
Abstract
Background
Long-acting inhaled bronchodilators, including anticholinergic tiotropium, are recommended for the maintenance therapy of chronic obstructive pulmonary disease (COPD). It has been shown in a number of studies that treatment with tiotropium alleviates symptoms, improves exercise tolerance, health status, and reduces exacerbations in patients with moderate to very severe stage COPD.
Aim
The aim of this noninterventional study was to observe the early effects of the maintenance treatment with tiotropium in patients with COPD of different severities, who had been previously treated on a regular basis, or as required, with at least one short-acting bronchodilator, in a real-life setting in Poland. The effect of the treatment was assessed through the collection of COPD Assessment Test (CAT) data.
Patients and methods
The MATHS clinical study was an observational, noninterventional, open-label, prospective, uncontrolled, single-arm, postmarketing, surveillance, real-life study conducted with the involvement of 236 pulmonology clinics based in Poland. The tiotropium observational period was 3 months. The health and COPD status was measured with the CAT questionnaire. The primary efficacy endpoint was the mean change from the baseline in the total CAT score at the end of the 3-month observational period.
Results
Patients treated with 18 μg of tiotropium once daily for 3 months showed a statistically significant result, with a clinically meaningful mean reduction (improvement) of 7.0 points in the total CAT score. The improvement was slightly greater in patients with more severe COPD; the mean change in the total CAT score was 7.6 in the subgroup of patients with more severe COPD and 6.7 points in the subgroup of patients with moderate COPD.
Conclusion
Results of this real-life study provide further support for the use of tiotropium as a first-line maintenance treatment for patients with COPD of different severities in Poland.
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable, and treatable disease, which is characterized by persistent airflow limitation that is usually progressive. According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Summary and the World Health Organization (WHO), COPD is the fourth leading cause of death in the world, and in 2020 it will become the third most common cause of death.Citation1 Polish statistics show that about two million people suffer from COPD in Poland, although this number is likely to be underestimated.Citation2 Data from the Central Statistical Office confirm that lung disorders (including the most prevalent, COPD) are also the fourth most common cause of death in Poland.Citation3
The main characteristic of COPD – airflow limitation – is caused by small airways disease and the destruction of lung parenchyma. Tobacco smoking is the main risk factor of COPD.
The main objectives of effective treatment of COPD patients are symptom alleviation, improvement in exertion tolerance, improvement in health-related quality of life (HRQoL) and general health status, and an increase in survival, as well as exacerbation prevention. Bronchodilators (most common β2 agonists and anticholinergics) are the main medicines used in COPD patients and help reduce dynamic hyperinflation. According to GOLD and the Polish Society of Lung Diseases (PTChP) guidelines, long-acting inhaled bronchodilators are convenient and more effective at relieving symptoms than short-acting bronchodilators for patients with stable moderate to severe stage COPD.Citation1,Citation4 Results of a study on the compliance of treatment with medications for COPD showed that patients treated with inhaled tiotropium remained on therapy significantly longer than patients treated with other medications.Citation5
Spiriva® (Tiotropium Bromide; Boehringer Ingelheim Pharma and Co, KG, Ingelheim, Germany) is a long-acting muscarinic antagonist (LAMA) that is administered once daily with a dosage of 18 μg via a HandiHaler® or 5 μg (two 2.5 μg puffs) via a Respimat® inhalator. It is indicated for the maintenance treatment of patients with COPD (including chronic bronchitis and emphysema), the maintenance treatment of associated dyspnea, and for a reduction in the risk of COPD exacerbations.Citation6 The key effect of tiotropium action is a prolonged blockade of muscarinic M3 receptors in the lungs, which decreases bronchial constriction and improves airflow and hyperinflation in patients with COPD. The anticholinergic action of tiotropium lasts up to 24 hours.Citation1,Citation7 Clinical trials with tiotropium that examined patients of different COPD severity over a period of 6 months–4 years showed that it increases the mean predose morning FEV1, reduces dyspnea, improves HRQoL (assessed with St George’s Respiratory Questionnaire – SGRQ), prevents exacerbations and related hospitalization, and prolongs survival.Citation6–Citation13 The COPD Assessment Test (CAT), which was used in this study, is a short, simple instrument for quantifying the influence of COPD symptoms on patients’ life in routine practice, to aid health status assessment, and to facilitate communication between patient and health care professionals.
An extensive network meta-analysis published by Kew et al showed that treatment with LAMA is the second highest ranked intervention regarding improvement in HRQoL as measured by the SGRQ.Citation14 The clinical studies included in this meta-analysis also provide evidence that the beneficial effects of tiotropium on HRQoL in patients with different severities of COPD are extensive. However, its effect has not yet been confirmed in the real-life setting of Polish COPD patients treated previously with short-acting bronchodilators, and our study aims at filling this gap.
Methods and disposition of patients
Study objective
The objective of this observational study was to evaluate the impact of tiotropium on the COPD status of Polish patients over a period of 3 months using the specific CAT questionnaire.
Detailed endpoints covered:
comparison of the total CAT score at the baseline and after 3 months of tiotropium treatment in patients with different COPD severities,
assessment of the frequency of use of short-acting bronchodilators (used by patients when required) at the baseline and during the 3-month tiotropium treatment observational period,
assessment of the safety of the treatment with tiotropium in COPD patients.
The study was performed in accordance with the Declaration of Helsinki and the International Conference on Harmonisation/Good Clinical Practice standards. It was approved by the Bioethics Committee of Military Institute of Medicine, Warsaw, Poland, in accordance with the Polish regulations on October 19, 2011. The study was carried out in compliance with the protocol; Subject Information and Consent have been used. Only patients who consented to participate in the study were enrolled.
Study design
The MATHS clinical study was an observational, non-interventional, open-label, prospective, uncontrolled, single-arm, postmarketing, surveillance study conducted with the involvement of 236 pulmonology clinics based in Poland. The observational period of tiotropium was 3 months, with an objective to collect and evaluate data on health and COPD status as measured by the CAT.
The study consisted of two main and one voluntary ambulatory clinic visits over a period of 3 months: visit 1 was the baseline visit at day 1, visit 2 could take place between the first and the second month of observation (day 20–60), and visit 3 was scheduled after 3 months (day 90), at the end of the observational period. Considering the noninterventional nature of the study, the schedule of visits was only tentative.
Male and female outpatients with stable COPD at various stages (according to GOLD 2010) being seen in a participating physician’s office for routine care were included in the study. The diagnosis of COPD was established by investigators according to the routine clinical practice and medical standards. Patients could have been treated (or not) with tiotropium within the last 4 weeks before entering the study (but not longer than 28 days prior to visit 1) and should have been suitable for long-bronchodilator treatment according to the product label.Citation15 Inclusion criterion was also previous treatment (on a regular basis or as required) with at least one short-acting bronchodilator for at least 3 months before changing the treatment for long-acting anticholinergic preparation. All patients included in the study had to be fluent in the language of the questionnaire (Polish) and have the cognitive and functional ability required to fill in the questionnaire on their own.
There were no restrictions on concomitant, rescue, and additional medications required by study participants. However, all treatment decisions for the regimen remained with the patient’s physician. Uncooperative patients, as judged by the physician, were excluded, as well as patients with any conditions specified as contraindication according to the approved Spiriva® product label in Poland,Citation15 currently enrolled in another clinical trial, or with COPD exacerbation, or any other acute disease within 3 months preceding enrollment. According to the study protocol, there was no situation specified for the removal of patients from the therapy. The treating physician was the only one who could make the decision to discontinue therapy on the basis of clinical judgment.
Statistical analysis
In this observational study, the health and COPD status under the treatment with tiotropium was measured using the CAT questionnaire. The sample size was calculated on the basis of range of confidence interval (CI) calculated for the proportion of respondents. Assuming 50% response rate and 95% CI being ±3%, the sample size was calculated as 1,068 patients. For 99% CI, the corresponding number was 1,810 patients. Data were analyzed descriptively with the calculation of 95% CIs. For continuous data, all statistical parameters were described by the mean, standard deviation, first quartile, third quartile, minimum value, and maximum value. Statistical analysis of the safety parameters included the data of all patients with a documented baseline visit (visit 1). Statistical analyses of the efficacy parameters included all patients with a documented baseline visit (visit 1), at least one dose of Spiriva® 18 μg taken, and available data on the respective efficacy parameter (CAT) at the end of the observational period (visit 3). It was not intended to replace missing data or extrapolate available data. The data analyzed were age, sex, weight, height, diagnosis, smoking history, COPD severity stage according to GOLD, concomitant diseases, concomitant pulmonary medication, adverse events, information on treatment continuation, reasons for study discontinuation, total CAT score at the baseline and after 3 months of the treatment, and the frequency of using the short-acting bronchodilators. COPD GOLD stages were presented as reported by investigators and not evaluated on the basis of spirometry results.
The study population
Treated set (TS) included all patients who were dispensed study medication and were documented to have taken at least one dose of investigational treatment. Full analysis set (FAS) included all patients in the TS who had valid CAT questionnaire results both at the baseline (visit 1) and at visit 3.
Based on the COPD severity, as per GOLD, patients were divided into two groups – COPD stage I and II formed the moderate COPD population, and COPD stage III and IV formed the severe COPD population.
An efficacy analysis was presented for the FAS population, while a safety analysis was presented for the TS population. The Student’s t-test was used to test the change in the overall CAT score (change in the score between visit 1 and visit 3) for paired variables. For all statistical tests, the significance level α was fixed at 5%. However, any P-values and CIs were only calculated for exploratory purposes. The R Project program was used for statistical analysis.
CAT questionnaire
CAT is a short, simple questionnaire for quantifying the influence of COPD symptoms on a patient’s life in routine practice. The test consists of eight items, each presented as a semantic 6-point differential scale, providing a score out of 40, which indicates the impact of the disease. It covers cough, phlegm, chest tightness, breathlessness going up hills/stairs, activity limitation at home, confidence leaving home, sleep, and energy. Scores of 0–10, 11–20, 21–30, and 31–40 represent mild, moderate, severe, or very severe clinical impact, respectively.Citation16–Citation18 The items related to cough and phlegm have a greater discriminatory power for milder stage COPD; items concerning chest tightness and confidence leaving home are more discriminative in severe COPD, and the remaining items capture moderate health status impairment. The minimum clinically important difference (MCID) of the CAT questionnaire is 2 points.Citation19 The CAT questionnaire has good repeatability, and its discriminative properties suggest that it is sensitive to treatment effects.
Results
Disposition of patients
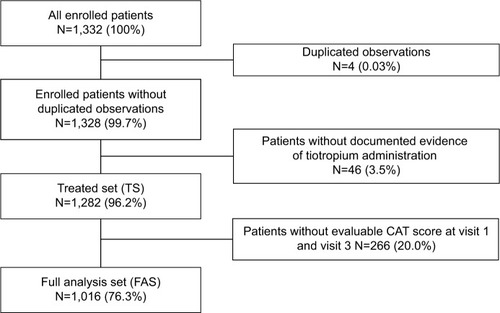
There were 1,332 patients enrolled in this study. Four observations, being duplicated, were excluded from TS, and 46 patients showing no evidence of tiotropium administration were excluded from the TS. No adverse events (AEs) were recorded in these patients. In 1,282 patients, administration of at least one dose of tiotropium was documented; these patients represent TS. FAS consisted of 1,016 patients with an available CAT score at visit 1 and at visit 3. The exact disposition of the patients into analysis sets is presented in .
Figure 1 Disposition of patients.
Demographic and baseline characteristics
The FAS population consisted of 1,016 patients, 61.3% of them male. Most of the patients (58.4%) were between 60 and 80 years of age and had normal BMI (75.9% of patients). The baseline demographic and characteristics of the total FAS population and COPD subgroups are listed in .
Table 1 Baseline characteristics – total FAS population and subgroups
Concerning the smoking history, 85.2% of the total FAS population were current or ex-smokers. The details of smoking history in the total FAS population and subgroups are presented in .
In the total FAS population, the average number of cigarettes smoked per day was 20.5 (SD=7.8) for ex-smokers and 17.8 (SD=7.4) for current smokers. The approximate number of years of smoking was 28.5 (SD=10.5) for ex-smokers and 31.7 (SD=10.4) for current smokers. The mean pack-years value was 30.6 (SD=18.9) for ex-smokers and 28.0 (SD=14.9) for current smokers.
In the FAS population, the mean time since COPD diagnosis to the start of the study (visit 1) was 5.9 years (SD=6.1). The moderate COPD population encompassed 506 patients and the severe COPD population 341. Detailed COPD characteristics of the total FAS population and subgroups are presented in .
Of the 1,016 patients in the FAS population, 754 had concomitant therapy related to respiratory disorders during the 3-month observational period. Most of the patients from the concomitant therapy subgroup were in COPD stage II and III (n=310 [41.1% of all patients with concomitant therapy] and 238 [31.6%], respectively). In the moderate COPD population, 353 (69.8%) patients had concomitant therapy related to respiratory disorders during the 3-month observational period, and in the severe COPD population, 281 (82.4) had concomitant therapy during the observational period ().
Table 2 Concomitant therapy related to respiratory disorders by COPD subgroups (FAS)
Before the start of the treatment with tiotropium, patients were treated for at least 3 months on a regular basis or as required, with at least one short-acting bronchodilator. In 1,016 patients in the FAS population, the most frequently used bronchodilators were ipratropium (45.6% of patients) and salbutamol (29.5%). The medicine most frequently used as required was salbutamol (24.4%), and the bronchodilator most frequently used on a regular basis was ipratropium (28.6%).
In the FAS population, long-acting medicines for COPD were used by 727 patients: formoterol was used by 18.0% of the patients and theophylline by 15.8% of the patients. Concomitant medication for COPD used by the patients is presented in .
Table 3 Concomitant medication
Moreover, 789 (77.7%) of the 1,016 patients in the FAS population had at least one relevant concomitant disease at the baseline (visit 1).
The most frequently reported relevant concomitant diseases (according to MedDRA system organ class and preferred term) were:
Vascular disorders – 439 patients (43.2%)
Cardiac disorders – 427 patients (42.0%)
Gastrointestinal disorders – 212 patients (20.9%)
Metabolism and nutrition disorders – 148 patients (14.6%)
Reproductive system and breast disorders – 71 patients (7.0%)
Musculoskeletal and connective tissue disorders – 59 patients (5.8%).
Efficacy
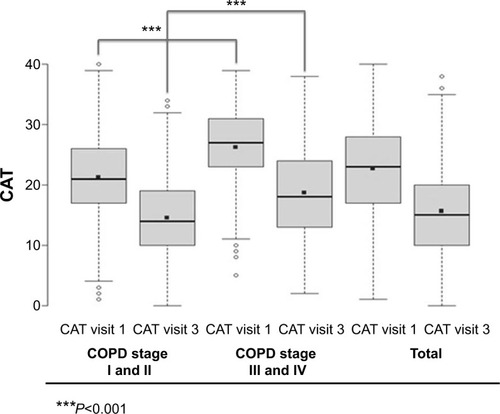
The mean CAT score at the baseline (visit 1) for the total FAS population was 22.7 points (SD=7.7). The score was lower in patients with moderate COPD (21.2, SD=7.4) than in patients with more severe COPD (26.3, SD=6.7, P<0.001). After 3 months of tiotropium treatment, the total CAT score decreased to 15.7 points (SD=7.4) for the total FAS population, and again it was lower in moderate COPD patients in comparison with patients with more severe COPD (14.5, SD=6.8 vs 18.7, SD=7.8; P<0.001) ().
Figure 2 Overall CAT score at visit 1 and visit 3 by COPD stage – FAS.
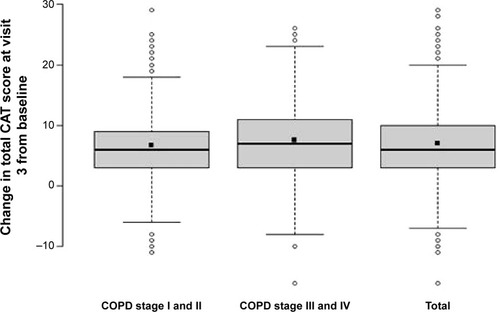
The mean change in the total CAT score after 3 months of treatment with tiotropium was 7.0 points (SD=5.9); patients in all COPD stages improved significantly. The improvement was greater in the patients with more severe COPD; the mean change in the total CAT score was 6.7 points (SD=5.4) in the subgroup of patients with moderate COPD, and 7.6 (SD=6.4) in the subgroup of patients with severe COPD (P-value within groups <0.001, P-value between groups =0.041). The results are presented in .
Figure 3 Change in the total CAT score at visit 3 from the baseline depending on COPD stage – FAS.
In the total FAS population, 2.9% of patients worsened by ≤−2 points, 1.5% of patients worsened by −2 to 0 points, 2.4% of patients had no change in the overall CAT score (0 points difference), 3.4% of patients improved by 0–2 points, and 89.9 improved by ≥2 points.
An analysis of the subgroups revealed the following: worsening by ≤−2 points was observed in 2.6% of patients with moderate COPD vs 3.8% of patients with more severe COPD; worsening by −2 to 0 points was observed in 1.8% of patients with moderate COPD vs 0.6% of patients with more severe COPD; no change in the overall CAT score (0 points difference) was observed in 2.8% of patients with moderate COPD vs 1.8% of patients with more severe COPD; improvement by 0–2 points was observed in 4.2% of patients with moderate COPD vs 2.6% of patients with more severe COPD; and improvement by ≥2 points in 88.7% vs 91.2%, respectively.
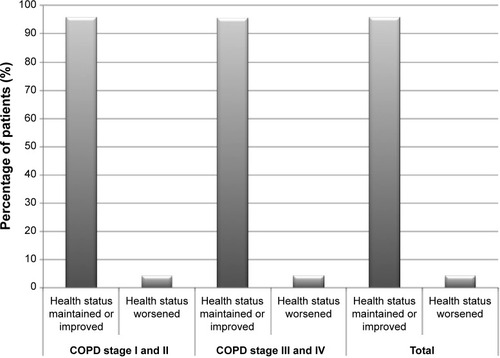
Maintenance or improvement of health and COPD status was also analyzed as a separate endpoint. Results are presented in . After 3 months of tiotropium treatment, maintenance or improvement of health status as measured with the CAT questionnaire was observed in 972 patients of the 1,016 in the total FAS population (95.7%); only 44 patients worsened (4.3%). There was no difference between COPD stage subgroups – 95.7% of the patients with moderate COPD and 95.6% of the patients with more severe COPD maintained or improved their health and COPD status (P=0.9716).
Figure 4 Maintenance or improvement of health and COPD status (measured by CAT) depending on COPD stage – FAS.
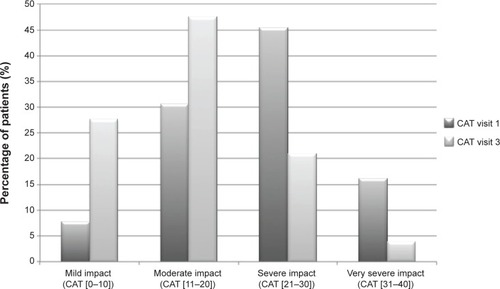
Next, the influence of COPD on the patients’ life was evaluated on the basis of the CAT score. The following grades of impact were assumed:
mild impact for a total CAT score between 0 and 10 points,
moderate impact for a total CAT score between 11 and 20 points,
severe impact for a total CAT score between 21 and 30 points,
very severe impact for a total CAT score between 31 and 40 points.
At the baseline, the majority of the patients (462, 45.5%) fell into the severe impact category, 311 (30.6%) patients were in the moderate impact category, 164 (16.1%) were in the very severe impact category, and 79 (7.8%) in the mild impact category. After 3 months of tiotropium treatment (visit 3), the majority of the patients (483, 47.5%) fell into the moderate impact category, 280 (27.6%) patients were in the mild impact category, 213 (21%) patients were in the severe impact category, and only 40 (4.9%) featured in the very severe impact category ().
Figure 5 Impact of COPD on patients’ health status at the baseline and after 3 months of tiotropium treatment – FAS.
The frequency of use of short-acting bronchodilators during the 3 months of tiotropium treatment decreased in 649 (50.6%) patients, while in six (0.5%) patients it increased, and in 179 (14%) patients there was no change.
Safety
The mean exposure to tiotropium was 92.4 (SD=22.8) days, and the majority of the patients were exposed between 91 and 105 days. The total exposure to tiotropium during this noninterventional study was 274.1 years. On voluntary visit 2, 706 of 712 patients (99.2%) decided to continue the treatment with tiotropium; on visit 3, this number was 1,007 of the 1,016 (99.1%) patients.
On voluntary visit 2, only 49 of 712 patients had changes in the concomitant COPD therapy, and 34 had newly added drugs for obstructive airway diseases (R03): seven (14.3%) of these patients had to additionally use salbutamol, six (12.2%) patients used fenoterol, six (12.2%) formoterol, five (10.2%) budesonide, four (8.2%) ipratropium, four (8.2%) theophylline, three (6.1%) fluticasone, three (6.1%) ipratropium and fenoterol, and one patient (2%) ciclesonide.
On visit 3, 47 of the 1,016 patients had changes in concomitant COPD therapy and 25 of 47 patients (53.2%) had new drugs for obstructive airway diseases (R03) added. The majority of these patients had to additionally use ipratropium (six, 12.8%), four (8.5%) patients used budesonide, 1onide and formoterol, four (8.5%) salbutamol, four (8.5%) salmeterol, three (6.4%) fenoterol, two (4.3%) ciclesonide, two (4.3%) formoterol, two (4.3%) ipratropium and fenoterol, one patient (2.1%) beclometasone, and one patient (2.1%) beclometasone and formoterol.
AEs analysis was undertaken for the TS population of patients. Of the 1,282 patients in the TS population, 25 (2%) patients reported AEs. Among all the AEs there were no serious AEs. Four patients (0.4%) with nine reported AEs discontinued study because of AE, among whom two experienced worsening of other preexisting diseases.
Most of the AEs were classified according to the MedDRA system organ class as respiratory, thoracic, and mediastinal disorders (nine patients, 0.7% of the total TS population), gastrointestinal disorders (eight patients, 0.6%), ear and labyrinth disorders (two patients), cardiac disorders (two patients), renal and urinary disorders (two patients), general disorders and administration site conditions (two patients), and investigations (two patients). Of the 1,282 patients in the TS population, 13 (1%) patients reported AEs, which were related to the study medication. The most commonly reported AEs related to the study medication were gastrointestinal disorders (dry mouth in six patients and nausea in one patient), cardiac disorders (two patients), renal and urinary disorders (two patients), and general disorders and administration site conditions (two patients). From the total number of 1,282 patients in the TS population, nine (0.7%) patients reported AEs, which led to treatment discontinuation. The most common AEs were classified as gastrointestinal disorders (three patients), renal and urinary disorders (two patients), general disorders and administration site conditions (two patients), and investigations (two patients). Among the 1,282 patients in the TS population, AEs that occurred in more than 5% of patients were not registered. Of all of the AEs, there were no serious AEs.
Discussion and conclusions
The objective of this noninterventional study was to evaluate the effects of the maintenance treatment with tiotropium in patients with COPD of different severities. Patients were previously routinely treated with different classes of pulmonary medicines including at least one short-acting bronchodilator used on a regular basis or as required in a real-life setting in Poland. The observational period with tiotropium was 3 months, and the treatment effect was assessed by the CAT.
Lung diseases including COPD which is the most common one, are fourth largest cause of death in Poland (after the heart and vascular diseases, cancer and sudden deaths).Citation4 Nevertheless, no epidemiological study on the incidence of COPD performed on a representative sample of the Polish population has been published. In the partial surveys, COPD was diagnosed in 10%–26% of participants above 40 years of age.Citation4 It was found in epidemiological studies that COPD is diagnosed in the early stages in less than 20% of patients; the majority of patients are diagnosed in the advanced stages of COPD (according to GOLD).Citation4 It is estimated that in Poland, approximately 80% of patients with COPD are in the mild to moderate stages of the disease and the disease is often underdiagnosed.Citation4
In the present study, men constituted the majority of the patients, which was consistent with the epidemiological data indicating a higher prevalence of COPD in Polish men.Citation4 In this study population, 42.6% of the patients were in the moderate COPD stage, 29.1% were in the severe COPD stage, 7.2% were in the mild COPD stage, and 4.4% of the patients were in the very severe COPD stage, which means that the study population represented more severe COPD than the average population in Poland. This can be explained by the fact that the study population was recruited from lung clinics.
The maintenance or improvement of health status (measured as a reduction in the total CAT score) after 3 months of treatment with tiotropium was achieved in 95.7% of the patients. The stage of COPD had no impact on the proportion of patients in whom an improvement was observed. This finding is concordant with the results of the TIPHON trial, where it was shown that the improvement of HRQoL after the treatment with tiotropium (reduction of at least 4 units in the SGRQ score) was similar in all disease severity subgroups.Citation9 Similarly, in the SOSPES observational study, in the total study population, the mean reduction of the SGRQ score from the baseline to month six was independent of the disease severity according to the GOLD classification. However, a significant difference in the change of the mean SGRQ score was observed in the subgroups of patients with GOLD stages II and III.Citation20
In the present study, the change in the total CAT score from visit 1 to visit 3 was greater in patients with more severe COPD stages (GOLD III and IV) than in those with moderate COPD (GOLD I and II).
It was interesting to observe that the quality of life of patients enrolled in this study, especially with more severe COPD stages, was very poor at the baseline, which shows that COPD patients in daily practice in Poland are severely impacted by their disease. Similar conclusions could be drawn from the results obtained for Polish patients during the SOSPES study.Citation20
The majority of patients (77.7%) enrolled in the present study had one or more concomitant diseases, with the most common being vascular and cardiac disorders, which is typical for COPD, as it is in most cases a complex condition.Citation1 The baseline mean CAT score in the total FAS population was 22.7 points. Concomitant diseases can also partially explain the high CAT score at the baseline. The CAT questionnaire includes questions related to limitations in daily activities, sleep, and energy, which can be influenced by vascular and cardiac disorders as well as other comorbidities. Nevertheless, the results of the study showed that tiotropium treatment is also effective in patients with concomitant diseases.
After 3 months of tiotropium treatment, the adverse impact of COPD on the patients’ life was reduced. At the beginning of the study, 45.5% of the patients reported the impact of the disease as severe, and after 3 months of treatment, almost half of the patients assessed it as moderate.
Efficacy of tiotropium was supported by the frequency of use of short-acting bronchodilators during the 3-month observational period; it decreased in 50.6% of the patients, it increased in 0.5% of the patients, and in 14.0% of the patients there was no change.
Analysis of safety showed a small number of AEs, and only 0.7% of patients from the TS had to discontinue the treatment because of AEs. There were no serious AEs reported in this study. However, underreporting cannot be excluded as one of the reasons for a low number of AEs, as this is often observed in noninterventional observational studies.
In conclusion, this observational study confirmed an additional benefit of maintenance treatment with tiotropium when introduced to patients of all COPD severity stages previously treated with different classes of pulmonary medicines, including short-acting bronchodilators, in real-life settings in Poland. Overall, treatment with tiotropium was safe, and beneficial effects were observed within the short period of treatment.
Acknowledgments
The authors thank Proper Medical Writing Sp. z o.o., Warsaw, Poland, for writing and the language assistance, and 2KMM Sp. z o.o., Katowice, Poland, for the statistical analysis provided in the preparation of this article.
Disclosure
Karina Jahnz-Różyk received research funding in the last 4 years from Boehringer Ingelheim, but has no other financial relationship relating to commercial activity that is of interest to the subject of this manuscript. Paweł Szepiel is an employee of Boehringer Ingelheim. The authors report no other conflicts of interest in this work.
References
- GOLD Executive Summary (revised 2014)Global strategy for the diagnosis, management and prevention of COPD Available from: http://www.goldcopd.com/Accessed November 5, 2014
- BednarekMMaciejewskiJWozniakMKucaPZielinskiJPrevalence, severity and underdiagnosis of COPD in the primary care settingThorax200863540240718234906
- Rocznik demograficzny 2010 [Statistical Yearbook 2010]Warsaw, PolandGłówny Urząd Statystyczny2011 Polish
- GóreckaDJassemEPierzchałaWŚliwińskiPZalecenia Polskiego Towarzystwa Chorób Płuc dotyczące rozpoznawania i leczenia przewlekłej obturacyjnej choroby płuc (POChP) [Recommendations of the Polish Society of Lung Diseases for diagnosis and treatment of chronic obstructive pulmonary disease (COPD)]Pneumonol Alergol Pol2012803220254 Polish22562274
- CramerJABradley-KennedyCScaleraATreatment persistence and compliance with medications for chronic obstructive pulmonary diseaseCan Respir J2007141252917315055
- BrusascoVHodderRMiravitllesMKorduckiLTowseLKestenSHealth outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients with COPDThorax200358539940412728159
- TashkinDPCelliBSennSfor UPLIFT Study InvestigatorsA 4-year trial of tiotropium in chronic obstructive pulmonary diseaseN Engl J Med2008359151543155418836213
- DonohueJFvan NoordJABatemanEDA 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterolChest20021221475512114338
- TonnelABPerezTGrosboisJMEffect of tiotropium on health-related quality of life as a primary efficacy endpoint in COPDInt J Chron Obstruct Pulmon Dis20083230131018686739
- DecramerMCelliBKestenSLystigTMehraSTashkinDPfor UPLIFT InvestigatorsEffect of tiotropium on outcomes in patients with moderate chronic obstructive pulmonary disease (UPLIFT): a pre-specified subgroup analysis of a randomised controlled trialLancet200937496961171117819716598
- TroostersTCelliBLystigTfor UPLIFT InvestigatorsTiotropium as a first maintenance drug in COPD: secondary analysis of the UPLIFT trialEur Respir J2010361657320185426
- VogelmeierCHedererBGlaabTfor POET-COPD InvestigatorsTiotropium versus salmeterol for the prevention of exacerbations of COPDN Engl J Med2011364121093110321428765
- MathioudakisAGKanavidisPChatzimavridou-GrigoriadouVTiotropium HandiHaler improves the survival of patients with COPD: a systematic review and meta-analysisJ Aerosol Med Pulm Drug Deliv2014271435023521168
- KewKMDiasSCatesCJLong-acting inhaled therapy (beta-agonists, anticholinergics and steroids) for COPD: a network meta-analysisCochrane Database Syst Rev20143CD01084424671923
- Spirivia Respimat 25 microgram, solution for inhalation [summary of product characteristics] IngelheimGermanyBoehringer Ingelheim2014
- DoddJWHoggLNolanJThe COPD assessment test (CAT): response to pulmonary rehabilitation. A multicentre, prospective studyThorax201166542542921398686
- JonesPWHardingGBerryPWiklundIChenWHKline LeidyNDevelopment and first validation of the COPD Assessment TestEur Respir J200934364865419720809
- CATestonline.org. COPD Assessment TestImproving COPD communication, improving care Available from: http://www.CATestonline.org/Accessed November 5, 2014
- KonSSCanavanJLJonesSEMinimum clinically important difference for the COPD Assessment Test: a prospective analysisLancet Respir Med20142319520324621681
- FležarMJahnz-RóżykKEnacheGSOSPES: SPIRIVA® observational study measuring SGRQ score in routine medical practice in Central and Eastern EuropeInt J Chron Obstruct Pulmon Dis2013848349224159258