory failureCrit Care Med20134148148823263582
- OzsancakASidhomSSLieschingTNHowardWHillNSEvaluation of the total face mask for noninvasive ventilation to treat acute respiratory failureChest20111391034104121330385
- CavaliereFContiGCostaRProiettiRSciutoAMasieriSNoise exposure during noninvasive ventilation with a helmet, a nasal mask and a facial maskIntensive Care Med2004301755176015185070
- NavalesiPCostaRCerianaPNon-invasive ventilation in chronic obstructive pulmonary disease patients: helmet versus facial maskIntensive Care Med200733748117039354
- VargasFThilleALyazidiACampoFRBrochardLHelmet with specific settings versus facemask for noninvasive ventilationCrit Care Med2009371921192819384209
- SchneiderEDualéCVailleJLComparison of tolerance of facemask vs mouthpiece for non-invasive ventilationAnaesthesia200661202316409337
- FraticelliATLelloucheFL’HerETailléSManceboJBrochardLPhysiological effects of different interfaces during noninvasive ventilation for acute respiratory failureCrit Care Med20093793994519237900
- CarteauxGLyazidiACordoba-IzquierdoAPatient-ventilator asynchrony during noninvasive ventilation: a bench and clinical studyChest2012142236737622406958
- NavaSAmbrosinoNBruschiCConfaleroniMRampollaCPhysiological effects of flow and pressure triggering during non- invasive mechanical ventilation in patientsThorax1997522492549093341
- BellaniGGuiseppeFSpagnolliECastagnaLPatronitiNPesentiAAn improved Boussignac device for the delivery of non-invasive CPAP: the SUPER-BoussignacIntensive Care Med2009351094109919169667
- American Association for Respiratory CareRestrepoRWalshBKHumidification during invasive and noninvasivemechanical ventilation; 2012Respir Care201257578278822546299
- OtoJImanakaHNishimuraMClinical factors affecting inspired gas humidification and oral dryness during noninvasive ventilationJ Crit Care201126535.e9535.e1521185145
- HessDRThe evidence for noninvasive positive-pressure ventilation in the care of patients in acute respiratory failure: a systematic review of the literatureRespir Care20044881082915222912
- LieschingTKwokHHillNSAcute applications of noninvasive positive pressure ventilationChest2003124669713
- LelloucheMMaggioreSMDeyeNEffect of the humidification device on the work of breathing during noninvasive ventilationIntensive Care Med2002281582158912415444
- JaberSChanquesGMateckiSComparison of the effects of heat and moisture exchangers and heat humidification on ventilation and gas exchange during non-invasive ventilationIntensive Care Med2002281590159412415445
- HubbleMWRichardsMEJarvisRMillikanTYoungDEffectiveness of prehospital continuous positive airway pressure in the management of acute pulmonary edemaPrehosp Emerg Care20061043043916997770
- DucrosLLogeartDVicautECPAP collaborative study groupCPAP for acute cardiogenic pulmonary oedema from out-of-hospital to cardiac intensive care unit: a randomised multicentre studyIntensive Care Med2011371501150921805159
- MasAAlonsoGPerezCSauraPAlcoverroJMGuiradoMNon-invasive mechanical ventilation for acute dyspnea in out-of-hospital emergency care [abstract]Intensive Care Med200228256S6911904653
- RoesslerMSSchmidDMichelsPEarly out-of-hospital non-invasive ventilation is superior to standard medical treatment in patients with acute respiratory failure: a pilot studyEmerg Med J201229540941421951764
- EstebanAFergusonNDMeadeMOVENTILA GroupEvolution of mechanical ventilation in response to clinical researchAm J Respir Crit Care Med200817717017717962636
- SinuffTCookDRandallJAllenCNoninvasive positive-pressure ventilation: a utilization review of use in a teaching hospitalCMAJ200016396997311068568
- HessDRNoninvasive ventilation for acute respiratory failureRespir Care20135895097223709194
- Soo HooGWSantiagoSWilliamsAJNasal mechanical ventilation for hypercapnic respiratory failure in chronic obstructive pulmonary disease: determinants of success and failureCrit Care Med199422125312618045145
- PoponickJMRenstonJPBennettRPEmermanCLUse of a ventilatory support system (BiPAP) for acute respiratory failure in the emergency departmentChest199911616617110424521
- SchettinoGAltobelliNKacmarekRNoninvasive positive-pressure ventilation in acute respiratory failure outside clinical trials: experience at the Massachusetts General HospitalCrit Care Med20083644144718091540
- ElliottMWThe interface: crucial for successful noninvasive ventilationEur Respir J2004237814738223
- Di MarcoFCentanniSBelloneAOptimization of ventilator setting by flow and pressure waveforms analysis during noninvasive ventilation for acute exacerbations of COPD: a multicentric randomized controlled trialCrit Care201115R28322115190
- VignauxLVargasFRoeselerJPatient-ventilator asynchrony during non-invasive ventilation for acute respiratory failure: a multicenter studyIntensive Care Med20093584084619183949
- HuangZChenYSYangZLLiuJYDexmedetomidine versus midazolam for the sedation of patients with non-invasive ventilation failureIntern Med2012512299230522975538
- ConstantinJMSchneiderECayot-ConstantinSRemifentanil-based sedation to treat noninvasive ventilation failure: a preliminary studyIntensive Care Med200733828717103141
- SenogluNOksuzHDoganZYildizHDemirkiranHEkerbicerHSedation during noninvasive mechanical ventilation with dexmedetomidine or midazolam: a randomized, double-blind, prospective studyCurr Ther Res Clin Exp20107114115324683260
- DuanJTangXHuangSJiaJGuoSProtocol-directed versus physician-directed weaning from noninvasive ventilation: the impact in chronic obstructive pulmonary disease patientsJ Trauma Acute Care Surg2012721271127522673254