
Abstract
Objective
We established a COPD taskforce for early detection, diagnosis, treatment, and intervention. We implemented a pilot intervention with a prospective and longitudinal design in a regional city. This study evaluates the usefulness of the COPD taskforce and intervention based on COPD case detection rate and per capita medical costs.
Method
We distributed a questionnaire to all 8,878 inhabitants aged 50–89 years, resident in Matsuura, Nagasaki Prefecture in 2006. Potentially COPD-positive persons received a pulmonary function test and diagnosis. We implemented ongoing detection, examination, education, and treatment interventions, performed follow-up examinations or respiratory lessons yearly, and supported the health maintenance of each patient. We compared COPD medical costs in Matsuura and in the rest of Nagasaki Prefecture using data from 2004 to 2013 recorded by the association of Nagasaki National Health Insurance Organization, assessing 10-year means and annual change.
Results
As of 2014, 256 people have received a definitive diagnosis of COPD; representing 31% of the estimated total number of COPD patients. Of the cases detected, 87.5% were mild or moderate in severity. COPD medical costs per patient in Matsuura were significantly lower than the rest of Nagasaki Prefecture, as was rate of increase in cost over time.
Conclusion
The COPD program in Matsuura enabled early detection and treatment of COPD patients and helped to lower the associated burden of medical costs. The success of this program suggests that a similar program could reduce the economic and human costs of COPD morbidity throughout Japan.
Introduction
COPD involves inflammation of the trachea and real progressive pulmonary destruction caused by long-term exposure to inhaled pollutants such as cigarette smoke. COPD features an accelerating drop in the airflow limitation and in pulmonary function, and it is an increasingly important factor of morbidity and mortality.Citation1,Citation2 By 2020, COPD is predicted to be the third leading cause of death throughout the world.Citation3 In Japan in 2012, COPD was the ninth leading cause of total deaths, and eighth in men; this number increases yearly.Citation4 The increase in COPD patients is predicted to increase as the population ages. In addition, large medical costs are incurred by the deteriorating condition of COPD patients during the progress of the disease.Citation5 Therefore, early detection and early treatment are important for slowing the increase in COPD patients and reducing the related financial burden.
Several reports giving data on the prevalence of COPD have been recently published. The Latin American Project for the Investigation of Obstructive Lung Disease (PLATINO) and Burden of Obstructive Lung Disease (BOLD) initiative studies of COPD prevalence have reported regional differences worldwide.Citation6,Citation7 Prevalences as high as 12% and as low as 7% have recently been reported, with most countries falling in the 7%–9% range.Citation8 The Nippon COPD Epidemiology (NICE) Study found a prevalence of 8.6%.Citation9 The study estimated that at least 5.3 million people in Japan had COPD but found that only approximately 260,000 people (4.9%) were receiving treatment, a very low figure.Citation10 COPD remains underdiagnosed and undertreated worldwide.Citation11,Citation12 The reasons for this include low awareness of COPD,Citation13 the slow spread of spirometry for use in definitive diagnoses,Citation11 and the lack of subjective symptoms in middle-aged male smokers with mild cases of COPD.Citation14 In addition, most COPD epidemiologic studies used data derived from a random sample without directly investigating all inhabitants of the area, are retrospective studies from databases, and use almost entirely cross-sectional techniques.Citation6–Citation9,Citation15,Citation16
COPD requires early detection and early treatment. Therefore improving the recognition of COPD is necessary to increase consultations. In addition, promoting the continuous detection of potential patients and preventing symptomatic exacerbation is important. However, few studies have evaluated the effects of sufficiently long-term interventions.Citation17,Citation18
There are many useful reports about COPD treatment interventions. The treatment of COPD patients with long-acting bronchodilators could alleviate the deterioration of pulmonary function with age,Citation19,Citation20 and studies have indicated that smoking cessation can inhibit decreased pulmonary function.Citation21–Citation24 Many reports have shown that rehabilitation interventions significantly improved COPD patient outcomes.Citation25–Citation27 Early detection and diagnosis of COPD and interventions including medical therapy, smoking cessation, and rehabilitation combine in an attempt to prevent the development and progression of the disease.
Because of the high degree of deterioration in quality of life and the serious economic consequences of COPD, the Japanese Ministry of Health, Labour and Welfare created a comprehensive policy for the prevention and management of COPD known as “Kenko Nihon [Healthy Japan] 21”. However, aside from describing methods of increasing the awareness of COPD, this policy contains no specific strategies.Citation28 As a result, local municipalities have neither specific initiatives to promote the early detection and treatment of COPD, smoking cessation policies, nor initiatives to promote continuous treatment of the disease.
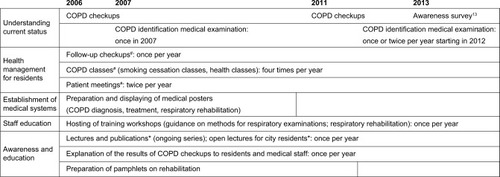
In 2006, we initiated a COPD taskforce in the city of Matsuura in Nagasaki Prefecture and created an original COPD intervention system.Citation13 The taskforce consisted of members of the medical association, the local government, and academia. Members of the public health center, the local government, a local medical association and a university jointly conducted COPD examinations on all inhabitants aged 50 years and older in a single city. A major hospital provided interventions to enable the early diagnosis of patients suspected of having COPD, their family doctors initiated treatment, and public health centers and the university jointly performed follow-up examinations (). In this long-term community-based study implemented by the COPD taskforce, we investigated the effects of cooperation between one city’s hospitals and clinics on case detection rate and on the medical costs of all inhabitants aged 50 years and older, as well as preventative measures including early detection and treatment, continuous treatment, and smoking cessation. To our knowledge, no other study of this kind has been published to date.
Figure 1 Overview of the educational COPD intervention activities.
The aim of this study was to verify the usefulness of the COPD taskforce and intervention.
We investigated the case detection rate and COPD-associated medical costs of all COPD patients diagnosed by this system to date.
Methods
Study design and setting
This study was a community-based longitudinal study of all inhabitants aged 50–89 years in the city of Matsuura, Nagasaki Prefecture (n=8,878 as of September 2006). This study was conducted with the approval of the Human Ethics Review Committee of Nagasaki University Graduate School of Biomedical Sciences (approval number: 1308056). The participants’ data were allocated a code to protect their identities, and all information was kept confidential. All participants provided written consent.
Summary of the COPD taskforce
Creation of the COPD taskforce and education campaign
We established the COPD taskforce in cooperation with the Kita Matsuura Medical Association and the Nagasaki Prefectural Kenhoku Health Center in Matsuura.Citation13 Its objectives were as follows. 1) The early detection and treatment of COPD, and continuous intervention for COPD patients to prevent the progression of COPD. 2) Increasing awareness of COPD to ensure that community inhabitants had a proper understanding of COPD. 3) Creating preventative measures such as smoking cessation programs and policies to prevent people being exposed to tobacco smoke. We developed educational material such as brochures and poster notices about COPD for the medical office in Matsuura to increase COPD recognition, and we held a study session ().
COPD examination and definitive diagnosis and actions for early detection
To efficiently select potential COPD patients from the community, we mailed a self-administered eleven-item pre-interview questionnaire (11-Q) to all inhabitants aged 50–89 years as initial screening.Citation29 The 11-Q consists of eleven items related to respiratory symptoms and disease background.Citation29 It has a high degree of repeatability, sensitivity, and specificity, which suggests it is useful as a screening method for COPD.Citation29 In line with previous studies, we set the cut-off point at 5 points, and patients scoring 5 or more points underwent secondary screening.Citation29
Secondary screening consisted of pulmonary function tests, physical measurements (height, weight, and body mass index), and an interview to determine smoking status and the Brinkman Index (BI). The pulmonary function tests were conducted using an electronic spirometer (Autospiro AS-507; Minato Medical Science Co., Osaka, Japan). Vital capacity (VC), VC predicted, forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), FEV1/FVC, and FEV1 predicted were measured. Measurements were performed according to the American Thoracic Society and European Respiratory Society pulmonary function testing guidelines.Citation30 Those patients whose pulmonary function test results indicated an FEV1/FVC of <0.7 or who reported subjective symptoms during their interview and expressed the desire for a definitive diagnosis were referred to a local foundation hospital where a specialist in pulmonary medicine performed reversibility tests using bronchodilators and computed tomography. COPD examinations were conducted in 2006 and 2011 ().
In addition, we asked each medical office in Matsuura to use a simple interview question during outpatient consultations for the purpose of early COPD detection. We established a COPD examination booth at the medical health checkup and the health festival in 2007 and subsequently provided a booth at these events yearly from 2012 until present (). When attending the booth, the applicants received a pulmonary function test; individuals who tested positive were advised to undergo a complete checkup and were integrated with the COPD patient early detection and treatment system.
Intervention for patients with a definitive diagnosis of COPD
The COPD taskforce conducted follow-ups for patients with a definitive diagnosis of COPD using a system of cooperation between hospitals and clinics. Family doctors played a central role in this system. They cooperated with medical facilities capable of providing a definitive COPD diagnosis, performing respiratory rehabilitation, and accommodating inpatients to provide continuous care. Medical information held by family doctors, cooperating medical facilities, and public health centers was integrated so that COPD patient data could be comprehensively managed.
When indicated, family doctors referred COPD patients to medical facilities capable of providing outpatient smoking cessation services, where the patients received smoking cessation guidance. The system was created so that patients could receive care in accordance with Japanese respiratory society guidelines. Citation31 The contents follow the GOLD COPD guidelines, eg, instruction in smoking cessation is important in Stage I, and the use of the short-acting bronchodilator is recommended for symptom reduction as needed. Improvement of quality of life and exercise tolerance becomes the aim in addition to symptom reduction in Stage II, and a long-acting bronchodilator and pulmonary rehabilitation are recommended. The prevention of exacerbations is important in Stage III and IV, and inhaled corticosteroids are considered in addition to the treatment mentioned above.Citation31 The list of hospitals was advertised in local government offices, hospitals, and the community to inform local inhabitants of the types of care available and the facilities where it was provided. Patients diagnosed with COPD who desired treatment were immediately provided with drug therapy and smoking cessation guidance by their family doctor. Follow-up checkups providing health guidance, pulmonary function tests, and interviews were conducted once per year in cooperation with the university and public health centers ().
In the respiratory classroom, educational courses were held two to four times yearly for patients and their family on topics including COPD pathology, smoking cessation, and pulmonary rehabilitation (including exercise training, upper and lower limb muscular strength exercises, and breathing control). These courses were provided by a doctor, a community health nurse, and a physical therapist. A workshop for the region’s doctors and medical staff was held every year including classes on pulmonary function testing or pulmonary rehabilitation, to ensure the necessary understanding and skill to implement COPD treatment ().
The estimated quantity and prevalence of COPD patients
Based on the number of COPD patients who received a definitive diagnosis, we calculated the estimated number of COPD patients in Matsuura and the prevalence of COPD. The estimated number of COPD patients was calculated by the 11-Q positive rate (the number of respondents with more than five points divided by the number of 11-Q effective respondents) multiplied by the pulmonary function test positive rate (the number of possible COPD cases divided by the number that received a pulmonary function test) multiplied by the COPD diagnosis decision rate (the number of COPD diagnosed divided by the number of possible COPD) divided by the target population.
The COPD prevalence was calculated using the percentage of the estimated number of COPD patients in the target population. Prevalence was also calculated separately for sex, age, and smoking history. We calculated prevalence by smoking history using the BI measured in question 1 of 11-Q.
Medical costs of COPD
To assess the financial benefits, if any, provided by our intervention, the medical costs associated with COPD in each city area in Nagasaki Prefecture were taken from the database of the Nagasaki National Health Insurance Organizations. Data were retrieved covering 10 years spanning 2004 through to 2013. Because of variation in the number of the members of National Health Insurance and in the population of cities, we calculated the COPD medical costs per one National Health Insurance member 50 years or older, and compared costs per patient residing in Matsuura with costs in the rest of Nagasaki Prefecture except Matsuura. In addition, we added the cost for taskforce to the medical cost of Matsuura. We compared a 10-year mean price as well as the annual change in medical costs. Because medical costs are recorded using the location of households, costs are therefore counted accurately and attributed to the correct region.
Statistical analysis
All data were checked for normality using the Shapiro–Wilk test. The comparison of measures of participation in COPD screening examinations was carried out using the chi-square test. We used a Student’s t-test and Mann–Whitney U-test to compare the averages of medical costs and used an analysis of covariance to compare the annual change.
Statistical processing was performed using IBM SPSS Statistics 21.0J for Windows (IBM Corporation, Armonk, NY, USA). Statistical significance was set as a probability of less than 5%.
Results
COPD examination
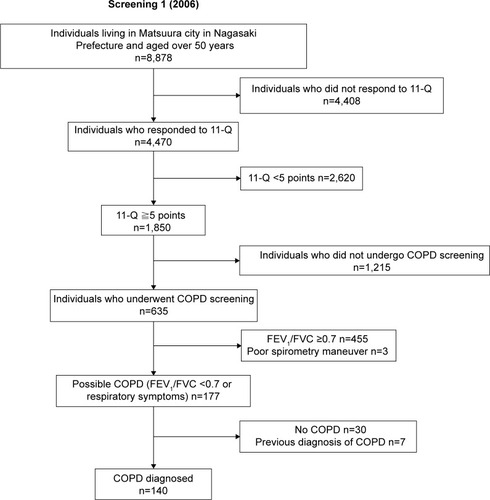
During the COPD examination that we carried out in 2006, 140 people received a definitive diagnosis of COPD (). The initial screening had a low ratio of male participants and individuals in the 50–59 year-old age group. The 50–59 year-old age group also had low participation in the secondary screening. In addition, the answers to 11-Q revealed that many people with some kind of symptom participated, and there was low participation among ex- and current smokers ().
Table 1 Characteristics of the COPD screening target sample
Figure 2 Flowchart of the COPD screening and diagnosis procedure in Matsuura, Japan.
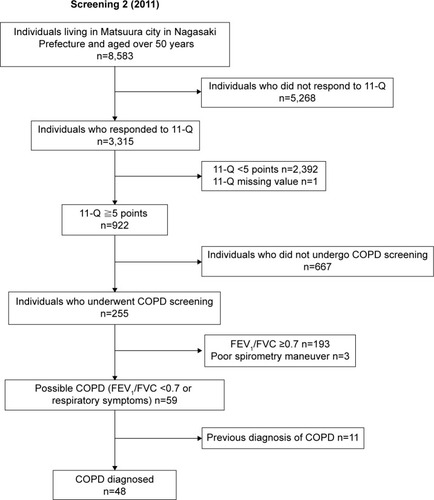
In the COPD examination that we carried out in 2011, 48 COPD patients were newly targeted for follow-up and were registered (). In the first screening, the ratio of participation was low in the youngest generation. Fewer women than men participated in the second screening, and there were no longer differences in reporting of symptoms in the 11-Q or smoking ().
The estimated number and prevalence of COPD patients
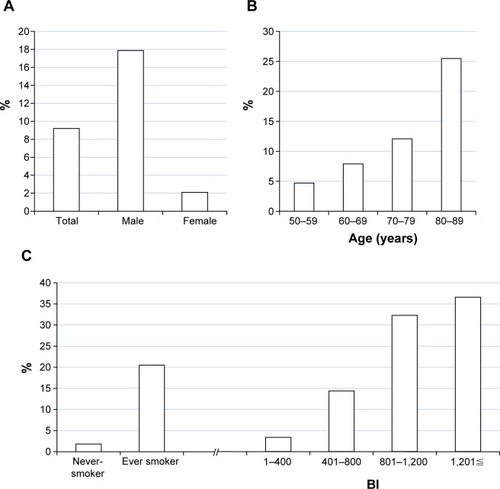
In the 2006 COPD examination, the prevalence was 9.2% (). Of the 814 estimated total COPD patients in Matsuura, we were able to detect 17% in this examination. COPD prevalence by sex was 17.6% in men and 2.1% in women (). The prevalence by age was 4.7% in the 50–59 year-old age group, 7.9% in the 60–69 year-old age group, 12.1% in the 70–79 year-old age group, and 25.5% in the 80+ year-old age group (). The prevalence by smoking status was 1.8% of non-smokers and 20.5% of smokers, and by BI was 3.4% of 1–400, 14.4% of 401–800, 32.3% of 801–1,200, and 36.6% of 1,201 or greater ().
Figure 3 Prevalence of COPD in Matsuura, 2006.
Abbreviation: BI, Brinkman Index.
Progress of the COPD taskforce
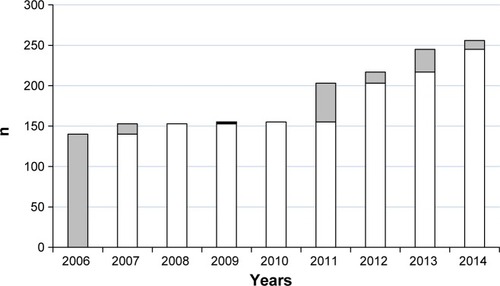
Using data from the database of the Nagasaki National Health Insurance Organizations, an average of eight outpatients consulted the medical institution each month in 2004, and eleven outpatients consulted the medical institution in 2005. After the COPD examination that we carried out in 2006, COPD patients were not identified by the simple outpatient questionnaire implemented by each medical office. However, 13 patients were found by participation in the specific health checkup in 2007. Subsequently, 14 cases of COPD were found at this checkup in 2012, 28 patients in 2013, and eleven patients in 2014. As a result, the number of patients targeted for follow-up increased to 256 in 2014, reaching 31% of the 814 predicted COPD patients in 2006 (). In addition, using the GOLD Stage classification, at the time of follow-up registration, patients at Stages I and II, equal to mild or moderate grade symptoms, comprised 87.5% of the total patients.
Figure 4 Number of newly diagnosed COPD patients each year from 2006 to 2014 in Matsuura.
Medical costs of COPD
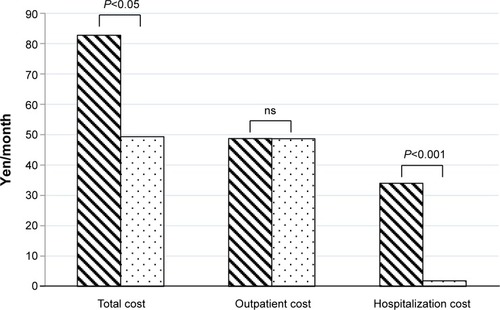
The total costs of the COPD screening in the task-force was 2,240,000 yen for mail and personnel costs. Besides, the annual action needed an average of approximately 400,000 yen. showed a comparison between Matsuura and the rest of Nagasaki Prefecture for the average COPD medical costs in 10 years of one National Health Insurance member 50 years or older. And the data of Matsuura are shown including cost of the taskforce. A Student’s t-test showed that the cost in Matsuura was significantly lower than for the rest of Nagasaki Prefecture (49.3±25.2 yen/month versus [vs] 82.7±37.0 yen/month, P<0.05). There was no significant difference in outpatient medical costs (48.6±24.9 yen/month vs 48.8±19.3 yen/month, P=0.739), but hospitalization costs were significantly lower in Matsuura (1.82±5.8 yen/month vs 34.0±18.9 yen/month, P<0.001).
Figure 5 Comparison of the average cost of medical care for managing COPD in 10 years of one National Health Insurance member aged 50 years or older in Matsuura and in the rest of Nagasaki Prefecture.
Abbreviation: ns, not significant.
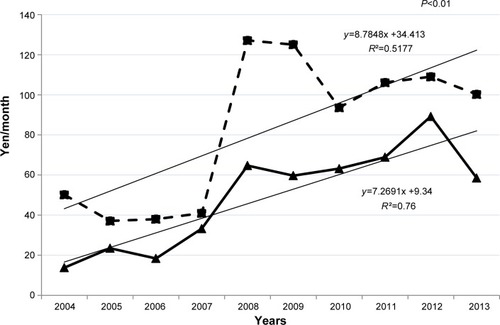
The comparison using analysis of covariance of the annual change of COPD medical costs shows that Matsuura had a significantly lower rate of increase in COPD medical costs than the rest of Nagasaki Prefecture (P<0.01) ().
Figure 6 Comparison of average per capita National Health Insurance cost of COPD medical treatment in Matsuura and the rest of Nagasaki Prefecture in 50–80 year-old patients.
Discussion
By 2014, the COPD taskforce reached and provided care to 31% of the estimated total number of COPD patients calculated at the start of the investigation. Approximately 266,000 people are receiving treatment for COPD in Japan,Citation10 comprising only 5% of the estimated 5.3 million total Japanese COPD patients calculated in the NICE study.Citation9 By comparison, we reached 31% of all COPD patients in one city and provided follow-up education and treatment, while lowering the growth rate of COPD cost-of-care, demonstrating the utility and financial viability of the approach implemented by the COPD taskforce. In addition, we consider it to be very useful that the taskforce was able to enroll 140 patients in primary care at a time in comparison with the consultation number of outpatients before the COPD task-force was implemented.
Many epidemiologic studies have been reported on COPD, including prevalence investigations, but bias occurs in the criteria for selection because these studies do not investigate all inhabitants of the relevant area.Citation6–Citation9 However, in an initial screening investigation using the simple 11-Q interview list, all inhabitants can be surveyed. In addition, there is a low burden on participants because the time required for this simple self-administered questionnaire is only approximately 5 minutes. This study demonstrated the benefit of such a convenient time-efficient screening questionnaire, because the 11-Q response rate was greater than 50%.
Kida et al have reported that a screening examination using a pulmonary function test alongside 11-Q is useful for early detection of COPD in primary care settings.Citation29 Oike et al reported that this combined screening examination was more effective for COPD patient detection than conventional preventative medical examinations in Japan.Citation32 In addition, it has been reported that primary care COPD screening using questionnaires such as the International Primary Care Airways Guidelines questionnaire and the simple expression pulmonary function test device was more useful for patient detection and medical cost reduction than a pulmonary function test.Citation33–Citation36 These reports further indicate the utility of the COPD screening method used in this study.
We developed brochures for medical personnel and the public and held a workshop for medical personnel while providing continuous support for the COPD patients identified in 2006 so that diagnosis and treatment of COPD would be augmented by primary care clinics identifying further COPD patients. However, we did not see a meaningful increase in COPD patients identified by primary care clinics between 2007 and 2010. We believe this is due to the complexity of primary care duties and by time constraints that preclude performing a pulmonary function test.
Consequently, in 2011, we again attempted to identify potential COPD patients through the investigative screening of all residents of Matsuura aged 50 years or older. It was subsequently possible to increase the number of COPD patients enrolled yearly by gathering the participants of the investigation in the event that a lot of participants were more likely to be anticipated. However, there may be the suggestion of an improvement in COPD patient detection in primary care settings in Matsuura, because recently there has been a report on the usefulness of primary care COPD screening and of a pulmonary function test performed by a trained nurse for diagnosing COPD.Citation33–Citation37
The COPD prevalence of 9.2% in all subjects aged 50 years or older is similar to a previous study.Citation8,Citation9 In addition, similar results were found relating to sex, generation, and smoking status, with higher COPD prevalence among smokers, older adults, and men.
During our trial, Matsuura was able to control COPD medical costs, and in particular those derived from hospitalization, when compared with the rest of Nagasaki Prefecture, and it had a significantly lower annual rate of increase in COPD medical costs. A report examining COPD medical costs in Japan found the estimated total cost of COPD to be 805.5 billion yen (US$6.8 billion) per year, including 645.1 billion yen (US$5.5 billion) in direct costs and 160.4 billion yen (US$1.4 billion) in indirect costs.Citation38 COPD brings a high economic burden, and costs associated with hospitalization appear to account for the majority of this burden. Darnell et al reported that costs connected to hospitalization accounted for US$18.7 million out of a total of US$21.4 million in COPD-related medical costs in the Cincinnati Veteran’s Administration Medical Center.Citation39 Breunig et al reported that of the $29.5 billion direct cost of COPD in the United States, the overhead costs were predicted to be $20.4 billion, and a maximum of 70% of the direct costs were caused by hospitalization in conjunction with the exacerbation of COPD symptoms.Citation12 In addition, in the report that examined COPD medical costs by GOLD Stage, there was no significant difference from the control group (non-COPD) for Stage I, but the medical costs were significantly higher than the control group for patients worse than Stage II, and the increase in hospitalization costs was particularly large.Citation40 In the report examining pneumonia among the older adults and the medical costs of COPD, COPD patients had a sixfold greater incidence of pneumonia when compared with patients without COPD, and their medical costs were significantly higher.Citation41
Decreasing hospitalization rates will help to control the medical costs of COPD, and the results of this study are consequently very relevant. Medical costs were kept low because COPD was discovered at an early stage through examination, and early treatment interventions such as smoking cessation were therefore possible. Matsuura was able to slow the progress of COPD and prevent acute exacerbation when compared with other cities. Physician recognition of COPD increased because of an educational course. Therefore we think that the treatment guidelines promoted COPD recognition in primary care. We also believe that the high recognition of COPD among Matsuura inhabitants contributed to the reduced medical costs.Citation13 Because educational activities for local inhabitants, including COPD examination and respiratory lessons, were carried out regularly, understanding of COPD was high and a positive environment was created for commencing treatment. This positive environment increased treatment rates and contributed to the comparatively reduced medical costs. In addition, it is a very important result that the increase in medical costs was lower than in other cities, even though the number of follow-up patients treated in Matsuura increased yearly. This result strongly demonstrates the usefulness of the COPD taskforce.
Limitations of this study include that it applies only to individuals 50 years or older, making it difficult to compare directly with other studies because most previous studies were intended for individuals 40 years or older. In addition, selection bias was introduced because individuals could choose whether to participate in each screening. Matsuura’s COPD patients were detected by examination, but, as for the patients of other cities, COPD was found by medical institution. Thus, lead time bias exists among the COPD patients detected in these two groups. In addition, the data on medical costs use cases where COPD was registered as the primary disease; the COPD frequency among patients registered under other diseases is unknown. Further we are unable to provide data on the total medical costs for each COPD patient because we are unable to determine the medical costs of treatment of other co-morbidities. Also, because COPD prevalence, severity, recognition, demographic, health, and socioeconomic profiles in cities are unidentified and the number of respiratory specialists varies, other factors may have influenced medical costs. Because we did not analyze it in detail, it is not revealed which element of the activity of the taskforce influenced a result.
Our study shows that COPD examination using the simple 11-Q questionnaire for all inhabitants extracted many COPD patients, and we were able to tie this in to early detection and early treatment. In addition, we suggested the possibility that it is possible to control the medical costs of COPD by continuously advancing COPD intervention.
Conclusion
For all inhabitants of Matsuura 50 years or older, COPD screening using the simple 11-Q questionnaire and a subsequent pulmonary function test enabled early detection and early treatment of COPD patients. During this time, Matsuura had a significantly lower increase in COPD-associated expenses than surrounding cities, suggesting that programs such as ours are cost-effective and publicly beneficial interventions that could be implemented throughout Japan.
Author contributions
HS was the principal investigator and contributed to the design of the study, administered the funding, supervised the team’s work, and made critical revisions to the paper for intellectual content. YT designed the study, drafted and revised, collected, analyzed and interpreted the data, and prepared the paper. SH interpreted the data, analyzed the data, handled supervision, and made critical revisions to the paper for important intellectual content. TS contributed toward data analysis and made critical revisions to the paper for important intellectual content. TT, KT, MA, RK, and MT collected and interpreted the data, drafted the manuscript, and made critical revisions to the paper for important intellectual content. All authors read and approved the final paper and agree to be accountable for all aspects of the work.
Acknowledgments
We thank the study participants, the staff of the government of Matsuura district, Nagasaki Prefecture, and Nagasaki National Health Insurance Organization and coworkers for their help. In addition, we are grateful to Dr Sue Jenkins, PhD, Lung Institute of Western Australia, for her help in reviewing our manuscript. This study was supported by the Ministry of Education, Culture, Sports, Science and Technology of Japan and the Environmental Restoration and Conservation Agency, Independent Administrative Institutions of Japan.
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
- Global Initiative for Chronic Obstructive Lung DiseaseGlobal Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Lung Disease UPDATE 2014 Available from: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2014.pdfAccessed November 30, 2014
- RabeKFHurdSAnzuetoSGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2007176653255517507545
- MurrayCJLopezADAlternative projections of mortality and disability by cause 1990–2020 Global Burden of Disease StudyLancet19973499064149815049167458
- Ministry of Health Labour and WelfareLeading causes of death by sexJapanMinistry of Health, Labour and Welfare2013 Available from: http://www.mhlw.go.jp/toukei/saikin/hw/jinkou/kakutei13/dl/10_h6.pdfAccessed November 30, 2014
- AkazawaMHalpernRRiedelAAStanfordRHDalalABlanchetteCMEconomic burden prior to COPD diagnosis: A matched case-control study in the United StatesRespir Med2008102121744175218760581
- MenezesAMPerez-PadillaRJardimJRChronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence studyLancet200536695001875188116310554
- BuistASMcBurnieMAVollmerWMInternational variation in the prevalence of COPD (The BOLD Study): a population-based prevalence studyLancet2007370958974175017765523
- LandisSHMuellerovaHManninoDMContinuing to Confront COPD International Patient Survey: methods, COPD prevalence, and disease burden in 2012–2013Int J Chron Obstruct Pulmon Dis2014959761124944511
- FukuchiYNishimuraMIchinoseMCOPD in Japan: The Nippon COPD epidemiology studyRespirology20049445846515612956
- Ministry of Health, Labour and Welfare [homepage on the Internet]The total number of patients (the patient address ground), sex age-grade, sickness and wound classification, metropolis and districts distinction (nationwide)Patient survey2011:file 147-1 Available from: http://www.e-stat.go.jp/SG1/estat/GL08020103.do?_toGL08020103_&listID=000001103075&requestSender=dsearchAccessed November 30, 2014 Japanese
- TakahashiTIchinoseMInoueHShiratoKHattoriTTakishimaTUnderdiagnosis and undertreatment of COPD in primary care settingsRespirology20038450450814629656
- BreunigIMShayaFTScharfSMDelivering cost-effective care for COPD in the USA: recent progress and current challengesExpert Rev Pharmacoecon Outcomes Res201212672573123252355
- AsaiMTanakaTKozuREffect of a COPD Intervention on COPD Awareness in a Regional City in JapanIntern Med201554216316925743007
- GeijerRMSachsAPVerheijTJLammersJWSaloméPLHoesAWAre patient characteristics helpful in recognizing mild COPD (GOLD I) in daily practice?Scand J Prim Health Care200624423724217118864
- MüllerováHLuCLiHTabbererMPrevalence and burden of breathlessness in patients with chronic obstructive pulmonary disease managed in primary carePLoS One201491e8554024427316
- BurneyPJithooAKatoBChronic obstructive pulmonary disease mortality and prevalence: the associations with smoking and poverty – a BOLD analysisThorax201469546547324353008
- KinnulaVLVasankariTKontulaESovijarviASaynajakangasOPietinalhoAThe 10-year COPD Programme in Finland: effects on quality of diagnosis, smoking, prevalence, hospital admissions and mortalityPrim Care Respir J201120217818321431275
- ZhouYHuGWangDCommunity based integrated intervention for prevention and management of chronic obstructive pulmonary disease (COPD) in Guangdong, China: cluster randomised controlled trialBMJ2010341c638721123342
- DecramerMCelliBKestenSEffect of tiotropium on outcomes in patients with moderate chronic obstructive pulmonary disease (UPLIFT): a prespecified subgroup analysis of a randomised controlled trialLancet200937496961171117819716598
- VogelmeierCHedererBGlaabTTiotropium versus salmeterol for the prevention of exacerbations of COPDN Engl J Med2011364121093110321428765
- AnthonisenNRConnettJEKileyJPEffects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health StudyJAMA199427219149715057966841
- CamilliAEBurrowsBKnudsonRJLyleSKLebowitzMDLongitudinal changes in forced expiratory volume in one second in adults. Effects of smoking and smoking cessationAm Rev Respir Dis198713547947993565927
- HigginsMWEnrightPLKronmalRASchenkerMBAnton-CulverHLylesMSmoking and lung function in elderly men and women. The Cardiovascular Health StudyJAMA199326921274127488492399
- WarnierMJvan RietEERuttenFHDe BruinMLSachsAPSmoking cessation strategies in patients with COPDEur Respir J201341372773422936706
- BerryMJRejeskiWJAdairNEZaccaroDExercise rehabilitation and chronic obstructive pulmonary disease stageAm J Respir Crit Care Med199916041248125310508815
- FogioKBianchiLBrulettiGBattistaLPaganiMAmbrosinoNLong-term effectiveness of pulmonary rehabilitation in patients with chronic airway obstructionEur Respir J199913112513210836336
- MaltaisFBourbeauJShapiroSEffects of home-based pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: a randomized trialAnn Intern Med20081491286987819075206
- KomiyamaYMinisterial Notification No 430 of the Ministry of Health, Labour and WelfareKenko Nihon [Healthy Japan] 21Second edition2013 Available from: http://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/0000047330.pdfAccessed November 30, 2014
- KidaKWakabayashiRMizuuchiTMurataAScreening for suspected chronic obstructive pulmonary disease with an eleven-item pre-interview questionnaire (11-Q)Intern Med200645211201120717139118
- MillerMRHankinsonJBrusascoVStandardisation of spirometryEur Respir J200526215316115994402
- Japanese Respiratory Society COPD Guideline 2nd edition making committeeChronic Obstructive Pulmonary Disease – Guideline for a Diagnosis and Treatment2nd edOsakaMedical Review Co., Ltd2004 Japanese
- OikeTSenjyuHHigaNDetection of Airflow Limitation Using the 11-Q and Pulmonary Function TestsIntern Med201352888789323583992
- SichletidisLSpyratosaDPapaioannouMA combination of the IPAG questionnaire and PiKo-6R flow meter is a valuable screening tool for COPD in the primary care settingPrim Care Respir J201120218418921597666
- ThornJTillingBLisspersKJörgensenLStenlingAStratelisGImproved prediction of COPD in at-risk patients using lung function pre-screening in primary care: a real-life study and cost-effectiveness analysisPrim Care Respir J201221215916622270480
- Franco-MarinaFFernandez-PlataRTorre-BouscouletLEfficient screening for COPD using three steps: a cross-sectional study in Mexico CityNPJ Prim Care Respir Med2014241400224841708
- YawnBPDuvallKPeabodyJThe impact of screening tools on diagnosis of chronic obstructive pulmonary disease in primary careAm J Prev Med201447556357525241196
- WaltersJAHansenECJohnsDPBlizzardELWaltersEHWood-BakerRA mixed methods study to compare models of spirometry delivery in primary care for patients at risk of COPDThorax200863540841418024537
- NishimuraSZaherCCost impact of COPD in Japan: Opportunities and challenges?Respirology20049446647315612957
- DarnellKDwivediAKWengZPanosRJDisproportionate utilization of healthcare resources among veterans with COPD: a retrospective analysis of factors associated with COPD healthcare costCost Eff Resour Alloc2013111323763761
- MennPHeinrichJHuberRMDirect medical costs of COPD – An excess cost approach based on two population-based studiesRespir Med2012106454054822100535
- RyanMSuayaJAChapmanJDStasonWBShepardDSThomasCPIncidence and Cost of Pneumonia in Older Adults with COPD in the United StatesPLoS One2013810e7588724130749