
Abstract
Background
A new approach to the treatment of COPD includes controlling inflammation because of its important role in exacerbation of the disease. Recently, roflumilast has been added as a therapeutic option for COPD. Roflumilast is an oral phosphodiesterase-4 inhibitor that targets inflammatory cells involved in triggering exacerbations of COPD. The objective of the current study was to evaluate roflumilast for its contribution to phagocytic activity in COPD patients.
Methods
Twenty-one patients diagnosed with COPD received roflumilast once daily for 6 months in combination with fluticasone (an inhaled corticosteroid), salmeterol (a long-acting β2-agonist), and tiotropium (a long-acting muscarinic antagonist) or combinations of these agents. The main inclusion criterion was stable disease for at least the previous 30 days. Neutrophils and spirometric changes, ie, forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC), were measured in the COPD patients at indicated time points. The first sample was taken before receiving roflumilast, the second 3 months later, and the third after 6 months. Examination of defective phagocytosis was done by flow cytometry using a FagoFlowEx® kit. The statistical analysis was performed using Statistica software.
Results
Our results indicate that phagocytic activity was increased after 3 and 6 months of treatment when compared with baseline (P<0.001). Similarly, FVC and FEV1 were also increased during the 6-month period, but only FVC differed significantly from baseline (P<0.001).
Conclusion
Although the number of patients in this study was limited, our results indicate that roflumilast induces phagocytic activity, which improves lung function.
Introduction
COPD is a chronic inflammatory disease affecting the lungs. Cigarette smoking is the most important risk factor, although smoke derived from burning biomass fuels is also a predisposing factor in developing countries.Citation1,Citation2
Diagnosis of COPD is confirmed by spirometry, ie, a post-bronchodilator forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC, Tiffeneau index) of 0.7. COPD is referred to as severe when the FEV1 is 50%–30% and very severe when it is <30% of the predicted value.Citation3 Recent global guidelines for the management of COPD recommend grouping patients into four groups labeled A, B, C, or D according to symptoms (classified as “less” and “more”), air flow limitation (classified as “mild”, “moderate”, “severe”, and “very severe”, Global Initiative for Chronic Obstructive Lung Disease stages 1–4 respectively), risk of exacerbation (classified as “low” [≤1 exacerbation per year] and “high” [≥2 exacerbations per year]), and the presence of comorbidities.Citation4
Typical pathological changes in COPD include destruction of the lung parenchyma, eg, emphysema and obstructive bronchiolitis, characterized functionally by progressive airway obstruction. Chronic cough and hypersecretion of mucus may also occur due to inflammatory changes and hyperplasia of the mucous glands in the larger airways.Citation5 The clinical course of COPD is characterized by acute exacerbations accompanied by acute deterioration in lung function and worsening disability.Citation6
The predominant inflammatory cells in COPD are CD68 macrophages and CD8 T-lymphocytes, with polymorphs increasing during acute exacerbations. The severity of inflammation increases during worsening of COPD, resulting in luminal narrowing, parenchymal destruction, and diminishing elastic recoil. The activated macrophages release inflammation mediators and chemotactic factors, including proinflammatory cytokines such as tumor necrosis factor-alpha and interleukin (IL)-6, IL-8, monocyte chemotactic peptide-1, leukotriene B4, and reactive oxygen species, and secrete proteolytic enzymes, in particular matrix metalloproteinases 9 and 12.Citation7 Neutrophils move directly to the respiratory tract under the influence of secreted chemotactic factors (particularly IL-8 and leukotriene B4) and cause overstimulation of submucosal mucous glands and goblet cells by proteinases, especially neutrophil elastase, cathepsin-G, and proteinase-3.Citation8
Although care of COPD has improved over the last decade,Citation9 there is still a huge unmet burden of disease. Exacerbations in particular can be distressing for patientsCitation10 and have serious consequences with regard to their long-term health, such as increased disease progression,Citation11 increased risk of cardiovascular events,Citation12 and increased mortality rates.Citation13,Citation14
In clinical practice, patients still suffering from frequent exacerbations may already be treated with a combination of a long-acting β2-agonist (LABA) and inhaled corticosteroids (ICS), often in addition to tiotropium (a long-acting muscarinic antagonist [LAMA]). Despite the wide variety of pharmacological treatments currently available for COPD, they are insufficient to prevent exacerbations in a number of patients with severe to very severe disease. Since frequent exacerbations are associated with a high level of inflammation,Citation15,Citation16 it is logical to add an anti-inflammatory therapy to combination treatment in order to further reduce the risk of exacerbation.
Roflumilast is an oral phosphodiesterase (PDE)-4 inhibitor that targets inflammatory cells involved in triggering exacerbations of COPD. It is the only PDE-4 inhibitor approved by the US Food and Drug Administration and is available in 500 μg tablets for once-daily administration. It is catalyzed by cytochrome P450 1A2 and 3A4 to its active metabolite, roflumilast N-oxide, which is responsible for >90% of the total PDE-4 inhibitory activity of roflumilast.Citation17
Eleven distinct PDE families have been identified, although most of the anti-inflammatory activity is believed to result from inhibition of PDE-4, for which there is clinical correlation. Three critical findings contributed to the rationale for developing selective PDE-4 inhibitors. First, PDE-4 regulates degradation of 3′5′-cyclic adenosine monophosphate in most immune and proinflammatory cells; second, in cell-based systems, PDE-4 inhibitors of varied structural classes suppress a plethora of responses that are considered to be proinflammatory; and third, PDE-4 inhibitors are efficacious in preclinical animal models that attempt to reproduce specific facets of the pathobiology of COPD.Citation18 Further, PDE-4 inhibitors ameliorate the activity of various inflammatory cells in vitroCitation19 and reduces pulmonary inflammation in complex in vivo animal models.Citation20,Citation21 Specifically, the pathobiological aspects of COPD where PDE-4 inhibitors are efficacious have been reported in: in vitro studies, such as decreased apoptosis (which may result in clearance of sputum), decreased release of cytokines in many cell types and release of inflammatory mediators in neutrophils;Citation22 in vivo studies, such as inhibition of cell trafficking, and release of cytokines and chemokines from inflammatory cells such as neutrophils, eosinophils, macrophages, and T-cells;Citation23 and in animal models, such as decreased accumulation of neutrophils in bronchoalveolar lavage fluid or abolition of the influx of inflammatory cells into the lung parenchyma.Citation24
Clinical trials have already demonstrated the ability of roflumilast to decrease the frequency of exacerbations and improve lung function in COPD,Citation25,Citation26 while its biological action may result potentially in targeting of the inflammatory processes underlying COPD. Thus, it is recognized that the inflammatory response of the lungs is an important field of research necessary for understanding the disease process and for subsequent development of novel therapies for COPD.
Given that the inflammatory infiltrate found in the airway lumen in patients with COPD consists mainly of neutrophils,Citation27 the objective of this open-label study was to evaluate roflumilast, a PDE-4 inhibitor, for its contribution to the phagocytic activity of neutrophils in patients with COPD and its therapeutic potential in terms of diminishing the inflammatory response associated with the disease. Thus, our hypothesis was that addition of an anti-inflammatory regimen such as roflumilast in patients who experience frequent exacerbations would have a beneficial influence on lung function and exacerbations.
Materials and methods
Ethics
Our study was approved by the investigational review board of G Papanikolaou General Hospital, Thessaloniki, Greece.
Treatment regimens
In our study, roflumilast was administered to COPD patients as 500 μg tablets once daily in addition to other COPD treatments, including fluticasone (an ICS), salmeterol (an LABA), and tiotropium (an LAMA).
Patients
Twenty-one patients diagnosed with severe or very severe COPD (groups C and D) with a bronchitis phenotype received roflumilast once daily for 6 months or more in combination with other COPD treatments (including an LABA + ICS + LAMA or an LABA + ICS; ). Entry criteria of patients included stable disease for at least 30 days. All patients had a history of one or two exacerbations during the previous year, but none were recovering from an acute exacerbation. All patients were ex-smokers and, to the best of our knowledge, no patient was smoking during the study period.
Table 1 Patient characteristics
Spirometry
FEV1 and FVC were measured at indicated time points, ie, baseline, 3 months, and 6 months.
Samples
Peripheral blood samples were taken from the COPD patients at the indicated time points. The first sample was taken before receiving roflumilast, the second after 3 months, and the third after 6 months of treatment.
Flow cytometry
Examination of phagocytosis was done by flow cytometry using the FagoFlowEx® kit (Exbio Diagnostics, Ramona, CA, USA). This kit enables examination of the phagocytic activity of granulocytes in heparinized whole blood by measuring the respiratory (oxidative) burst after their stimulation with inactive Escherichia coli bacteria.
Statistical analysis
The statistical analysis was performed using Statistica software (StatSoft Inc., Tulsa, OK, USA). Means calculated from statistically significant factors were examined for potential differences between factor levels by comparing their 95% confidence intervals based on the pooled standard error of analysis of variance. Intervals that do not overlap indicate means that differ significantly from each other. In all statistical analyses, the 0.05 probability level of significance was chosen as the level of reference.
Results
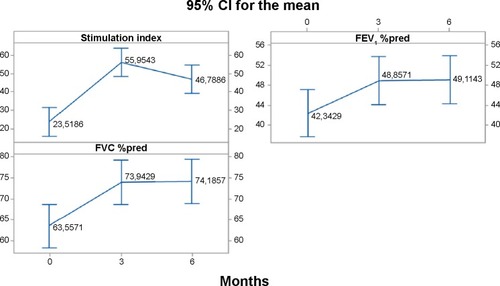
Our results indicate that phagocytic activity was increased during the 6-month treatment period when compared with the first sample. The mean dependence of phagocytic activity before receiving roflumilast differs significantly from the rest periods, since the 95% confidence intervals do not overlap, bringing out a particular pattern of change (0<3, 3>6; ). Similarly, FVC and FEV1 values were also increased at the 3-month and 6-month time points when compared with the first sample. However, only FVC values differed significantly. The mean dependence of FVC values before receiving roflumilast differed significantly from the rest periods (P<0.001, ).
Table 2 P-values from statistical analysis
Figure 1 Mean change in stimulation index for phagocytic activity, FEV1 %pred, FVC %pred, per indicated periods (0, before receiving roflumilast, and 3 months and 6 months after).
Abbreviations: CI, confidence interval; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; %pred, percent predicted.
Discussion
The last Global Initiative for Chronic Obstructive Lung Disease publication recommended a new staging system that contains the frequency of exacerbations,Citation4 and treatment recommendations are made taking into account the group into which the patient falls.
In 2010, roflumilast, a selective PDE-4 inhibitor with anti-inflammatory properties, was approved by the European Medicines Agency for use as once-daily oral maintenance treatment for adult patients with severe or very severe COPD associated with chronic bronchitis and a history of frequent exacerbations, as an add-on to bronchodilators. The hypothesis was that roflumilast provides a large benefit to a subset of COPD patients due to its ability to block activation of inflammatory cells. In our study, phagocytic activity was increased, and this anti-inflammatory effect may in part explain the concomitant improvement in spirometry values, as indicated by our results. Neutrophils play a central role in COPD, and their accumulation and degranulation are associated with tissue damage, increased inflammation, and disordered tissue repair. In particular, the effect of roflumilast on neutrophils is possibly due to the increase in intracellular 3′5′-cyclic adenosine monophosphate attributable to PDE-4 inhibition.Citation28 Furthermore, PDE inhibitors decrease neutrophil damage.Citation29
Until recently, it was assumed that the activity and function of neutrophils was a response to the presence of high levels of inflammation in the lung. However, more recent studies of neutrophil function (including migration, generation of reactive oxygen species, degranulation, phagocytosis, and extracellular trap production) suggest that there is a general impairment of neutrophil responses in COPD that predisposes to increased inflammation and reduced clearance of bacteria.Citation1 This could be very useful for restoring some key neutrophil responses in COPD. Targeting neutrophil intracellular signaling might improve disease outcomes by reducing the extraneous inflammatory burden.
In our study, the FVC in COPD patients was increased significantly in the first 3 months after starting roflumilast in combination with other therapy regimens, such as LABA + ICS + LAMA and LABA + ICS. FEV1 was not significantly improved. This is possibly due to the limited number of patients in our study or perhaps due to the short time period examined. Our results also show that FVC and FEV1 values not only increased during the first 3 months but also remained stable during the following 3 months (). These findings are in accordance with several other studies.Citation29,Citation30 PDE-4 inhibition by roflumilast treatment for 4 weeks improved post-bronchodilator FEV1, and at the same time resulted in an anti-inflammatory effect whereby the numbers of neutrophils and eosinophils were reduced, as well as soluble markers of neutrophilic and eosinophilic inflammatory activity in induced sputum samples of patients with COPD.Citation30
Other clinical investigators have reported similar results. Treatment with a PDE-4 inhibitor was associated with a significant improvement in FEV1 over the trial period compared with placebo in patients with COPD (15 trials, 12,654 patients).Citation31 Similarly, in clinical trials of Asian COPD patients, roflumilast provided a sustained increase in mean prebronchodilator and post-bronchodilator FEV1 and in prebronchodilator and post-bronchodilator FVC when compared with placebo.Citation32,Citation33 The investigators concluded that roflumilast is an optimal treatment choice for patients with severe to very severe COPD. In another study (n=3,091), roflumilast reduced exacerbation rates and improved lung function in patients with COPD who received a concomitant LABA, regardless of prior ICS use, and across various patient subgroups regardless of age and smoking status.Citation34 In a meta-analysis of eleven trials involving 9,675 patients, roflumilast significantly reduced the mean exacerbation rate (mild, moderate, or severe) and improved trough FEV1, FVC, and other post-bronchodilator spirometric parameters.Citation35 In six placebo-controlled trials involving nearly 4,500 patients with COPD of varying severity, use of roflumilast was associated with reduced COPD exacerbations and improved lung function, as determined by spirometry, with the greatest benefits observed in patients with severe COPD who had chronic bronchitis and a history of frequent exacerbations; clinical efficacy was demonstrated in patients receiving roflumilast alone and in those receiving LABA therapy.Citation36
There has been a number of reports concerning the adverse effects of roflumilast. In clinical trials, the most common adverse events reported were diarrhea, nausea, and headache. Weight loss and an increased risk of psychiatric events have also been reported in association with roflumilast. In our study, six (28%) patients reported diarrhea and four (19%) reported headache, but no patient wished to be withdrawn from treatment with roflumilast.
Management of stable COPD should focus on reducing the patient’s future risk of disease progression (determined primarily by exacerbation frequency).Citation37 We should also take into account systemic inflammation as the biological link in combination with exacerbations for evaluation of COPD severity. According to the guidelines, use of combinations of all these treatments is recommended when the severity of COPD increases.Citation3 However, until now, no therapy has been shown to treat the underlying inflammation found in COPD.
To the best of our knowledge, this is the first study in which phagocytic activity was measured in COPD patients receiving roflumilast. A limitation of our study is the small number of patients included; however, our study is an ongoing pilot trial. Future studies should include biomarkers of systemic inflammation and cytokines, and will shed more light on improvement in lung function and reduction of exacerbations.
In conclusion, in our study, treatment with roflumilast induced phagocytic activity which improved lung function. We should view COPD as a preventable and treatable disease. As roflumilast has novel anti-inflammatory activity in COPD, it provides the physician with a treatment option beyond bronchodilation. Although this was a small study, the anti-inflammatory activity of roflumilast was shown to provide incremental benefits on top of existing therapies. Future randomized studies will further confirm the impact of roflumilast on COPD.
Disclosure
An abstract of this paper appeared in a supplement to the Journal of Thoracic Disease containing abstracts presented at the Pan Hellenic Congress on COPD in 2014. Otherwise, the authors report no conflicts of interest in this work.
References
- StockleyJAWaltonGMLordJMSapeyEAberrant neutrophil functions in stable chronic obstructive pulmonary disease: the neutrophil as an immunotherapeutic targetInt Immunopharmacol20131741211121723994347
- FujimotoKUp-to-date COPD treatmentRinsho Byori2014625471477 Japanese25051662
- GelsominoFFacchinettiFHaspingerERTargeting the MET gene for the treatment of non-small-cell lung cancerCrit Rev Oncol Hematol201489228429924355409
- Global Strategy for the Diagnosis, Management, and Prevention of COPDGlobal Initiative for Chronic Obstructive Lung Disease (GOLD) 2015 Available from: http://www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.htmlAccessed May 19, 2015
- AngelisNPorpodisKZarogoulidisPAirway inflammation in chronic obstructive pulmonary diseaseJ Thorac Dis20146Suppl 1S167S17224672691
- BarnesPJThe cytokine network in chronic obstructive pulmonary diseaseAm J Respir Cell Mol Biol200941663163819717810
- BarnesPJShapiroSDPauwelsRAChronic obstructive pulmonary disease: molecular and cellular mechanismsEur Respir J200322467268814582923
- SommerhoffCPNadelJABasbaumCBCaugheyGHNeutrophil elastase and cathepsin G stimulate secretion from cultured bovine airway gland serous cellsJ Clin Invest19908536826892107207
- AlmagroPSalvadoMGarcia-VidalCRecent improvement in long-term survival after a COPD hospitalisationThorax201065429830220388752
- KesslerRStahlEVogelmeierCPatient understanding, detection, and experience of COPD exacerbations: an observational, interview-based studyChest2006130113314216840393
- DecramerMCooperCBTreatment of COPD: the sooner the better?Thorax201065983784120805184
- DonaldsonGCHurstJRSmithCJHubbardRBWedzichaJAIncreased risk of myocardial infarction and stroke following exacerbation of COPDChest201013751091109720022970
- WedzichaJASeemungalTACOPD exacerbations: defining their cause and preventionLancet2007370958978679617765528
- Soler-CatalunaJJMartinez-GarciaMARoman SanchezPSalcedoENavarroMOchandoRSevere acute exacerbations and mortality in patients with chronic obstructive pulmonary diseaseThorax2005601192593116055622
- PereraWRHurstJRWilkinsonTMInflammatory changes, recovery and recurrence at COPD exacerbationEur Respir J200729352753417107990
- BhowmikASeemungalTASapsfordRJWedzichaJARelation of sputum inflammatory markers to symptoms and lung function changes in COPD exacerbationsThorax200055211412010639527
- LahuGNassrNHunnemeyerAPharmacokinetic evaluation of roflumilastExpert Opin Drug Metab Toxicol20117121577159122059647
- HoggJCChuFUtokaparchSThe nature of small-airway obstruction in chronic obstructive pulmonary diseaseN Engl J Med2004350262645265315215480
- HatzelmannASchudtCAnti-inflammatory and immunomodulatory potential of the novel PDE4 inhibitor roflumilast in vitroJ Pharmacol Exp Ther2001297126727911259554
- BundschuhDSEltzeMBarsigJWollinLHatzelmannABeumeRIn vivo efficacy in airway disease models of roflumilast, a novel orally active PDE4 inhibitorJ Pharmacol Exp Ther2001297128029011259555
- WollinLBundschuhDSWohlsenAMarxDBeumeRInhibition of airway hyperresponsiveness and pulmonary inflammation by roflumilast and other PDE4 inhibitorsPulm Pharmacol Ther200619534335216257550
- HatzelmannAMorcilloEJLungarellaGThe preclinical pharmacology of roflumilast – a selective, oral phosphodiesterase 4 inhibitor in development for chronic obstructive pulmonary diseasePulm Pharmacol Ther201023423525620381629
- SanzMJCortijoJMorcilloEJPDE4 inhibitors as new anti-inflammatory drugs: effects on cell trafficking and cell adhesion molecules expressionPharmacol Ther2005106326929715922015
- Le QuementCGuenonIGillonJYThe selective MMP-12 inhibitor, AS111793 reduces airway inflammation in mice exposed to cigarette smokeBr J Pharmacol200815461206121518493250
- CalverleyPMRabeKFGoehringUMKristiansenSFabbriLMMartinezFJRoflumilast in symptomatic chronic obstructive pulmonary disease: two randomised clinical trialsLancet2009374969168569419716960
- FabbriLMCalverleyPMIzquierdo-AlonsoJLRoflumilast in moderate-to-severe chronic obstructive pulmonary disease treated with longacting bronchodilators: two randomised clinical trialsLancet2009374969169570319716961
- KeatingsVMBarnesPJGranulocyte activation markers in induced sputum: comparison between chronic obstructive pulmonary disease, asthma, and normal subjectsAm J Respir Crit Care Med199715524494539032177
- CastroAJerezMJGilCMartinezACyclic nucleotide phosphodiesterases and their role in immunomodulatory responses: advances in the development of specific phosphodiesterase inhibitorsMed Res Rev200525222924415514991
- EssayanDMCyclic nucleotide phosphodiesterase (PDE) inhibitors and immunomodulationBiochem Pharmacol199957996597310796066
- GrootendorstDCGauwSAVerhooselRMReduction in sputum neutrophil and eosinophil numbers by the PDE4 inhibitor roflumilast in patients with COPDThorax200762121081108717573446
- ChongJLeungBPoolePPhosphodiesterase 4 inhibitors for chronic obstructive pulmonary diseaseCochrane Database Syst Rev201311CD00230924190161
- ZhengJYangJZhouXRoflumilast for the treatment of COPD in an Asian population: a randomized, double-blind, parallel-group studyChest20141451445224135893
- ChoiDRLeeDHChoiCMKimSWSuhCLeeJSErlotinib in first-line therapy for non-small cell lung cancer: a prospective phase II studyAnticancer Res201131103457346221965761
- HananiaNACalverleyPMDransfieldMTPooled subpopulation analyses of the effects of roflumilast on exacerbations and lung function in COPDRespir Med2014108236637524120253
- YanJHGuWJPanLEfficacy and safety of roflumilast in patients with stable chronic obstructive pulmonary disease: a meta-analysisPulm Pharmacol Ther2014271838923624309
- LipariMBenipalHKale-PradhanPRoflumilast in the management of chronic obstructive pulmonary diseaseAm J Health Syst Pharm201370232087209524249758
- PostmaDAnzuetoACalverleyPA new perspective on optimal care for patients with COPDPrim Care Respir J201120220520921559550