
Abstract
Background
Acupuncture has been used as an adjuvant therapy for Chronic obstructive pulmonary disease (COPD). However, systematic reviews (SRs) and meta-analyses (MAs) have reported inconsistent results and unknown quality. This overview aimed to summarize the current SRs/MAs to provide evidence for the effectiveness and safety of acupuncture in the treatment of COPD.
Methods
SRs/MAs were searched via eight databases from their establishment to December 31, 2023. The methodological quality was assessed by A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2). The risk of bias was assessed using the Risk of Bias in Systematic Review (ROBIS) tool. The Preferred Reporting Items for Systematic Reviews and Meta-analyses for Acupuncture (PRISMA-A) to evaluate the reporting quality. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to determine the strength of evidence. In addition, we also conducted an analysis of the acupuncture points used in the primary RCTs.
Results
Twenty-two SRs/MAs were included in this overview. Based on the assessment using AMSTAR 2, nineteen SRs/MAs were “critically low”. Eight SRs/MAs had a low risk of bias. Based on PRISMA-A, the reporting completeness of eighteen SRs/MAs were more than 70%. As for GRADE assessment, only three outcome measures were of high quality. COPD patients can benefit from moxibustion, acupoint application, acupoint catgut embedding, manual acupuncture, and electroacupuncture, as indicated by effectiveness in measures including lung function, 6MWD, mMRC, CAT, and acute exacerbation. In addition, the efficacy of TENS needed to be further demonstrated. The commonly used acupuncture points in the RCTs include BL13, BL23, and EX-B1.
Conclusion
Evidence from SRs showed that acupuncture is beneficial to lung function, acute exacerbation, 6MWD, mMRC and CAT. For SGRQ and brog scale, acupuncture should be used selectively, but this finding should still be taken with caution.
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterized by chronic respiratory symptoms such as dyspnea, cough, and expectoration.Citation1 COPD is associated with significant socioeconomic implications, a substantial global prevalence, and high mortality rates. Older adults have a higher prevalence of COPD.Citation2 As the population ages worldwide, the incidence and mortality of COPD will likely increase substantially, and the COPD burden is projected to increase over the coming decades.Citation3,Citation4 It is projected that by the year 2060, COPD will contribute to over 5.4 million annual deaths.Citation3,Citation5 The etiology of COPD is complex and remains unclear. It is commonly associated with tobacco smoking, occupational exposure, air pollutants, and a history of lung infections.Citation6,Citation7 Studies have shown that patients with COPD are at high risk of developing cardiovascular disease, osteoporosis, and metabolic syndrome.Citation8,Citation9 Furthermore, COPD can negatively impact the mental health of patients with COPD.Citation10 Therefore, COPD is an important and urgent global public health issue that deserves widespread attention.Citation11
Currently, the main approach is to deal with symptoms of the airflow limitation through medication, oxygen treatment and rehabilitation therapy. However, current treatments are unable to achieve satisfactory therapeutic effects or prevent the progression of the disease. Drug treatment also cause side effects, including infection and immunosuppression. Consequently, it is imminent to discover safe and effective treatments for COPD.Citation12,Citation13 Hence, there is an urgent need to explore adjunctive treatment options for COPD. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 Report emphasizes the relevance of non-pharmacological treatment as a complementary component of the comprehensive management of COPD alongside pharmacological treatment.Citation14 Acupuncture, a non-pharmacological modality with a rich history dating back at least 2500 years in traditional Chinese medicine, has shown promise in effectively and safely treating various conditions, including COPD.Citation15–18 Notably, a substantial number of randomized controlled trials (RCTs) and systematic reviews (SRs) have evaluated the efficacy and safety of acupuncture in COPD.Citation19–24 However, the findings of these studies have been inconsistent.
SRs have progressively risen to the summit of what is considered high-quality evidence in research.Citation25 However, SRs are susceptible to bias and errors, and previous studies have revealed that not all SRs are truly systematic and their quality is highly variable.Citation26,Citation27 Therefore, it is necessary to compile evidence in an unbiased, systematic manner to assess the quality of evidence regarding COPD treatment. Recently, an overview was conducted to evaluate the role of acupuncture in the management of COPD.Citation28 However, the review did not include non-invasive acupuncture methods such as moxibustion and transcutaneous electrical acupoint stimulation.
In this case, we aimed at conducting an overview of the SRs on acupuncture for patients with COPD, to systematically evaluate and broadly summarize SRs that assess the effects and safety of acupuncture for COPD patients, also to provide recommendations for future reviews and trials, as well as support clinical practice.
Methods
This overview was registered on PROSPERO (registration number: CRD42023453584), and the study protocol was developed using the framework described by Smith et al.Citation29 This overview was performed following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Table S1).Citation30,Citation31
Search Strategy
We searched four English databases (PubMed, the Cochrane Library, Embase, and Web of Science) and four Chinese databases (CNKI, Wanfang Data, VIP, and CBM) from their inception to December 31, 2023. MeSH items or free words included: (Chronic obstructive lung disease OR Chronic obstructive pulmonary disease OR Chronic obstructive airway disease OR Chronic airflow obstruction) AND (systematic review OR Meta-analysis) AND (Acupuncture OR Acupuncture therapy OR Acupuncture points OR Electroacupuncture OR Transcutaneous electrical stimulation). The search strategy of EMBASE is shown in Table S2 and adapted according to the different characteristics of each database.
Inclusion Criteria
Our inclusion criteria were as follows: (1) Study design: the study must be a systematic review/meta-analysis of RCTs. (2) Participants: patients who were diagnosed with COPD based on the GOLD 2023 report, without restrictions on sex, age, and race.Citation14 (3) Treatment group intervention: acupuncture as the main treatment or main adjuvant treatment, including manual acupuncture, moxibustion, electroacupuncture, warm acupuncture, abdominal acupuncture, auricular needling, transcutaneous electrical acupoint stimulation, acupoint catgut embedding, and acupoint application. (4) Control group intervention: conventional treatment, placebo, and waiting treatment. (5) Outcome measures: covering various parameters, including lung function, exercise capacity, dyspnea, and health-related quality of life.
Exclusion Criteria
SRs were excluded if they met any of the following criteria: (1) solely conducted network meta-analysis. (2) participants were diagnosed with COPD alongside other diseases. (3) acupuncture was a non-major intervention in the treatment group. (4) the control group included acupuncture Methods and traditional Chinese medicine. (5) comprised SR protocols, duplicate publications, commentaries, or meeting abstracts.
Study Screening
All the authors were trained to conduct the review professionally. Initially, all the search results were imported into NoteExpress V.3.5.0, and duplicate publications were removed. Two authors (QZ and LL) independently screened all studies by reading titles, abstracts, and keywords. Eligible studies then underwent full-text screening. During the full-text review, any excluded studies were documented with the reasons for their exclusion. In the event of any disagreements regarding the eligibility of a study, a Discussion was initiated to resolve the matter. If a consensus could not be reached, a third investigator (YC) was involved.
Data Extraction
A data extraction form was collaboratively developed by the authors. Data extraction was performed independently by two authors (QZ and LL), while the other two authors (DHC and ZYZ) checked the accuracy and format of the data. The following information was extracted: basic information (first author, year of publication, country), methods (the number of included RCTs and participants, diagnostic criteria, intervention and control treatment, quality assessment tools), and results (safety and main conclusions). If several SRs involved the same intervention and outcome, chose the effect size of the SRs with the largest number of RCTs to reported.
Methodological Quality Evaluation
The methodological quality of the included SRs was evaluated using the A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2),Citation32 a critical appraisal tool for assessing the quality of SRs that include randomized or non-randomized studies. AMSTAR 2 contains 16 items, including 7 critical items and 9 non-critical items. The tool classifies the quality of SRs into four levels: high (0/1 shortcoming in non-critical item), moderate (≥ 1 shortcoming in non-critical items), low (1 critical flaw, with or without a shortcoming in non-critical items), and extremely low (≥ 1 critical flaw, with or without shortcomings in non-critical items). Two authors (QZ and ZYZ) independently assessed the methodological quality of the included reviews. Any conflicts were resolved through discussion or by seeking guidance from the third author (YC).
Risk of Bias Assessment
Two authors (QZ and SYG) independently assessed the included SRs for bias using the Risk of Bias in Systematic Reviews (ROBIS) tool.Citation33 Any disparities in the assessments made by these two authors that remained unresolved were further evaluated by the third author (YC). The ROBIS tool was used to assess the risk of bias in the included SRs across four domains, including study eligibility criteria, identification and selection of studies, data collection and study appraisal, and synthesis and findings. Each domain was rated as “low”, “high”, or “unclear”.
Assessment of Reporting Quality
Two authors (QZ and LL) independently used the Preferred Reporting Items for Systematic Reviews and Meta-analyses for Acupuncture (PRISMA-A) checklist to evaluate the reporting quality of each included SR (Table S4).Citation34 The PRISMA-A, published in 2019, is an extension version of PRISMA designed for the interpretation of SRs of acupuncture. It consists of 27 items, with each item being judged as “yes”, “no”, or “partial yes”. Any discrepancies in the assessment made by QZ and LL were resolved by consensus or adjudication by the third author (YC).
Evidence Quality Evaluation
The quality of evidence for the results of the included SRs was independently assessed by two authors (QZ and DHC) using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system.Citation35 The pieces of evidence were rated as “high”, “moderate”, “low”, and “very low” quality based on five key aspects: limitation, inconsistency, indirectness, imprecision, and publication bias. Any disagreement in the assessment made by the authors was resolved through the guidance of the third author (YC).
Data Synthesis
This study provides a comprehensive analysis regarding the use of acupuncture in the treatment of COPD. The results of the meta-analysis and other data from the included SRs were synthesized descriptively. If a SR did not separate the different types of acupuncture therapies, we will use Review Manager 5.4 to re-quantified relevant outcome indicators from the RCTs in the SR. Furthermore, because this study involves acupuncture therapy, we also analyzed the selected acupoints in each RCT. The data were summarized and presented as percentage and frequency for each item of AMSTAR 2, ROBIS, PRISMA-A and GRADE.
Results
Search Results
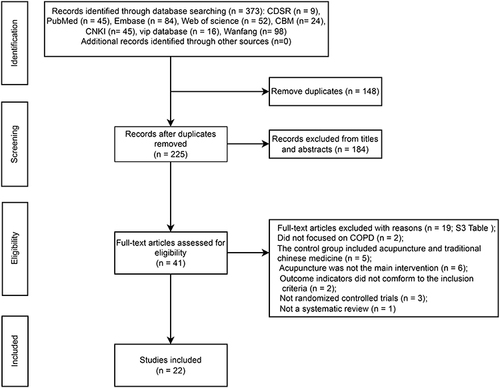
The initial search strategy produced 373 articles. After importing these articles into Note Express 3.5, 148 duplicates were identified and subsequently removed. Next, 184 articles were excluded after a thorough review of their titles and abstracts. After reading the full text, 19 articles were excluded and 22 articles were finally included in this overview. The process of study selection is shown in . The list of excluded studies and reasons is provided in Table S3.
Figure 1 Flow diagram of study selection. The inclusion and exclusion of systematic reviews studying acupuncture for chronic obstructive pulmonary disease.
Characteristics of the Included Systematic Reviews
All studies included in the 22 SRs were RCTs.Citation22,Citation36–56 The eligible SRs were all published between 2014 and 2023, with 9 of them published in English and 13 in Chinese. The included SRs searched between 6 to 9 databases and included between 8 RCTs (with 498 participants) to 42 RCTs (with 4192 participants). The intervention groups included acupuncture alone and acupuncture combined with conventional treatment. The acupuncture interventions included various forms of acupuncture, including manual acupuncture, electroacupuncture, acupoint catgut embedding, moxibustion, acupoint application, and transcutaneous electrical nerve stimulation. The control groups were mainly conventional treatment, sham acupuncture. The outcome measures mainly referred to the following five categories: lung function, dyspnea, quality of life, exercise capacity, and frequency of acute exacerbation. Only 10 SRs reported the stage of COPD, with 9 SRs involving stable patients and 1 SR involving exacerbated patients. A total of 19 SRs used the Cochrane risk of bias tool to assess the methodological quality of the RCTs they included; 1 SR used the modified Jadad scale; and 1 SR did not report the assessment tool that they used. Furthermore, 18 studies assessed the safety of acupuncture therapy, with 18 finding it safe and 4 having inconclusive Results. Only 7 SRs reported funding sources. The characteristics of included SRs are presented in .
Table 1 Characteristics of Included Systematic Reviews on Acupuncture for COPD
Methodological Quality of Included SRs
As assessed by AMSTAR 2, none of the included SRs was rated as high quality. Notably, 3 SRs (13.64%) were considered to be of low quality, while 19 SRs (86.36%) were considered to be of critically low quality. All 22 SRs reported their review questions and inclusion criteria following the patient/problem, intervention, comparison, and outcome (PICO) principle. Five SRs (22.73%) registered their protocol before the study began. In terms of the eligibility criteria, all 22 SRs reported the inclusion of RCTs without providing a specific explanation but did employ systematic search strategies. Nineteen SRs (86.36%) conducted double screening and extraction. None of the SRs provided a complete list of excluded references and reasons for their exclusion. All 22 SRs followed the PICO principle in describing the characteristics of the included RCTs. Among them, 7 SRs (31.82%) provided detailed information about the population, intervention and control measures, study site, and follow-up period. All SRs used appropriate tools to assess the risk of bias in the included studies, including the Cochrane risk of bias tool or the Jadad scale. Seventeen SRs (77.27%) investigated the possibility of publication bias, and 4 SRs (18.18%) stated no conflict of interest. All SRs had shortcomings, including incomplete literature searches and insufficiently detailed descriptions of the RCTs. The results of the AMSTAR-2 assessment are shown in .
Table 2 Quality of the Included Reviews as Rated on the AMSTAR 2 Scale
Risk of Bias of Included SRs
The results of the risk of bias assessment are presented in . In Phase 2 of Domain-1, which evaluated study eligibility criteria, 18 SRs (81.82%) were considered to be at low risk of bias. Domain-2 evaluated the identification and selection of studies, and only 6 SRs (27.27%) were considered to have a low risk of bias. Domain-3 covered data collection and study appraisal, and 13 SRs (59.09%) were considered to have a low risk of bias, while 8 SRs (36.36%) had an unclear risk of bias. Only 6 SRs (27.27%) had a low risk of bias in Domain-4, which evaluated data synthesis and findings. The overall risk of bias in the SRs was evaluated in Phase 3, where 8 SRs (36.36%) were regarded as having an overall low risk of bias.
Table 3 Risk of Bias of the Included Systematic Reviews Assessed by Risk of Bias in Systematic Reviews
Reporting Quality of Included SRs
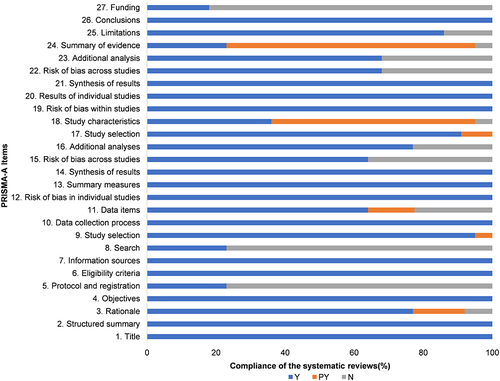
The reporting quality of the included SRs is displayed in , and a detailed assessment is presented in Table S4. Of the 27 items assessed, 18 items were reported with eligibility of at least 70%, suggesting that the reports were mostly complete. Furthermore, the reporting completeness of 18 SRs (81.82%) was greater than 70%. However, the included SRs have 5 substantial deficiencies: Item 5 (Methods: protocol and registration), Item 8 (methods: search), Item 18 (Results: study characteristics), Item 24 (discussion: summary of evidence), and Item 27 (funding). Only 5 out of the 22 SRs (22.73%) reported registration of their protocol. Moreover, 5 SRs (22.73%) provided a full electronic search strategy for at least one commonly used database. Also, 14 SRs (63.64%) did not consider their relevance to key groups or provide sufficient detail about the characteristics of the RCTs they included, and only 4 SRs (18.18%) described their sources of funding and other support.
Figure 2 Graphical presentation of PRISMA-A.
Confidence in Study Outcomes
We summarized the confidence in the findings of the 22 SRs in Table S5. Our assessment tool found confidence in study outcomes to be “high” in 3 studies (2.50%), “moderate” in 20 studies (16.67%), “low” in 57 studies (47.50%), and “very low” in 40 studies (33.33%). Publication bias (76.67%) was the most common of the downgrading factors in the included SRs, followed by imprecision (66.67%), inconsistency (44.17%), risk of bias (27.50%), and indirectness (0.00%).
Lung Function
All 22 SRs used lung function to assess the effect of acupuncture in COPD patients. A total of 9Citation22,Citation42,Citation45,Citation46,Citation50–54 SRs assessed FEV1, of which acupoint application + CT [MD= 0.12, 95% (0.04, 0.20), P=0.002], acupoint autohemotherapy [MD= 0.32, 95% (0.26, 0.39), P<0.00001], TENS + CT [MD= 0.13, 95% (0.11, 0.14), P<0.00001], acupoint catgut embedding [MD= 0.04, 95% (0.00, 0.09), P=0.04], moxibustion [MD= 0.54, 95% (0.45, 0.63), P<0.05] were able to improve FEV1. However, compared with placebo therapy, there was no statistically significant difference in the clinical efficacy of TENS [MD=0.04, 95% (−0.05, 0.13), P>0.05], manual acupuncture [MD=0.00, 95% (−0.15, 0.15), P>0.05], ear acupuncture [MD=0.05, 95% (−0.05, 0.14), P=0.33], and acupoint application [MD=0.01, 95% (−0.19, 0.21), P>0.05], as shown in .
Table 4 Result of Lung Function
14Citation36–45,Citation49–51,Citation55 SRs systematically analyzed FEV1%pre, CarlesCitation43 found that electroacupuncture [MD=8.85, 95% ((2.11, 15, 59), P=0.01] was more effective than manual acupuncture [MD=3.20, 95% (0.56, 5.83), P=0.02] and manual acupuncture + ear acupuncture [MD=5.40, 95% (2.55, 8.25), P<0.05] were able to achieve more positive impacts. In addition, moxibustion [MD=4.00, 95% (2.63, 5.37), P<0.00001] and acupoint application [MD=3.04, 95% (1.76, 4.33), P<0.00001] could achieve the desired results. In contrast, TENS and warm needling did not improve the outcome indicators significantly, as shown in and Figure S1.
17Citation22,Citation36–41,Citation43–47,Citation49,Citation50,Citation52,Citation53,Citation56 SRs assessed FEV1/FVC, CarlesCitation43 found that electroacupuncture [MD=10.40, 95% (4.79, 16.01), P=0.0003], manual acupuncture [MD=4.28, 95% (2.44,6.12), P<0.00001], manual acupuncture + ear acupuncture [MD=4.97, 95% (2.00,7.94), P<0.05] all achieved better results, with electroacupuncture being more effective. Moxibustion [MD=3.56, 95% (1.69, 5.43), P=0.0002] improved FEV1/FVC compared with conventional treatment, but the effect of warm needling and acupoint catgut embedding on this outcome indicator were not statistically different, as shown in and Figure S2.
4Citation22,Citation37,Citation42,Citation54 SRs assessed FVC, only acupoint autohemotherapy [SMD=0.34, 95% (0.11, 0.57), P=0.004] can effectively improve FVC. However, the effect of manual acupuncture [MD=0.00, 95% (−0.27, 0.27), P>0.05], TENS [MD=0.12, 95% (−0.16, 0.39), P=0.40], and electroacupuncture [MD=2.01, 95% (−5.25, 9.26), P=0.59] on the FVC seems to be not statistically significant, as shown in and Figure S3.
Exercise Capacity
FifteenCitation22,Citation36,Citation37,Citation39–46,Citation51–54 SRs assessed exercise capacity, with all trials using the 6-minute walking distance (6MWD). CarlesCitation43 found that electroacupuncture [MD=68.82, 95% (10.81, 126.83), P=0.02] was superior to warm needling [MD=51.44, 95% (14.00, 88.88), P=0.007], manual acupuncture + ear acupuncture [MD =5.40, 95% (2.55, 8.25), P<0.05]. Moxibustion [MD=35.00, 95% (18.02, 51.99), P<0.0001], acupoint application [MD=16.77, 95% (7.15, 26.39), P=0.0006], acupoint catgut embedding [MD=28.16 95% (17.31, 39.00), P<0.00001], TENS + CT [MD=14.68, 95% (6.92, 22.44), P=0.0002], and acupoint autohemotherapy [MD=29.82, 95% (19.31, 40.33), P<0.00001] all significantly improved the 6MWD in COPD patients. However, compared with placebo therapy, the effect of TENS alone on this outcome indicator was not statistically different, as shown in and Figure S4.
Table 5 Result of Exercise Capacity
Quality of Life
Two scales were used to assess the improvement in the quality of life of patients: St. George’s Respiratory Questionnaire (SGRQ) and COPD Assessment Test (CAT). ElevenCitation37,Citation39,Citation42,Citation44,Citation47–50,Citation52,Citation55,Citation56 SRs evaluated interventions using SGRQ as an outcome indicator. Acupoint application [MD=−6.77, 95% (−9.81, −3.72), P<0.0001] and manual acupuncture [MD=−10.09, 95% (−18.43, −3.37), P<0.05] were able to reduce the SGRQ score, but the effect of electroacupuncture and TENS on reducing SGRQ were not statistically significant, as shown in .
Table 6 Result of Quality of Life
CAT was observed in tenCitation38,Citation40,Citation44–46,Citation49,Citation51,Citation54–56 SRs. Compared with conventional treatment, moxibustion [MD=−3.40, 95% (−5.82, −0.98), P=0.006], acupoint catgut embedding [MD=−2.39, 95% (−3.65, −1.13), P=0.0002], acupoint application [MD=−3.33, 95% (−3.87, −2.79), P<0.00001], acupoint autohemotherapy [SMD=3.22, 95% (2.72, 3.73), P<0.00001], warm needling [MD=−4.77, 95% (−6.53, −3.01), P<0.00001] and TENS [MD=−4.25, 95% (−5.24, −3.27), P<0.00001] all significantly reduced CAT. Furthermore, XieCitation38 found that manual acupuncture + ear acupressure [MD=−4.30, 95% (−6.32, −2.28), P<0.05] and manual acupuncture + acupoint application [MD=−4.20, 95% (−6.28, −2.21), P<0.05] could also reduce CAT of patients with COPD, as shown in .
Dyspnea
NineCitation36,Citation38,Citation40–43,Citation45,Citation51,Citation52 SRs assessed Dyspnea. The modified Medical Research Council (mMRC) scale was used in eight 34, 36, 38–41, 43, 50 SRs. In terms of mMRC, moxibustion [MD=−0.52, 95% (−0.88, −0.15), P=0.006], acupoint catgut embedding [MD=−0.15, 95% (−0.29, −0.02), P=0.03], acupoint application [SMD=−1.14, 95% (−1.53, - 0.75), P<0.0001], manual acupuncture + acupoint application [MD=−0.60, 95% (−0.99, −0.20), P<0.05], and manual acupuncture + ear acupressure [MD=−0.90, 95% (−1.24, −0.56), P<0.05] were able to outperform conventional treatment and placebo therapy, but the effect of manual acupuncture on mMRC was not statistically different, as shown in .
Table 7 Result of Dyspnea
The Borg scale was observed in 3Citation42,Citation43,Citation51 SRs Compared with conventional treatment, both TENS [MD=−0.46, 95% (−0.86, −0.06), P=0.03] and acupoint application [MD=−0.34, 95% (−0.38, −0.30), P<0.05] reduced the Borg scale in patients with COPD. However, the effect of manual acupuncture on the Borg scale scores is not significant, as shown in .
Frequency of Acute Exacerbation
EightCitation36,Citation40,Citation41,Citation46,Citation48,Citation50,Citation53,Citation55 SRs evaluated the frequency of acute exacerbation. Compared with conventional treatment, moxibustion [MD=−0.31, 95% (−0.49, −0.14), P=0.0005], acupoint catgut embedding [MD=−0.54, 95% (−0.91, −0.17), P=0.004] and acupoint application [MD=−0.66, 95% (−0.76, −0.57), P<0.00001] were able to reduced acute exacerbation. In contrast, compared with placebo treatment, acupoint application did not reduce the outcome indicators significantly, as shown in .
Table 8 Result of Acute Exacerbation
Safety
SixteenCitation22,Citation36,Citation38,Citation40–46,Citation48,Citation49,Citation51–53,Citation55 SRs summarized the adverse events reported in various clinical trials. Among the SRs that reported specific cases, only mild adverse events were identified, including hematomas, dizziness, and needle-site pain. Notably, no serious adverse events were associated with acupuncture. Other SRs either did not mention adverse events nor reported any Safety information related to acupuncture.
Acupoint Analysis
We have computed all the acupoints used in the RCTs and selected the top acupoints in the primary studies, as shown in . Through analyzing acupuncture points of all acupuncture-related therapies, we discovered that the top 5 acupuncture points with the highest usage frequency are BL13 (Feishu), BL23 (Shenshu), EX-B1 (Dingchuan), ST36 (Zusanli), and BL20 (Pishu).
Table 9 Types of Acupoints Used for COPD
Discussion
This overview integrates and summarizes existing SRs that have investigated the use of acupuncture as an adjunctive treatment for COPD. The primary goal of this study was to evaluate the efficacy and safety of acupuncture in COPD. Moreover, we aimed to assess the methodological quality, risk of bias, and the overall quality of evidence of different interventions in the included SRs to guide clinical practice and direct future research.
Main Findings
Although the included SRs have suggested that acupuncture could be beneficial in managing COPD, confidence in these conclusions is weak due to the limitations of the RCTs included in the SRs. In addition, our assessments using the AMSTAR 2, ROBIS, and PRISMA-A revealed that each SR had notable deficiencies.
Studies on acupuncture as an adjunctive treatment for COPD mainly focused on stable patients. In this overview, out of the 11 SRs that reported the stage of COPD, 10 focused on stable patients, and 1 focused on exacerbated patients. For lung function, acupoint application, acupoint autohemotherapy, moxibustion, manual acupuncture, and electroacupuncture could significantly improve the lung function of COPD patients. In terms of exercise capacity and quality of life, moxibustion, acupoint catgut embedding, acupoint autohemotherapy, acupoint application, warm needling could significantly improve 6MWD and CAT compared with conventional treatment. As for reducing SGRQ scores, the effect of electroacupuncture, manual acupuncture, TENS on this outcome indicator was not statistically different. For the outcome indicators of dyspnea and moxibustion, acupoint catgut embedding, and acupoint application could also reduce the mMRC score and acute exacerbation of COPD patients. However, compared with sham therapy, the effect of TENS, electroacupuncture, and manual acupuncture on this outcome indicator was not statistically significant.
In the RCTs evaluated in this study, BL13 (Feishu), BL23 (Shenshu), EX-B1 (Dingchuan) and ST36 were the most commonly used acupoints. ST36 is a commonly used acupoint for various respiratory diseases, including COPD. The potential therapeutic mechanisms of ST36 may be closely related to anti-inflammatory and anti-oxidation effects.Citation57 Zou et al conducted a study revealing that electroacupuncture at ST36 and BL13 acupoints significantly reduced inflammatory response in rats.Citation58 Furthermore, a research study observed acupuncture at EX-B1 and BL23 appeared to protect lung function and reduce the COPD-induced inflammatory response.Citation59
However, interpretation of these findings needs to be approached with caution, given the potential risk of bias in the evidence. Notably, these SRs did not dismiss acupuncture as a viable treatment option. Instead, they recommended that clinicians consider acupuncture as a relatively effective and safe treatment option for COPD.
Acupuncture could be regarded as a safe adjunctive therapy for patients with COPD, as no severe adverse events were reported in the included SRs. Instead, the observed adverse events were generally mild and transient, such as spot-bleeding, needle-site pain, fatigue, and bruising. These effects can be effectively avoided by a qualified acupuncturist.
The methodological quality of the SRs, as assessed using AMSTAR 2, was generally low, mainly due to the lack of a registered protocol, a lack of an exclusion article list, and incomplete retrieval. However, the quality appraisal tools were properly selected. Evaluation using the ROBIS tool showed that the main sources of risk of bias in the included SRs stemmed from a lack of additional search sources, inadequate search terms, and unstable results. In the evaluation using PRISMA-A, failure to publish a protocol and registration, lack of literature search strategy, and incomplete Disclosures of sources of funding were associated with the limitations of the SRs. The assessment based on the GRADE approach showed that 80.83% of the outcomes had low- or very low-quality evidence. The most common reasons for downgrading included publication bias and imprecision.
Comparison with Previous Studies
In a previous overviewCitation28 closely related to this topic, acupuncture was investigated as either a primary or adjuvant treatment for COPD, the findings were similar to ours. This earlier overview identified nine SRs on acupuncture and demonstrated the therapeutic effects of acupuncture on 6MWD, SGRQ, FEV1%, and FEV1/FVC.
Our review, on the other hand, identified the largest number of SRs (22 SRs) of RCTs focusing on all acupuncture-related therapies for COPD. This comprehensive approach augments the clinical evidence, further supporting the use of acupuncture for managing COPD. Unlike the previous overview, we included SRs on invasive acupuncture (eg, manual acupuncture, acupoint injection, auricular acupuncture, and electro-acupuncture) and non-invasive acupuncture (eg, acupoint injection, moxibustion, acupoint application, and transcutaneous electrical acupoint stimulation). In addition, strict appraisal tools (AMASTAR 2, GRADE, PRISMA-A, and ROBIS) were used to assess the methodological quality, evidence quality, and risk of bias across all the included SRs. Moreover, although a few SRs indicated no difference between acupuncture plus conventional treatment and conventional treatment alone, we found that the superior effects of acupuncture in managing COPD became apparent after including newly published RCTsCitation45,Citation56 Therefore, acupuncture could be a treatment option for COPD.Citation24
Implications for Practice
This is a summary of evidence derived from SRs of RCTs on the efficacy and safety of acupuncture as an adjunctive treatment for COPD. This review demonstrated that acupuncture is an effective adjunctive treatment option for patients with COPD and should be considered in clinical practice. In addition, acupuncture is a traditional Chinese medical therapy, and the selection of acupoints for COPD patients should be based on individual diagnosis. Therefore, while standardizing acupoints, it is also important to pay careful to individualized treatment, so as to evaluate its clinical efficacy more accurately.
Implications for Future Research
Considering the identified limitations, future research in this area needs to adopt the following conditions: (1) Clinical studies should be recommended on conditions commonly used acupuncture in clinic, but lacking high-quality or well-reported evidence, like COPD-related lung function, dyspnea and exercise capacity. So RCTs should comply with the Consolidated Standards of Reporting Trials (CONSORT) guidelines and the Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA) to enhance the methodological quality, and no more low-quality, insufficient clinical studies. (2) Increasing the sample size and improving the quality of acupuncture-based RCTs are required to demonstrate its effectiveness and to determine which type (eg, manual acupuncture, moxibustion, auricular acupuncture, and electroacupuncture) and doses are more beneficial to patients. (3) Clinical studies should focus on implementing blinding, despite blinding is challenging in trials of non-drug treatments. Meanwhile, researchers should also pay attention to the potential effects of placebo acupuncture and use it sparingly. (4) Future SRs must adhere to the PRISMA statement and must pay attention to protocol and registration, comprehensive literature search, detailed information on excluded literature, and the assessment of the impact of bias risk—often overlooked aspects in SRs.
Strengths and Weaknesses
This is the first umbrella review to assess the effectiveness and safety of multiple different acupuncture therapies for COPD. This study provided a comprehensive overview of the use of acupuncture in COPD. The included studies SRs of RCTs. Such studies have the highest quality evidence. Our study used the AMSTAR tool, PRISMA-A, and the GRADE system to examine the methodological quality, risk of bias, and the quality of evidence. This will contribute to a more authentic perception of the effectiveness and value of acupuncture in the treatment of COPD. However, this overview has several limitations. First, the low quality of the primary RCTs directly limits the robustness of the overall assessment. Therefore, the reported results need to be interpreted with caution. Second, the AMSTAR 2, ROBIS, PRISMA-A, and GRADE tools are ultimately subjective. Although our assessment underwent analysis and review by independent researchers, the conclusions of the assessment may be influenced by different researchers’ subconscious bias. Finally, this study did not compare the efficacy of different acupuncture-related therapies. Therefore, we hope to remedy this limitation by utilizing the Network meta-analysis tool in subsequent studies.
Conclusion
Existing evidence indicates that acupuncture can be considered a useful adjunctive therapy for COPD, capable of reducing the frequency of acute exacerbation, mMRC, and CAT, enhance the lung function and exercise capacity. For SGRQ and brog scale, acupuncture should be used selectively. The appropriate use of acupuncture for managing COPD appears to be safe, with no serious adverse events reported. It is recommended that future trials adhere to CONSORT and STRICTA criteria to improve the quality of evidence.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
The authors really appreciate the help of people from Chengdu University of Traditional Chinese Medicine.
Additional information
Funding
References
- Celli B, Fabbri L, Criner G, et al. Definition and nomenclature of chronic obstructive pulmonary disease: time for its revision. Am J Respir Crit Care Med. 2022;206(11):1317–1325. doi:10.1164/rccm.202204-0671PP
- Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: results from the Global Burden of Disease Study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
- Soriano JB, Kendrick PJ, Paulson KR, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/s2213-2600(20)30105-3
- Zhai M, Jiang Q, Liu S, et al. DALY trend and predictive analysis of COPD in China and its provinces: findings from the global burden of disease study. Front Public Health. 2022;10:1046773. doi:10.3389/fpubh.2022.1046773
- World Health Organization. Projections of mortality and causes of death, 2016 and 2060. Available from: https://colinmathers.com/2022/05/10/projections-of-global-deaths-from-2016-to-2060/. Accessed July 3, 2024.
- Eisner MD, Anthonisen N, Coultas D, et al. An official American Thoracic Society public policy statement: novel risk factors and the global burden of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2010;182(5):693–718. doi:10.1164/rccm.200811-1757ST
- Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-smokers. Lancet. 2009;374(9691):733–743. doi:10.1016/s0140-6736(09)61303-9
- Fabbri LM, Luppi F, Beghé B, Rabe KF. Complex chronic comorbidities of COPD. Eur Respir J. 2008;31(1):204–212. doi:10.1183/09031936.00114307
- He Y, Liu S, Zhang Z, et al. Imbalance of endogenous hydrogen sulfide and homocysteine in chronic obstructive pulmonary disease combined with cardiovascular disease. Front Phar. 2017;8:624. doi:10.3389/fphar.2017.00624
- Hanania NA, Müllerova H, Locantore NW, et al. Determinants of depression in the ECLIPSE chronic obstructive pulmonary disease cohort. Am J Respir Crit Care Med. 2011;183(5):604–611. doi:10.1164/rccm.201003-0472OC
- Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/s0140-6736(22)00470-6
- Labaki WW, Rosenberg SR. Chronic obstructive pulmonary disease. Ann Intern Med. 2020;173(3):Itc17–itc32. doi:10.7326/aitc202008040
- Wang C, Zhou J, Wang J, et al. Progress in the mechanism and targeted drug therapy for COPD. Signal Transduct Target Ther. 2020;5(1):248. doi:10.1038/s41392-020-00345-x
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for prevention, diagnosis and management of COPD: 2023 report. Available from: https://goldcopd.org/2023-gold-report-2/. Accessed July 3, 2024.
- von Trott P, Oei SL, Ramsenthaler C. Acupuncture for breathlessness in advanced diseases: a systematic review and meta-analysis. J Pain Symptom Manage. 2020;59(2):327–38.e3. doi:10.1016/j.jpainsymman.2019.09.007
- Zhao L, Chen J, Li Y, et al. The Long-term Effect of Acupuncture for Migraine Prophylaxis: a Randomized Clinical Trial. JAMA Intern Med. 2017;177(4):508–515. doi:10.1001/jamainternmed.2016.9378
- Zhao L, Li D, Zheng H, et al. Acupuncture as adjunctive therapy for chronic stable angina: a randomized clinical trial. JAMA Intern Med. 2019;179(10):1388–1397. doi:10.1001/jamainternmed.2019.2407
- Suzuki M, Namura K, Ohno Y, et al. Combined standard medication and acupuncture for COPD: a case series. Acupunct Med. 2012;30(2):96–102. doi:10.1136/acupmed-2011-010112
- Levy I, Elimeleh Y, Gavrieli S, et al. Treatment of acute exacerbations of chronic obstructive pulmonary disease with acupuncture during hospitalization: a three-arm double-blinded randomized sham-controlled trial. Acupunct Med. 2022;40(6):505–515. doi:10.1177/09645284221086293
- Öncü E, Zincir H. The effect of transcutaneous electrical nerve stimulation in patients with acute exacerbation of chronic obstructive pulmonary disease: randomised controlled trial. J Clin Nurs. 2017;26(13–14):1834–1844. doi:10.1111/jocn.13450
- Suzuki M, Namura K, Ohno Y, et al. The effect of acupuncture in the treatment of chronic obstructive pulmonary disease. J Altern Complement Med. 2008;14(9):1097–1105. doi:10.1089/acm.2007.0786
- Fernández-Jané C, Vilaró J, Fei Y, et al. Acupuncture techniques for COPD: a systematic review. BMC Complement Med Ther. 2020;20(1):138. doi:10.1186/s12906-020-02899-3
- Liu Q, Duan H, Lian A, Zhuang M, Zhao X, Liu X. Rehabilitation effects of acupuncture on the diaphragm dysfunction in chronic obstructive pulmonary disease: a systematic review. Int J Chron Obstruct Pulmon Dis. 2021;16:2023–2037. doi:10.2147/COPD.S313439
- Tsai CL, Lan CC, Wu CW, et al. Acupuncture point stimulation treatments combined with conventional treatment in chronic obstructive pulmonary disease: a systematic review and network meta-analysis. Front Med Lausanne. 2021;8:586900. doi:10.3389/fmed.2021.586900
- Muka T, Glisic M, Milic J, et al. A 24-step guide on how to design, conduct, and successfully publish a systematic review and meta-analysis in medical research. Eur J Epidemiol. 2020;35(1):49–60. doi:10.1007/s10654-019-00576-5
- Conway A, Inglis SC, Chang AM, Horton-Breshears M, Cleland JG, Clark RA. Not all systematic reviews are systematic: a meta-review of the quality of systematic reviews for non-invasive remote monitoring in heart failure. J Telemed Telecare. 2013;19(6):326–337. doi:10.1177/1357633x13503427
- Gurevitch J, Koricheva J, Nakagawa S, Stewart G. Meta-analysis and the science of research synthesis. Nature. 2018;555(7695):175–182. doi:10.1038/nature25753
- Chun L, Li X, Feng Z, Xie Y, Li J. Role of acupuncture in the treatment of COPD: an overview of systematic reviews. Int J Gen Med. 2021;14:1079–1092. doi:10.2147/IJGM.S300270
- Smith V, Devane D, Begley CM, Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol. 2011;11(1):15. doi:10.1186/1471-2288-11-15
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
- Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi:10.1136/bmj.n160
- Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
- Whiting P, Savović J, Higgins JP, et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. 2016;69:225–234. doi:10.1016/j.jclinepi.2015.06.005
- Wang X, Chen Y, Liu Y, et al. Reporting items for systematic reviews and meta-analyses of acupuncture: the PRISMA for acupuncture checklist. BMC Complement Altern Med. 2019;19(1):208. doi:10.1186/s12906-019-2624-3
- Atkins D, Best D, Briss PA, et al. Grading quality of evidence and strength of recommendations. BMJ. 2004;328(7454):1490. doi:10.1136/bmj.328.7454.1490
- Lou JL, Sun HJ, Li XY, et al. Clinical efficacy and safety of moxibustion as adjuvant therapy for COPD in stable phase: a Meta-analysis (in Chinese). Zhongguo Zhen Jiu. 2021;41(4):451–457. doi:10.13703/j.0255-2930.20200213-k0004
- Wang YD, Li FS, Li Z, Yue JN, Ma CL. Systematic evaluation of acupuncture and moxibustion on pulmonary rehabilitation in patients with Stable Chronic Obstructive Pulmonary Disease (in Chinese). Mod Trad Chin Med Mater Medica World Sci Technol. 2020;22(01):196–204. doi:10.11842/wst.20190222003
- Xie HF. Systematic review and meta-analysis of acupuncture treatment for acute exacerbation of COPD. [ Master’s thesis]. Beijing (China): Beijing University of Chinese Medicine; 2019.
- Cao AL, He HL, Zhou XM. Meta analysis of the therapeutic effect of acupuncture on chronic obstructive pulmonary disease (in Chinese). Global Tradit Chin Med. 2017;10(07):899–904. doi:10.3969/j.issn.1674-1749.2017.07.038
- Yuan Y. Meta-analysis of Governor Moxibustion to Improve clinical efficacy and quality of life of chronic obstructive pulmonary disease (in Chinese). J Med Informa. 2022;35(01):93–99. doi:10.3969/j.issn.1006-1959.2022.01.022
- Yu MX, Huang HR, Huang YX, Yu ZL, Wu CJ. Effect of Du moxibustion on rehabilitation in patients with chronic obstructive pulmonary disease in Stable Stage: a Meta-analysis (in Chinese). Fujian J Tradit Chin Med. 2022;53(09):54–59. doi:10.13260/j.cnki.jfjtcm.012553
- Coyle ME, Shergis JL, Huang ET, et al. Acupuncture therapies for chronic obstructive pulmonary disease: a systematic review of randomized, controlled trials. Altern Ther Health Med. 2014;20(6):10–23.
- Fernández-Jané C, Vilaró J, Fei Y, et al. Filiform needle acupuncture for copd: a systematic review and meta-analysis. Complement Ther Med. 2019;47:102182. doi:10.1016/j.ctim.2019.08.016
- Hsieh PC, Yang MC, Wu YK, et al. Acupuncture therapy improves health-related quality of life in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Complement Ther Clin Pract. 2019;35:208–218. doi:10.1016/j.ctcp.2019.02.016
- Gu C, Yu Y, Chen Y, et al. Effect of acupoint catgut embedding combined with western medicine on patients with stable COPD: acupoint catgut embedding treating stable COPD meta-analysis. Medicine. 2023;102(41):e35281. doi:10.1097/MD.0000000000035281
- He WQ, Li JS, Wang MH. Literature analysis of acupoint catgut embedding therapy for chronic obstructive pulmonary disease (in Chinese). J Basic Chin Med. 2022;28(07):1140–1146. doi:10.19945/j.cnki.issn.1006-3250.2022.07.018
- Cheng JP, Niu GH, Chen JW, Shen XK, Wu YT. Meta-analysis of the acupoint application therapy of “Treating Winter Diseases in Summer” for chronic obstructive pulmonary disease: an updated systematic review (in Chinese). Clin J Tradit Chin Med. 2019;31(12):2270–2276. doi:10.16448/j.cjtcm.2019.0657
- Wu D, Yang C, Tong JB, Zhang XX, Yang QJ, Li ZG. Meta analysis of acupoint application in the prevention and treatment of chronic obstructive pulmonary disease (in Chinese). Mod Trad Chin Med Mater Medica World Sci Technol. 2019;21(11):2491–2498. doi:10.16448/j.cjtcm.2019.0657
- Hu HY, Sun MY, Zhu ZY, Xuan LH, Yu BY. Systematic assessment and meta-analysis of acupoint application for stable chronic obstructive pulmonary (in Chinese). Shanghai J Acu and Mox. 2019;38(08):932–940. doi:10.13460/j.issn.1005-0957.2019.08.0932
- Yu JJ, Wang J, Cai CS. A meta-analysis of point application on pulmonary rehabilitation in patients with stable chronic obstructive pulmonary disease (in Chinese). Clin J Chin Med. 2018;10(25):1–5. doi:10.3969/j.issn.1674-7860.2018.25.001
- Wei Y, Yuan N, Dong Y, Wang L, Ding J. Transcutaneous electrical nerve stimulation over acupoint for chronic obstructive pulmonary disease: a systematic review and meta-analysis. Front Public Health. 2022;10:937835. doi:10.3389/fpubh.2022.937835
- Pang LJ, Zhang H, Lu XD, Liu JP, Liu C, Lu L. Preventive and therapeutic effectiveness of Sanfu acupoint herbal patching for chronic obstructive pulmonary disease at stable stages: a systematic review and Meta-analysis (in Chinese). J Tradit Chin Med. 2020;40(04):530–549. doi:10.19852/j.cnki.jtcm.2020.04.003
- Zhou F, Shan YW, Lewith G, Liu JP. Acupoint Herbal Patching with or without Conventional Treatment for Stable Chronic Obstructive Pulmonary Disease: systematic Review of Randomized Controlled Trials (in Chinese). World J Tradit Chin Med. 2015;1(01):45–58. doi:10.15806/j.issn.2311-8571.2014.0013
- Huang C, Chen C, Zhou R, et al. A systematic review and meta-analysis of acupoint autohemotherapy and western medicine therapy in treating chronic obstructive pulmonary disease. Complement Ther Clin Pract. 2021;43:101336. doi:10.1016/j.ctcp.2021.101336
- Wang LM, Tang L, Shi MJ, et al. Meta-analysis and Grade evaluation of acupoint application in treatment of chronic obstructive pulmonary disease (in Chinese). Tianjin Chin Med. 2023;40(10):1292–1303. doi:10.11656/j.issn.1672-1519.2023.10.13
- Yin YQ, Zeng JR, Shen F. Meta-analysis of the acupoint application therapy for stable chronic obstructive pulmonary disease (in Chinese). J Hainan Med Univ. 2023;21:1655–1663. doi:10.13210/j.cnki.jhmu.20230515.001
- Zhang XF, Xiang SY, Geng WY, et al. Electro-acupuncture regulates the cholinergic anti-inflammatory pathway in a rat model of chronic obstructive pulmonary disease. J Integr Med. 2018;16(6):418–426. doi:10.1016/j.joim.2018.10.003
- Zou Y, Bhat OM, Yuan X, et al. Release and actions of inflammatory exosomes in pulmonary emphysema: potential therapeutic target of acupuncture. J Inflamm Res. 2021;14:3501–3521. doi:10.2147/JIR.S312385
- Li J, Wu S, Tang H, et al. Long-term effects of acupuncture treatment on airway smooth muscle in a rat model of smoke-induced chronic obstructive pulmonary disease. Acupunct Med. 2016;34(2):107–113. doi:10.1136/acupmed-2014-010674