

Abstract
Background
Olodaterol is a long-acting β2-agonist with a 24-hour bronchodilator profile. Two replicate, randomized, double-blind, placebo-controlled, parallel-group, Phase III trials were performed as part of a comprehensive clinical program to investigate the long-term safety and efficacy of olodaterol in patients with moderate to very severe chronic obstructive pulmonary disease (COPD) receiving usual-care background therapy.
Methods
Patients received olodaterol 5 μg or 10 μg or placebo once daily for 48 weeks. Coprimary end points were forced expiratory volume in 1 second (FEV1) area under the curve from 0 to 3 hours (AUC0–3) response (change from baseline), and trough FEV1 response at 12 weeks. Secondary end points included additional lung function assessments, use of rescue medications, FEV1 AUC response from 0 to 12 hours, and Patient Global Rating over 48 weeks.
Results
Overall, 624 and 642 patients were evaluated in studies 1222.11 and 1222.12, respectively. In both studies, olodaterol 5 μg and 10 μg significantly improved the FEV1 AUC0–3 response (P<0.0001) and trough FEV1 (study 1222.11, P<0.0001; study 1222.12, P<0.05, post hoc) at week 12, with an incidence of adverse events comparable with that of placebo. Secondary end points supported the efficacy of olodaterol.
Conclusion
These studies demonstrate the long-term efficacy and safety of once-daily olodaterol 5 μg and 10 μg in patients with moderate to very severe COPD continuing with usual-care maintenance therapy.
Online supplementary tables and figures
Figure S1 Participant flow in study 1222.11 (A) and study 1222.12 (B).
Notes: aOne patient not treated because electrocardiogram was reviewed after randomization and was abnormal; bone patient was excluded due to lack of Health Insurance Portability and Accountability Act authorization; one patient discontinued prior to first drug dose.
Abbreviations: QD, once daily; AE, adverse event.
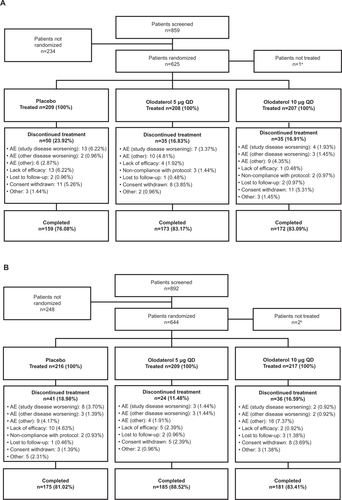
Figure S2 FEV1 over time from 1 hour pre-dose to 3 hours post-dose in the combined data set at day 1 (A) and week 12 (B).
Abbreviations: FEV1, forced expiratory volume in 1 second; h, hours.
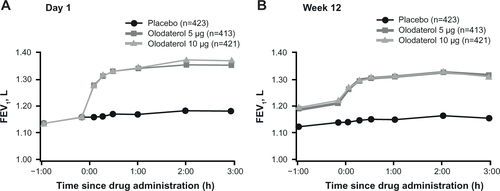
Figure S3 Weekly mean morning (A) and evening (B) PEFR over 48 weeks in study 1222.11 and study 1222.12.
Abbreviation: PEFR, peak expiratory flow rate.
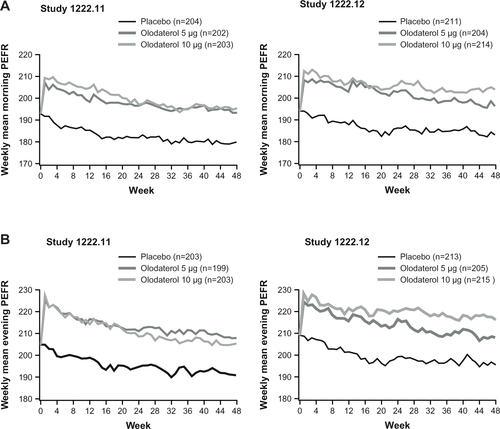
Figure S4 Daytime (A) and nighttime (B) rescue medication use (combined data set).
Note: Value plotted at week 0 is common baseline mean (daytime =1.200 actuations/day; nighttime =2.218).
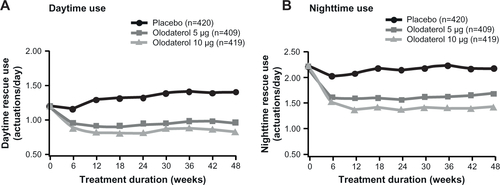
Table S1 Null and alternative hypotheses
Table S2 Comparison of lung function results based on the original and revised statistical models
Table S3 Adjusted mean FEV1 responses (absolute change from baseline) at key time points
Table S4 Adjusted mean FEV1 responses at key time points in tiotropium and non-tiotropium groups in the combined data set
Table S5 Adjusted mean rescue medication (difference from placebo) at key time points
Table S6 Adjusted mean PGR (difference from placebo) at key time points
Disclosure
The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors. They take full responsibility for the scope, direction, content of, and editorial decisions relating to, the manuscript, were involved at all stages of development, and approved the submitted manuscript. The authors received no compensation related to the development of the manuscript. This work was supported by Boehringer Ingelheim Pharma GmbH and Co, KG. Medical writing assistance was provided by Claire Scofield of Complete HealthVizion, which was contracted and compensated by Boehringer Ingelheim Pharma GmbH and Co, KG.