

Abstract
Purpose
Breathlessness is a predominant symptom of chronic obstructive pulmonary disease (COPD), making it a valuable outcome in addition to lung function to assess treatment benefit. The phosphodiesterase-4 inhibitor roflumilast has been shown to provide small but significant improvements in dyspnea, as measured by the transition dyspnea index (TDI), in two 1-year studies in patients with severe to very severe COPD.
Patients and methods
To provide a more comprehensive assessment of the impact of roflumilast on dyspnea, post hoc analyses of four 1-year roflumilast studies (M2-111, M2-112, M2-124, and M2-125) in patients with moderate to very severe COPD were conducted.
Results
In this pooled analysis (N=5,595), roflumilast significantly improved TDI focal scores versus placebo at week 52 (treatment difference, 0.327; P<0.0001). Roflumilast was associated with significantly greater TDI responders and significantly fewer TDI deteriorators (≥1-unit increase or decrease from baseline, respectively) versus placebo at week 52 (P<0.01, both); these significant differences were apparent by week 8 and maintained until study end (P<0.05, all). At study end, the postbronchodilator forced expiratory volume in 1 second improvement in TDI responders was significantly greater with roflumilast versus placebo (P<0.05). Similar to the overall population, improvements in TDI focal scores at week 52 were small but consistently significant over placebo in patients with chronic bronchitis, regardless of exacerbation history, concomitant treatment with short-acting muscarinic antagonists or long-acting β2-agonists, or pretreatment with inhaled corticosteroids.
Conclusion
This analysis shows that patients treated with roflumilast to reduce exacerbation risk may also experience small but significant improvements in dyspnea, with accompanying improvements in lung function.
Supplementary materials
Figure S1 TDI responders (A) and deteriorators (B) over time for the subpopulation of patients with chronic bronchitis.
Notes: *P<0.05; **P≤0.01; ***P≤0.001 versus placebo.
Abbreviations: LOCF, last observation carried forward; n, number of responders; N, number of patients analyzed; TDI, transition dyspnea index.
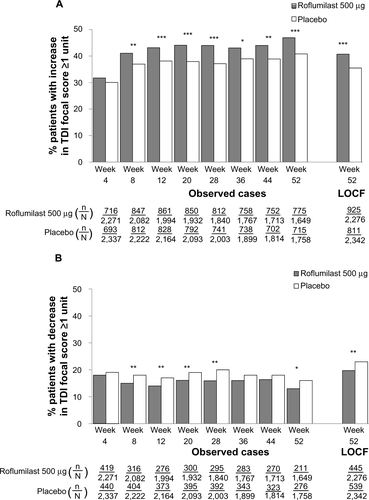
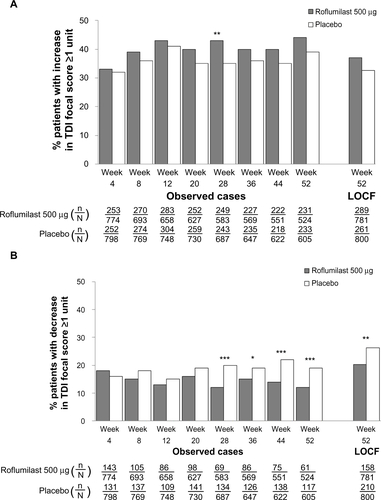
Figure S2 TDI responders (A) and deteriorators (B) over time for the subpopulation of patients with chronic bronchitis and a history of exacerbations.
Notes: *P<0.05; **P≤0.01; ***P≤0.001 versus placebo.
Abbreviations: LOCF, last observation carried forward; n, number of responders; N, number of patients analyzed; TDI, transition dyspnea index.
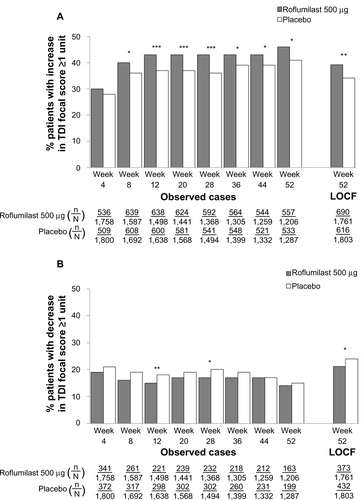
Figure S3 TDI responders (A) and deteriorators (B) over time for the subpopulation of patients with chronic bronchitis, a history of exacerbations, and pretreatment with inhaled corticosteroids.
Notes: *P<0.05; ***P≤0.001 versus placebo.
Abbreviations: LOCF, last observation carried forward; n, number of responders; N, number of patients analyzed; TDI, transition dyspnea index.
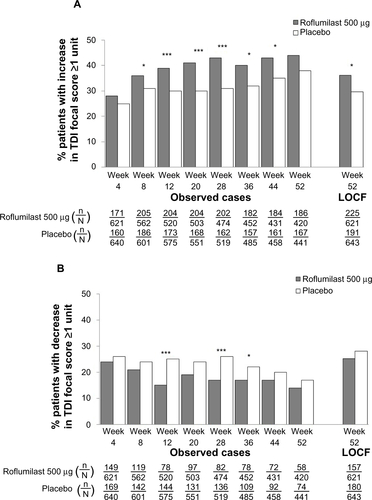
Figure S4 TDI responders (A) and deteriorators (B) over time for the subpopulation of patients with chronic bronchitis, a history of exacerbations, and concomitant long-acting β2-agonist treatment.
Notes: *P<0.05; **P≤0.01; ***P≤0.001 versus placebo.
Abbreviations: LOCF, last observation carried forward; n, number of responders; N, number of patients analyzed; TDI, transition dyspnea index.
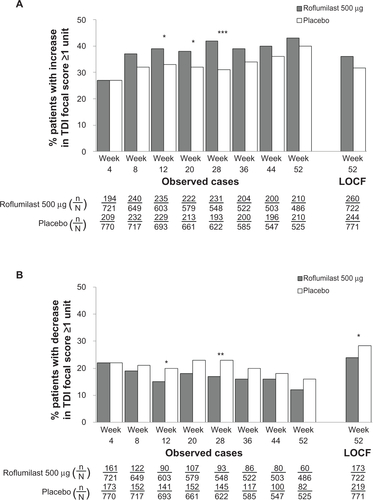
Figure S5 TDI responders (A) and deteriorators (B) over time for the subpopulation of patients with chronic bronchitis and concomitant short-acting muscarinic antagonist treatment.
Notes: *P<0.05; **P≤0.01.
Abbreviations: LOCF, last observation carried forward; n, number of responders; N, number of patients analyzed; TDI, transition dyspnea index.
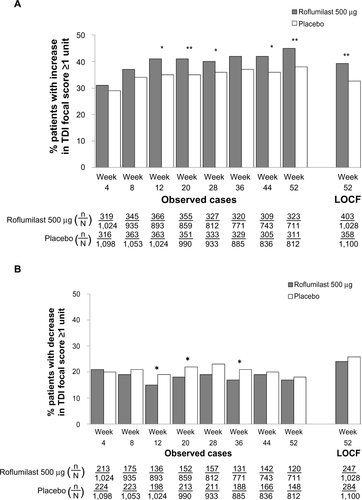
Figure S6 TDI responders (A) and deteriorators (B) over time for the subpopulation of patients with concomitant inhaled corticosteroid treatment.
Notes: *P<0.05; **P≤0.01; ***P≤0.001 versus placebo.
Abbreviations: LOCF, last observation carried forward; n, number of responders; N, number of patients analyzed; TDI, transition dyspnea index.
Acknowledgments
The authors would like to thank Dana Creanga, PhD, a contractor employed by Forest Research Institute, Inc., at the time of these analyses, for assistance with data analysis. Medical writing and editorial support was provided by Prescott Medical Communications Group (Chicago, IL, USA) and was funded by Forest Research Institute, Inc. Studies were sponsored by Takeda Pharmaceuticals International GmbH (Zürich, Switzerland). Analyses were performed by Forest Research Institute (Jersey City, NJ, USA), a wholly owned subsidiary of Forest Laboratories, Inc., (New York, NY, USA). The sponsors were kept informed throughout the development of the manuscript. All scientific decisions were made by the authors independently and without restrictions of any kind. The sponsors had no involvement in the decision to submit the manuscript for publication.
Disclosure
Stephen I Rennard has served as a consultant or participated in advisory boards for: ABIM, Able Associates, Adelphi Research, Almirall, APT, Aradigm, Argenta, AstraZeneca, BI (ACCP), Biostrategies, BoomCom, Britnall and Nicolini, Capital Research, Chiesi, Clinical Advisors, CommonHealth, Complete Medical Group, Consult Complete, COPDForum, DataMonitor, Decision Resources, Defined Health, Dey, Dunn Group, Easton Associates, Enterprise Analysis, Equinox, Forest, Fulcrum, Gerson Lehman, GSK, Guidepoint, Hoffman LaRoche, IMS, Informed, Inspire, Insyght, KOL Connection, Leerink Swan, M Pankove, MDRx Financial, MedaCorp, Medimmune, Mpex, Novartis, Nycomed, Oriel, Otsuka, Pearl, Pennside Partners, Pfizer, Pharma Ventures, Pharmaxis, Pick Research, Prescott, Price Waterhouse, Propagate, Pulmatrix, Pulmonary Reviews, Quadrant, Reckner Associates, Recruiting Resource, Reviews and Trends in COPD/Convergent Health Solutions, Roche, Sacoor, Schering, Schlesinger Medical, Scimed, Smith Research, Sudler and Hennessey, Talecris, Theravance, UBC, Uptake Medical, and Vantage Point. He has received lecture fees from AAAAI, Am Col Osteopathic Physicians, Asan Medical Center, ATS, AstraZeneca, California Soc Allergy, Convergent Health Solutions for Reviews and Trends in COPD, COPD Foundation, Creative Educational Concepts, Dey, Duke, France Foundation, Information TV, University of California-Los Angeles, Network for Continuing Education, Novartis, Nycomed, Otsuka, Pfizer, Sarasota Mem Hospital, Spanish Thoracic Society, University of Washington, University of Alabama-Birmingham, University of Pittsburgh, University of British Columbia, University of California-Davis, VA Sioux Falls. He has received industry-sponsored grants from AstraZeneca, Biomarck, Centocor, GlaxoSmithKline, Mpex, Nabi, Novartis, Otsuka, and Pfizer. Peter M A Calverley has given presentations at symposia sponsored by Astra Zeneca, Boehringer, GlaxoSmithKline, and Nycomed, and has received fees for advising Astra Zeneca, Boehringer, GlaxoSmithKline, Novartis, and Nycomed. Shawn X Sun, Stavros Tourkodimitris, and Paul Rowe are employees of Forest Research Institute, Inc. Udo M Goehring and Dirk Bredenbröker are employees of Takeda Pharmaceuticals International GmbH.